Comprehensive Surgical Management of the Cavus Foot and Lambrinudi Arthrodesis
Key Takeaway
The surgical management of the cavus foot requires a meticulous understanding of multiplanar deformity, joint flexibility, and underlying neuromuscular etiology. While triple arthrodesis remains a powerful tool for achieving a plantigrade foot, procedures like the Lambrinudi arthrodesis are specifically indicated for fixed equinus and drop foot deformities. This guide details the biomechanical principles, preoperative templating, and step-by-step surgical execution required to optimize patient outcomes and minimize adjacent joint degeneration.
Introduction to Cavus Foot Deformity
The cavus foot presents one of the most complex biomechanical challenges in orthopedic foot and ankle surgery. Characterized by an abnormally high medial longitudinal arch, the deformity is frequently accompanied by hindfoot varus, forefoot pronation, and plantarflexion of the first ray (cavovarus). The etiology is predominantly neuromuscular, with Charcot-Marie-Tooth (CMT) disease being the most common hereditary cause. Other etiologies include poliomyelitis, spinal dysraphism, cerebral palsy, and post-traumatic sequelae.
Successful management requires a profound understanding of foot biomechanics, a meticulous clinical examination, and a tailored surgical approach that addresses both bony architecture and soft-tissue imbalances.
Prognostic Determinants and Treatment Algorithm
The decision-making process for treating a cavus foot is dictated by a systematic evaluation of the deformity. The most important determinants of prognosis and treatment include the following six critical questions:
- Is the deformity multiplanar or single planar?
Cavus deformities rarely exist in isolation. The surgeon must evaluate the presence of hindfoot varus, midfoot adduction, and forefoot equinus. - Is the deformity primarily forefoot, midfoot, hindfoot, or a combination?
Identifying the apex of the deformity dictates the level of intervention (e.g., first metatarsal osteotomy vs. midfoot osteotomy vs. calcaneal osteotomy). - Is one or more of the components fixed?
The Coleman block test is mandatory to differentiate between a flexible, forefoot-driven hindfoot varus and a rigid, fixed hindfoot varus. Fixed deformities necessitate structural bony correction (arthrodesis or osteotomy), whereas flexible deformities may respond to soft-tissue balancing. - Is the underlying cause a progressive, severe course?
Neuromuscular conditions like CMT are progressive. Surgical planning must account for future muscle deterioration, often favoring more rigid stabilization in later stages. - Are tendon transfers required?
Arthrodesis or osteotomy alone is rarely sufficient. Tendon transfers (e.g., Jones procedure, Hibbs procedure, or split anterior tibial tendon transfer) are frequently required to maintain the correction gained and prevent recurrence driven by spastic or overpowering musculature. - Is there a sensory deficit?
The presence of neuropathy drastically alters the surgical algorithm.
Clinical Pearl: In general, the least that can be done to alleviate a specific symptom is the best treatment for cavus foot deformity, especially in feet with sensory deficits. Over-correction or excessive rigid fixation in an insensate foot dramatically increases the risk of Charcot neuroarthropathy and recalcitrant plantar ulcerations.
The Role and Limitations of Triple Arthrodesis
Historically, the triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) was the workhorse procedure for severe cavovarus deformities. However, modern orthopedic principles emphasize joint-sparing techniques whenever possible.
Triple arthrodesis in patients with neuromuscular disease alters the biomechanics of the foot, eliminating essential shock absorption and accommodative motion. Ultimately, this may result in accelerated degenerative arthritis of adjacent joints, particularly the ankle and midtarsal articulations.
Furthermore, outcomes are highly age-dependent. Triple arthrodesis performed in adolescents with Charcot-Marie-Tooth disease is significantly less likely to produce satisfactory long-term results than when performed in adults 40 years of age or older. The adolescent foot lacks the adaptive capacity of the mature skeleton, and progressive neuromuscular imbalance can lead to severe adjacent joint breakdown.
However, if the patient has no sensory deficit and presents with a rigid, severe cavus or cavovarus deformity, triple arthrodesis remains a highly reasonable choice. In end-stage rigid deformities, it may be the only procedure capable of producing a stable, plantigrade foot.
The Lambrinudi Arthrodesis: Biomechanics and Indications
For patients presenting with a paralytic drop foot or severe, fixed equinus deformity (historically common in poliomyelitis), the Lambrinudi arthrodesis offers a specialized variation of the triple arthrodesis.
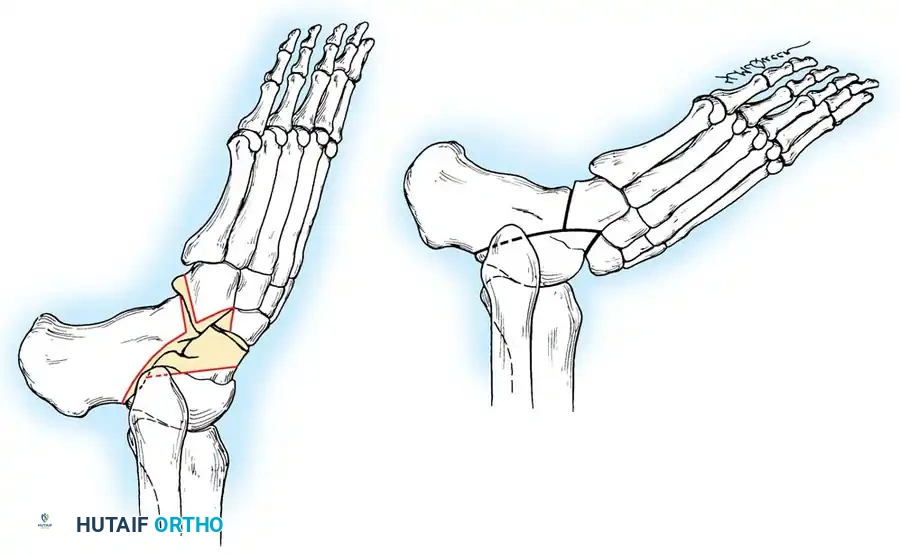
The biomechanical genius of the Lambrinudi procedure lies in its use of the anterior capsule of the ankle joint. By locking the talus in maximal equinus (plantarflexion) within the ankle mortise, the anterior capsule becomes taut, preventing any further plantarflexion. The remainder of the foot is then fused to the talus in a neutral or slightly equinus position. Consequently, when the patient attempts to bear weight or swing the leg, the locked talus prevents the foot from dropping, effectively substituting for absent ankle dorsiflexors.
Preoperative Planning and Templating
Accurate preoperative templating is the most critical step in a successful Lambrinudi arthrodesis. The exact dimensions of the bony wedge to be resected must be calculated to ensure the foot is plantigrade postoperatively.
- Obtain a strict lateral radiograph of the foot and ankle with the ankle held in extreme plantarflexion.
- Trace the radiographic film onto acetate paper (or utilize digital templating software).
- Cut the tracing into three distinct pieces along the outlines of the subtalar and midtarsal joints.
- From these pieces, determine the exact amount of bone to be removed from the plantar and distal aspects of the talus.
- Crucial Alignment: In the tracing, the line representing the tibiotalar articulation is left undisturbed. The line corresponding to the plantar and distal parts of the talus is cut so that when the navicular and calcaneocuboid joints are fitted to it, the foot rests in slight equinus relative to the leg.
Surgical Warning: The final position of the foot should be in 5 to 10 degrees of equinus. If the affected extremity has significant limb length discrepancy (shortening), slightly more equinus may be desirable to assist with limb length equalization.
Surgical Technique: Lambrinudi Arthrodesis (Technique 83-20)
1. Patient Positioning and Exposure
Place the patient in the lateral decubitus or supine position with a large bump under the ipsilateral hip to internally rotate the leg, providing excellent access to the lateral hindfoot. Apply a proximal thigh tourniquet.
Expose the tarsus through a long, lateral curved incision (extended Ollier approach), beginning distal to the lateral malleolus and extending toward the base of the fourth metatarsal.
2. Soft Tissue Dissection and Joint Release
Identify and protect the sural nerve. Expose the peroneal tendon sheath. Section the peroneus longus and brevis tendons using a Z-shaped cut. This allows for adequate exposure and subsequent repair under appropriate tension.
Open the talonavicular and calcaneocuboid joints. To mobilize the hindfoot, sharply divide the interosseous talocalcaneal ligament and the fibular collateral ligaments of the ankle. This extensive release permits complete medial dislocation of the tarsus at the subtalar joint, exposing the articular surfaces.
3. Bony Resection
Utilize a small oscillating power saw for the bone cuts.
Surgical Pearl: A power saw is highly recommended over a chisel or osteotome. Osteotomes can cause microfractures and uncontrolled propagation into the talar body, whereas a saw provides the precise, planar cuts required for the complex geometric fit of the Lambrinudi procedure.
Remove the predetermined wedge of bone from the plantar and distal parts of the neck and body of the talus, as calculated during preoperative templating. Next, remove the cartilage and subchondral bone from the superior surface of the calcaneus to form a flat plane that is perfectly parallel with the longitudinal axis of the foot.
Prepare the midfoot by making a V-shaped trough transversely in the inferior part of the proximal navicular. Denude the calcaneocuboid joint of enough bone to correct any pre-existing lateral or varus deformity.
4. Reduction and Fixation
Firmly wedge the sharp, newly created distal margin of the remaining talus into the prepared V-shaped trough in the navicular. Appose the raw osseous surfaces of the calcaneus and talus.
Critical Positioning Step: Place the distal margin of the talus well medially within the navicular trough. Failure to translate the talus medially will result in an unsatisfactory, lateralized position of the foot.
Surgical Pitfall: No attempt should be made to compensate in the foot for any pre-existing tibial torsion. Attempting to derotate the foot through the arthrodesis will severely compromise the bony contact area and lead to nonunion or severe midfoot malalignment. Tibial torsion must be addressed via a separate supramalleolar osteotomy if clinically necessary.
Once reduced, the talus is mechanically locked in the ankle joint in complete equinus, and the foot cannot be plantarflexed further. Secure the arthrodesis sites using modern rigid internal fixation (e.g., large fragment cannulated screws or compression staples), ensuring absolute stability across the subtalar, talonavicular, and calcaneocuboid joints.
5. Closure
Thoroughly irrigate the wound. Repair the previously sectioned peroneal tendons using a non-absorbable suture, adjusting tension as necessary. Close the extensor retinaculum, subcutaneous tissues, and skin in a routine, layered manner. Apply a sterile dressing and a rigid, well-padded short-leg cast in the corrected position.
Postoperative Protocol
- 0-6 Weeks: The patient is maintained strictly non-weight-bearing in a short-leg cast. Elevation is critical to manage postoperative edema.
- 6-12 Weeks: Radiographs are obtained to assess trabecular bridging. If clinical and radiographic signs of union are progressing, the patient is transitioned to a controlled ankle motion (CAM) boot and allowed progressive partial weight-bearing.
- 12+ Weeks: Full weight-bearing is permitted once solid bony union is confirmed. Custom orthotics or an ankle-foot orthosis (AFO) may be utilized to support the transverse arch and accommodate any residual muscular imbalances.
Concurrent Neuropathic Pathologies: Tarsal Tunnel and Interdigital Neuromas
When managing the cavus foot, the surgeon must be acutely aware of concurrent nerve entrapment syndromes. The altered biomechanics of the cavovarus foot—specifically the rigid hindfoot varus and forefoot overload—predispose patients to secondary neuropathies.
Tarsal Tunnel Syndrome
The tibial nerve and its branches (medial and lateral plantar nerves) are highly susceptible to traction and compression within the fibro-osseous tarsal tunnel. In the cavovarus foot, the varus alignment of the calcaneus increases tension on the flexor retinaculum and the neurovascular bundle.
Patients frequently present with burning pain, paresthesias radiating into the plantar aspect of the foot, and a positive Tinel's sign posterior to the medial malleolus. While conservative management (orthotics to correct hindfoot alignment) is the first line of treatment, surgical decompression of the tarsal tunnel—including release of the deep fascia of the abductor hallucis—is often required if symptoms persist. When performing reconstructive bony surgery for the cavus foot, concurrent tarsal tunnel release should be considered if preoperative electrodiagnostic studies and clinical exams confirm entrapment.
Morton's Neuroma (Interdigital Neuritis)
The cavus foot architecture inherently forces the metatarsals into a more plantarflexed position, drastically increasing forefoot contact pressures during the terminal stance phase of gait. This mechanical overload frequently leads to perineural fibrosis of the common digital nerve, most commonly in the third intermetatarsal space (Morton's Neuroma).
Diagnosis is primarily clinical, characterized by sharp, burning forefoot pain and a palpable Mulder's click upon lateral compression of the metatarsal heads. If conservative measures (metatarsal pads, wide toe-box footwear, corticosteroid injections) fail, surgical excision of the neuroma via a dorsal approach is highly effective. The surgeon must ensure the nerve is resected proximal to the deep transverse metatarsal ligament to prevent the formation of a symptomatic stump neuroma in the weight-bearing area.
Conclusion
The surgical management of the cavus foot demands a comprehensive, multi-staged approach. While the triple arthrodesis and its variations, such as the Lambrinudi procedure, remain powerful tools for correcting rigid deformities and paralytic drop foot, they must be applied judiciously. Careful preoperative templating, meticulous surgical execution, and a deep respect for the underlying neuromuscular etiology and associated nerve entrapments are paramount to achieving a stable, plantigrade, and functional foot.
You Might Also Like

