Z-Shaped Calcaneal Osteotomy: Comprehensive Surgical Guide
Key Takeaway
The Z-shaped calcaneal osteotomy, pioneered by Knupp et al., is a powerful step-cut technique designed for three-plane correction of severe varus hindfoot deformities. By allowing simultaneous multiplanar translation and angulation of the calcaneal tuberosity, this procedure effectively addresses rigid hindfoot varus, forefoot valgus, and plantarflexed first ray deformities while preserving joint congruity. Proper execution requires meticulous soft tissue handling and precise osteotomy cuts to optimize biomechanical realignment.
Introduction to the Z-Shaped Calcaneal Osteotomy
The management of severe, rigid hindfoot varus deformities presents a complex biomechanical challenge for the orthopaedic foot and ankle surgeon. Traditional osteotomies, such as the lateral closing wedge (Dwyer) or simple sliding calcaneal osteotomies, often fall short in providing adequate multiplanar correction without compromising the structural integrity or length of the calcaneus.
To address these limitations, Knupp, Horisberger, and Hintermann described an innovative procedure utilizing a step-cut (scarf-like) osteotomy. Known as the Z-shaped calcaneal osteotomy, this technique allows for powerful, simultaneous correction of the heel in both the frontal and transverse planes, with the added ability to modulate sagittal plane alignment. By translating and angulating the posterior tuberosity, surgeons can effectively restore the mechanical axis of the hindfoot, converting the deforming force of the Achilles tendon from an invertor to an evertor.
This comprehensive guide details the indications, biomechanical rationale, preoperative assessment, and step-by-step surgical execution of the Z-shaped calcaneal osteotomy, providing a masterclass for orthopaedic residents, fellows, and practicing consultants.
Biomechanical Principles and Rationale
The Z-shaped calcaneal osteotomy is fundamentally a three-dimensional corrective procedure. The step-cut design provides a broad surface area for bony healing while allowing the posterior calcaneal tuberosity to be manipulated in multiple planes:
- Frontal Plane (Valgus Correction): Lateral translation of the tuberosity shifts the weight-bearing axis laterally, correcting the varus thrust.
- Transverse Plane (Abduction/Adduction): The tuberosity can be rotated to correct internal or external rotation deformities of the heel.
- Sagittal Plane (Lengthening/Shortening): By sliding the tuberosity posteriorly along the horizontal cut, the calcaneus can be lengthened, which is particularly useful in cavovarus feet with a shortened lateral column.
Clinical Pearl: Lateralizing the calcaneal tuberosity alters the lever arm of the Achilles tendon. In a varus hindfoot, the Achilles acts as a paradoxical invertor. Post-osteotomy, the lateralized insertion restores the tendon's normal eversion moment, dynamically stabilizing the hindfoot during the gait cycle.
Indications and Patient Selection
Careful patient selection is paramount. The Z-shaped calcaneal osteotomy is primarily indicated for complex, multiplanar deformities where joint-sparing correction is desired.
Primary Indications
- Rigid Varus Hindfoot: Combined with forefoot valgus and an excessively plantarflexed first ray (classic cavovarus foot).
- Metatarsus Primus Flexus: Osteotomy of the calcaneus is necessary if the varus deformity is driven by a rigid metatarsus primus flexus, even without a primary rigid hindfoot deformity. The hindfoot varus, initially compensatory, often becomes structurally adapted.
- Neurological Cavovarus: Secondary to conditions such as Charcot-Marie-Tooth (CMT) disease, provided the subtalar joint remains free of advanced arthrosis.
Contraindications
- Degenerative Joint Disease: Advanced osteoarthritis of the subtalar or transverse tarsal joints is an absolute contraindication. These patients are better served by corrective arthrodesis (e.g., subtalar or triple arthrodesis).
- Tarsal Coalitions: Rigid deformities secondary to untreated coalitions that preclude joint-sparing realignment.
- Severe Vascular Compromise: Peripheral arterial disease that threatens wound healing over the lateral calcaneal wall.
- Active Infection: Local or systemic.
Surgical Warning: A thorough neurological assessment must be performed preoperatively. If Charcot-Marie-Tooth (CMT) disease or another progressive neuropathy is suspected, the surgeon must anticipate the need for concomitant soft-tissue balancing, such as peroneus longus to peroneus brevis tendon transfers, or plantar fascia release, to address the excessively pronated forefoot and plantarflexed first ray.
Preoperative Clinical and Radiographic Assessment
Clinical Evaluation
The clinical exam must differentiate between flexible and rigid deformities. The Coleman Block Test is essential; it eliminates the influence of a plantarflexed first ray on the hindfoot. If the hindfoot corrects to neutral or valgus on the block, the deformity is forefoot-driven. If the hindfoot remains in varus, the deformity is rigid, and a calcaneal osteotomy is mandated.
Radiographic Imaging
Standard weight-bearing radiographs are required:
* Anteroposterior (AP) and Lateral Foot: To assess the Meary's angle, calcaneal pitch, and talocalcaneal angles.
* Hindfoot Alignment View (Saltzman View): Critical for quantifying the degree of varus offset of the calcaneal tuberosity relative to the tibial axis.
* CT/MRI: May be indicated to rule out subtalar arthrosis or tarsal coalitions if the clinical exam reveals unexpected rigidity or pain out of proportion to the deformity.
Surgical Technique: The Knupp et al. Approach (Technique 86-17)
The following step-by-step technique outlines the precise execution of the Z-shaped calcaneal osteotomy.
1. Patient Positioning and Preparation
- Place the patient in the supine position on the operating table.
- Place a large sandbag or gel bump under the ipsilateral buttock. This internally rotates the leg, bringing the lateral aspect of the hindfoot forward and parallel to the floor, optimizing the surgical trajectory.
- Apply a well-padded thigh tourniquet.
- Exsanguinate the limb and inflate the tourniquet to the standard pressure (typically 250-300 mmHg).
- Administer prophylactic intravenous antibiotics prior to tourniquet inflation.
2. Incision and Soft Tissue Exposure
- Make a slightly curved, L-shaped or extensile lateral incision. The incision should run parallel to and approximately 1 cm posterior to the peroneus longus tendon.
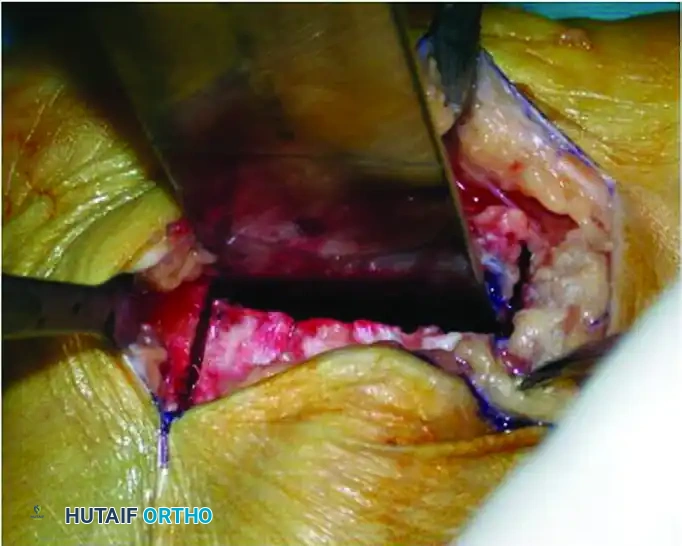
Figure 86-37A: Exposure of the lateral wall of the calcaneus.
- Deepen the incision through the subcutaneous tissues.
- Critical Anatomy: Take meticulous care to identify and protect the lateral dorsal cutaneous branch of the sural nerve, which typically crosses the surgical field in the proximal-to-distal direction.
- Incise the periosteum directly over the lateral wall of the calcaneus and strip it using a periosteal elevator to expose the bone from the posterior tuberosity to the retrocalcaneal space.
3. Designing the Z-Shaped Osteotomy
The osteotomy consists of one horizontal cut and two vertical cuts, creating the "Z" or step-cut configuration.
- The Horizontal Cut: Using an oscillating saw, make a 2 cm long horizontal osteotomy cut parallel to the plantar fascia.
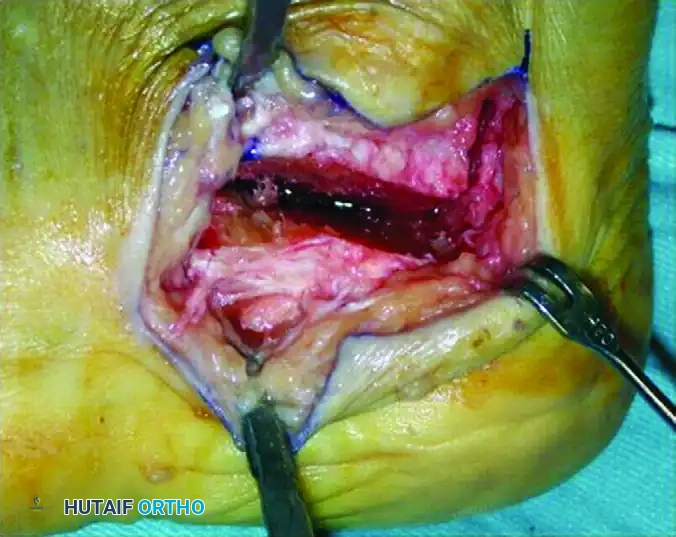
Figure 86-37B: Initiation of the first horizontal cut.

Figure 86-37C: Progression of the horizontal cut and preparation for vertical cuts.
- The Anterior Vertical Cut: Make a vertical cut slightly anterior to the tuberosity, connecting to the anterior aspect of the horizontal cut.
- Surgical Pearl: Use a Hohmann retractor placed plantarly to protect the plantar fascia, intrinsic musculature, and neurovascular bundle.
- The Posterior Vertical Cut: Make another vertical cut in the posterior half of the concavity of the tuberosity, connecting to the posterior aspect of the horizontal cut.
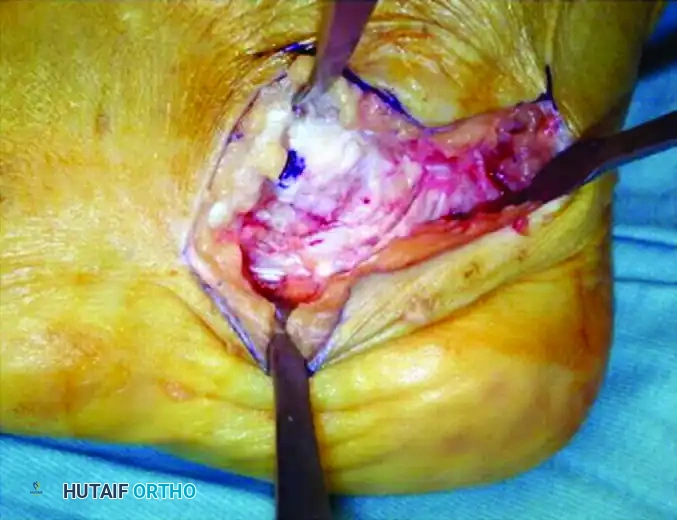
Figure 86-37D: Execution of the two vertical cuts.
Pitfall: Take extreme care not to carry the posterior vertical cut too far posteriorly. Over-penetration will injure the Achilles tendon insertion. The posterior aspect must be strictly protected with a second Hohmann retractor placed superiorly.
4. Wedge Resection and Mobilization
To achieve the desired multiplanar correction, a precise bony wedge is often removed from the step-cut.
- Place four Kirschner wires (K-wires) to mark the exact corners of the bony wedge to be removed. This ensures precise, symmetric resection and prevents inadvertent over-resection.
- Complete the osteotomy cuts using the oscillating saw. Use a broad osteotome or chisel to gently pry and complete the plantar and medial cortices.
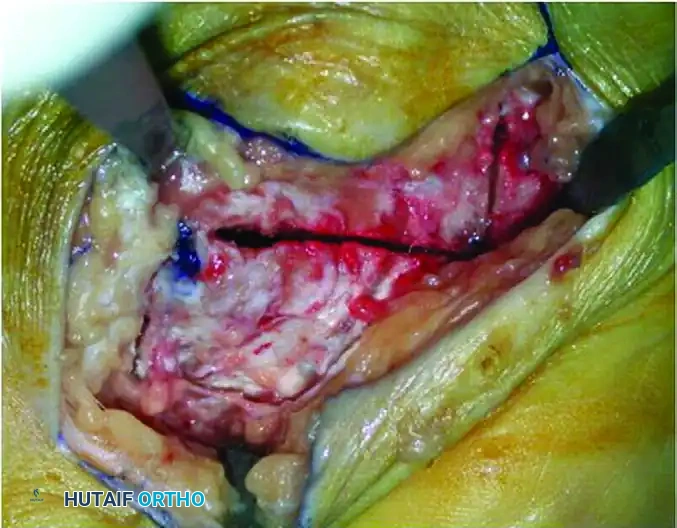
Figure 86-37E: Completion of the osteotomy with a chisel.
- Carefully extract the pre-measured bone wedge.
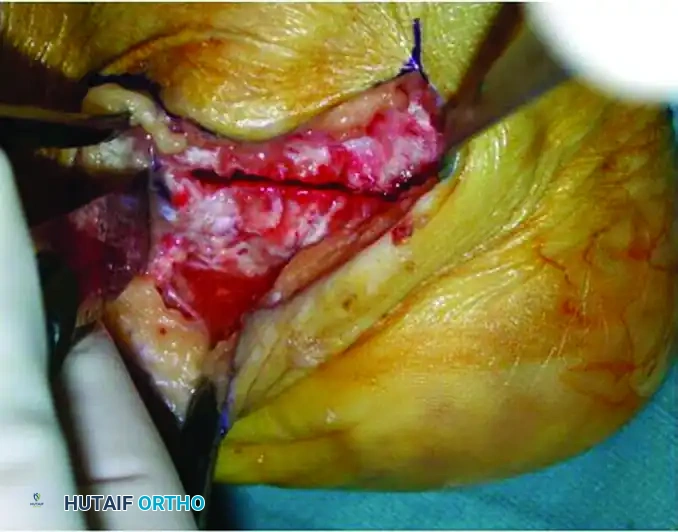
Figure 86-37F: The surgical field after wedge removal and before closing of the osteotomy and lateralization of the tuberosity.
5. Translation and Deformity Correction
With the osteotomy complete and the wedge removed, the posterior tuberosity is now highly mobile.
- Displace the tuberosity laterally to correct the varus alignment.
- Close the bony gap created by the wedge resection to induce the desired valgus angulation.

Figure 86-38A: Lateralization and valgus placement of the tuberosity after a Z-osteotomy and translation of the calcaneus.

Figure 86-38B: Diagrammatic representation of the site of osteotomy and removal of the bone wedge.

Figure 86-38C: Lateral translation of the calcaneal tuberosity viewed from posterior and from proximal.
- Sagittal Plane Adjustment: If the patient has a shortened lateral column or requires increased Achilles tension, the calcaneus can be lengthened by displacing the tuberosity posteriorly along the horizontal cut axis before fixation.
Biomechanical Translation Diagrams
The following diagrams illustrate the precise geometric shifts achieved during the Z-osteotomy:

Diagram A: Medial to Lateral translation mechanics.
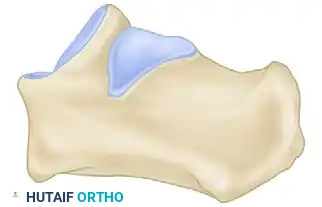
Diagram B: Cross-sectional view of the resected wedge.
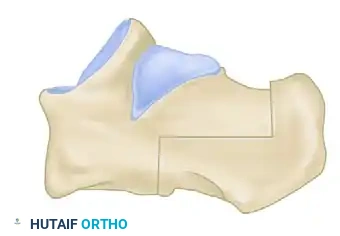
Diagram B (Alternate): Detail of the cancellous bone interface.

Diagram C: Final structural realignment of the calcaneus.
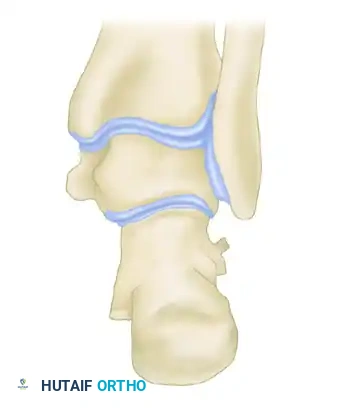
Diagram C (Alternate): Posterior view demonstrating restored mechanical axis.
6. Temporary Fixation and Fluoroscopic Verification
- Remove the Hohmann retractors.
- Manually hold the tuberosity in the corrected, lateralized position.
- Secure the osteotomy provisionally with one or two heavy (e.g., 2.0 mm) Kirschner wires driven from the posterior-inferior tuberosity, directed anteriorly and slightly superiorly into the anterior body of the calcaneus.
- Fluoroscopic Check: Obtain intraoperative axial (Harris) and lateral fluoroscopic views. Confirm that the varus is corrected, the tuberosity is adequately lateralized, and the hardware does not penetrate the subtalar joint.
7. Definitive Fixation
- Once reduction is confirmed, insert one or two large-fragment (e.g., 6.5 mm or 7.0 mm) partially threaded cannulated screws over the K-wires.
- Ensure the screw heads are countersunk into the posterior tuberosity to prevent symptomatic hardware prominence near the Achilles insertion.
- Remove the provisional K-wires.
8. Closure
- Thoroughly irrigate the wound to remove bone debris.
- Deflate the tourniquet and achieve meticulous hemostasis. Hematoma formation in the lateral hindfoot can lead to severe wound breakdown.
- Close the periosteum and subcutaneous tissue in layers using absorbable sutures (e.g., 2-0 or 3-0 Vicryl).
- Close the skin with interrupted non-absorbable sutures (e.g., 3-0 Nylon or Prolene) using a modified Donati or Allgöwer-Donati technique to maximize skin edge perfusion.
Postoperative Care and Rehabilitation Protocol
The success of the Z-shaped calcaneal osteotomy relies heavily on strict adherence to postoperative protocols to ensure bony union and prevent displacement.
Phase 1: Immediate Postoperative (Days 0-4)
- Apply a bulky, sterile compressive dressing.
- Place the limb in a well-padded posterior splint with the ankle in neutral to slight eversion.
- Strict elevation is mandated to decrease swelling and minimize the risk of wound dehiscence.
- Non-weight-bearing (NWB) with crutches or a knee scooter.
Phase 2: Immobilization (Weeks 1-6)
- At 2 to 4 days postoperatively (or at the first clinic visit at 10-14 days for suture removal), transition the patient to a short-leg walking cast or a rigid controlled ankle motion (CAM) boot.
- The patient remains strictly non-weight-bearing for a total of 6 weeks to allow for primary osteotomy consolidation.
- Radiographs (AP, Lateral, Axial) are obtained at 2 weeks and 6 weeks to monitor alignment and early callus formation.
Phase 3: Progressive Weight-Bearing (Weeks 6-12)
- After 6 weeks, if clinical and radiographic evidence of healing is present, the cast is removed.
- The patient is transitioned to a CAM boot and allowed to begin progressive partial weight-bearing, advancing to full weight-bearing as tolerated over the next 4 weeks.
- Initiate physical therapy focusing on:
- Subtalar and ankle joint range of motion.
- Peroneal tendon strengthening to support the newly corrected valgus alignment.
- Achilles tendon stretching.
Phase 4: Return to Activity (Months 3-6)
- Wean out of the CAM boot into supportive athletic footwear.
- The patient can gradually return to full activity, including sports, as tolerated and guided by their physical therapist.
- Maximum medical improvement and final bone remodeling may take up to 12 months.
Complications and Surgical Pitfalls
While highly effective, the Z-shaped calcaneal osteotomy carries specific risks that the orthopaedic surgeon must mitigate:
- Sural Nerve Injury: The lateral dorsal cutaneous branch is highly vulnerable during the initial exposure and retractor placement. Neuroma formation here is notoriously difficult to treat. Meticulous blunt dissection is required.
- Wound Dehiscence: The lateral skin of the heel has tenuous vascularity. Avoid excessive retraction, ensure a thick subcutaneous flap, and utilize tension-free closure techniques.
- Achilles Tendon Laceration: As noted, over-penetration of the posterior vertical cut can sever the Achilles insertion. Always protect the posterior cortex with a retractor.
- Under-correction or Over-correction: Failure to accurately assess the required wedge size or translation distance can result in residual varus or iatrogenic severe valgus. Intraoperative axial fluoroscopy is non-negotiable.
- Nonunion/Delayed Union: Rare due to the large cancellous surface area of the step-cut, but risk is increased in smokers or non-compliant patients who bear weight prematurely.
- Symptomatic Hardware: Prominent screw heads at the posterior heel frequently cause shoe-wear irritation, necessitating hardware removal after bony union is achieved (typically after 6-12 months).
Conclusion
The Z-shaped calcaneal osteotomy represents a sophisticated evolution in the surgical management of the rigid varus hindfoot. By providing a stable, multiplanar correction that lateralizes the mechanical axis and optimizes the Achilles tendon lever arm, surgeons can achieve profound, joint-sparing deformity correction. Mastery of the step-cut geometry, rigorous soft-tissue handling, and precise internal fixation are the hallmarks of success for this advanced orthopaedic procedure.
You Might Also Like
