Resection of Middle Facet Tarsal Coalition: Surgical Guide
Key Takeaway
Middle facet tarsal coalition resection is a joint-preserving procedure aimed at restoring subtalar motion and alleviating pain in patients with rigid flatfoot deformities. This technique involves meticulous excision of the talocalcaneal bridge, interposition of a fat graft to prevent recurrence, and potential adjunctive calcaneal osteotomies to correct associated hindfoot valgus or forefoot abduction. Proper execution demands precise anatomical knowledge of the medial neurovascular structures.
INTRODUCTION AND BIOMECHANICS
Tarsal coalitions represent a complex congenital anomaly characterized by the abnormal union of two or more tarsal bones, leading to altered hindfoot kinematics, progressive deformity, and debilitating pain. Among these, the middle facet talocalcaneal coalition is one of the most common, frequently presenting in the second decade of life as the cartilaginous or fibrous bridge begins to ossify.
The subtalar joint is a critical component of the lower extremity kinematic chain, functioning as a mitered hinge that translates tibial rotation into foot inversion and eversion. A coalition at the middle facet obliterates this motion, forcing compensatory, non-physiologic stresses onto the transverse tarsal (Chopart) and ankle joints. Clinically, this manifests as a rigid pes planovalgus deformity, often accompanied by peroneal spasticity—a reflex muscle spasm secondary to subtalar joint irritation rather than a true neurologic spasticity.
Resection of a middle facet tarsal coalition is a joint-preserving interpositional arthroplasty designed to restore subtalar motion, alleviate pain, and prevent the progression of adjacent joint arthrosis. Success depends on meticulous surgical technique, complete excision of the coalition, and appropriate management of any concurrent structural deformities.
CLINICAL EVALUATION AND IMAGING
Patients typically present with insidious onset of vague, deep hindfoot pain exacerbated by weight-bearing activities or walking on uneven surfaces. Physical examination reveals a rigid flatfoot with absent subtalar inversion and eversion. The heel is often in fixed valgus, and the midfoot may be abducted.
Advanced imaging is mandatory for surgical planning. While standard weight-bearing radiographs may demonstrate secondary signs such as talar beaking or the "C-sign" (a continuous C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali), Computed Tomography (CT) is the gold standard for defining the exact size, location, and osseous nature of the coalition.

FIGURE 82-84 A: Lateral radiograph of an immature foot demonstrating a middle facet tarsal coalition. Note the subtle obscuration of the subtalar joint space.

FIGURE 82-84 B: Lateral radiograph of a patient in their late 20s showing adaptive changes in the middle facet, including dorsal talar beaking secondary to altered midtarsal kinematics.

FIGURE 82-84 C: Harris axial calcaneal view, traditionally used to visualize the middle and posterior facets, demonstrating an abnormal medial joint space.
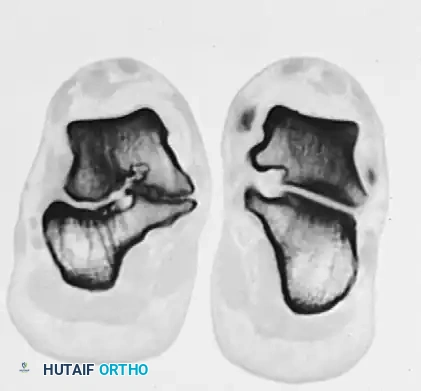
FIGURE 82-84 D: Coronal CT scan confirming degenerative changes in the middle and posterior facets. Note the adaptive changes of the entire shape of the calcaneus and the bridging bone at the sustentaculum tali.

FIGURE 82-84 E: Oblique radiograph of the same foot as in B and D, showing the coalition extending distal to the middle facet.
INDICATIONS AND CONTRAINDICATIONS
Indications for Resection
- Symptomatic middle facet talocalcaneal coalition failing conservative management (e.g., immobilization, orthotics, NSAIDs).
- Coalition size involving less than 50% of the total talocalcaneal joint surface area.
- Absence of advanced degenerative arthrosis in the posterior facet of the subtalar joint or the talonavicular joint.
- Younger patients (typically adolescents) with remaining adaptive potential, though carefully selected adults may also benefit.
Contraindications
- Coalition encompassing >50% of the subtalar joint.
- Advanced degenerative changes in the posterior facet or transverse tarsal joints.
- Severe, rigid, uncorrectable hindfoot valgus that cannot be managed with adjunctive osteotomies (in such cases, a subtalar or triple arthrodesis is preferred).
- Active local or systemic infection.
SURGICAL ANATOMY
The surgical approach to the middle facet requires navigation through the complex anatomy of the medial ankle. The primary landmark is the sustentaculum tali, a medial projection of the calcaneus that supports the middle articular facet.
The structures of the tarsal tunnel, passing posterior to the medial malleolus, must be meticulously protected. From anterior to posterior, these include:
1. Tibialis Posterior Tendon: Lies most anteriorly, directly posterior to the medial malleolus.
2. Flexor Digitorum Longus (FDL) Tendon: Crosses directly over the central portion of the sustentaculum tali and the coalition.
3. Posterior Tibial Artery and Tibial Nerve (Neurovascular Bundle): Courses obliquely across the proximal end of the surgical incision.
4. Flexor Hallucis Longus (FHL) Tendon: Courses inferior (plantar) to the sustentaculum tali. The coalition typically sits directly dorsal to the FHL tendon.
💡 Clinical Pearl
The FDL and FHL tendons serve as critical anatomical boundaries during resection. The FDL marks the superficial/medial aspect of the coalition, while the FHL marks the deep/plantar margin. Protecting these tendons ensures the safety of the adjacent neurovascular bundle.
OPERATIVE TECHNIQUE: STEP-BY-STEP
1. Positioning and Preparation
The patient is placed in the supine position on the operating table. A bump is placed under the contralateral hip to allow external rotation of the operative leg, providing optimal exposure to the medial aspect of the hindfoot. A thigh tourniquet is applied to ensure a bloodless surgical field. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
2. Surgical Incision
- Begin the incision at the proximal margin of the navicular.
- Curve the incision slightly dorsally, passing distal to the tip of the medial malleolus, approximately 1 to 2 cm plantar to its distal tip.
- At that point, curve the incision slightly plantarward, ending 3 to 4 cm proximal to the tip of the medial malleolus.
- Warning: The neurovascular bundle courses obliquely across the proximal end of this incision. Dissection in this area must be blunt and meticulous.
3. Superficial Dissection and Tendon Management
- Incise the skin and subcutaneous tissue. Carefully manage and ligate any large superficial veins to prevent postoperative hematoma.
- Palpate the sustentaculum tali, located approximately 2 cm plantarward and slightly distal from the tip of the medial malleolus.
- Identify the flexor digitorum longus (FDL) tendon, which passes directly over the central portion of the coalition.
- Open the FDL tendon sheath longitudinally. Mobilize the tendon and retract it either dorsally or plantarly to expose the underlying osseous pathology.
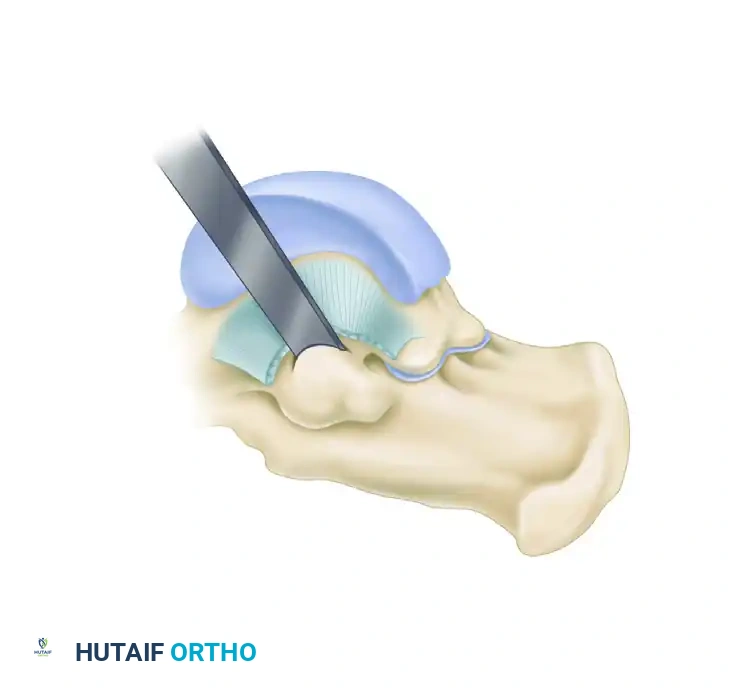
FIGURE 82-85 A: Surgical exposure for resection of a middle facet tarsal coalition. The FDL sheath is opened, and the tendon is retracted to expose the underlying coalition at the sustentaculum tali.
4. Exposure of the Coalition
- Incise the periosteum directly over the coalition. Use a periosteal elevator to define the proximal, distal, dorsal, and plantar margins of the coalition mass.
- Expose the entire coalition and a limited, safe area of the normal posterior facet to serve as a visual landmark. This helps avoid inadvertent injury to the normal articular cartilage with the osteotome.
- Identify the flexor hallucis longus (FHL) tendon at the plantar margin of the coalition. The coalition sits directly over the FHL; retracting the FHL plantarly protects it during the bony resection.
5. Resection of the Coalition
- With all four margins (proximal, distal, dorsal, plantar) clearly exposed, begin the resection.
- Utilize a 1/4-inch to 1/2-inch straight osteotome to outline and determine the margins of the resection. Remove the bulk of the bridging bone.
- Transition to a 3- to 4-mm high-speed burr for the final, precise resection. Continue burring until healthy, glistening hyaline cartilage is visible on both the talar and calcaneal surfaces of the middle facet.
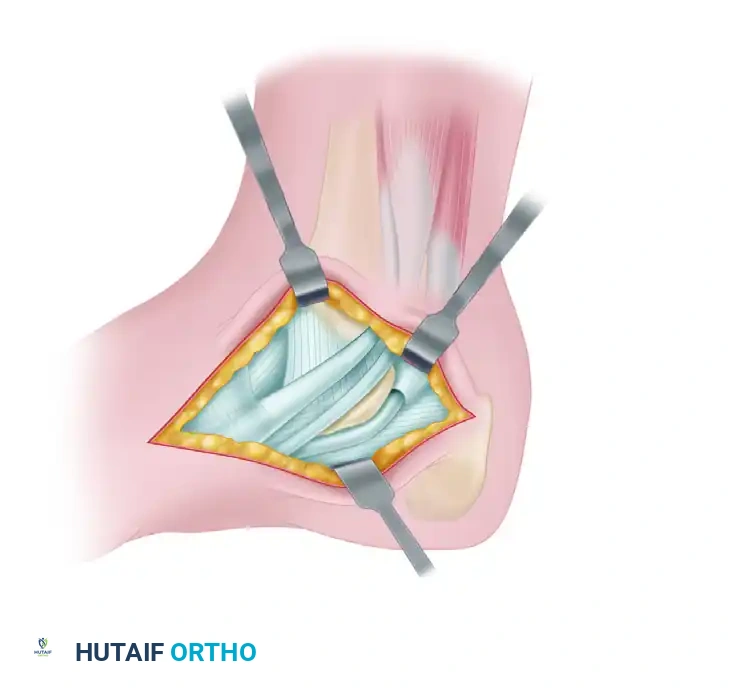
FIGURE 82-85 B: The coalition is systematically removed with an osteotome and burr until the resection is flush with the posterior facet and normal cartilage is visualized.
🚨 Surgical Warning: The Most Common Error
The most frequent cause of failure and recurrence is inadequate resection. The surgeon must extend the resection sufficiently distally and proximally to view normal cartilage on both sides of the joint. Cartilage must be seen throughout the entire depth of the resected area, leaving absolutely no areas of fibrous or bony connection.
- Intraoperative Assessment: Once resection is complete, apply subtalar stress (inversion and eversion). The surgeon should immediately observe and palpate restored motion at the subtalar joint.
6. Interpositional Grafting
To prevent hematoma ossification and recurrence of the coalition, an interpositional material must be placed in the dead space created by the resection.
* Apply bone wax generously to the raw, bleeding cancellous bone surfaces of the resected middle facet.
* Harvest a free fat graft. This can be obtained locally from the Kager's fat pad region if sufficient, or through a separate small incision in the ipsilateral thigh.
* Pack the fat graft into the resection void. Secure it in place using small absorbable sutures passed through the adjacent periosteum of the middle facet or the surrounding soft tissues.
7. Closure
- Release the tourniquet and achieve meticulous hemostasis.
- Allow the FDL tendon to fall back into its anatomical position. Repair the tendon sheath loosely if possible, without causing constriction.
- Close the subcutaneous tissue and skin in a standard layered fashion.
ADJUNCTIVE PROCEDURES
Resection of the coalition restores motion but does not inherently correct the chronic, adaptive pes planovalgus deformity. For patients who have significantly increased heel valgus or severe forefoot abduction in combination with a middle facet coalition, corrective osteotomies of the calcaneus are highly recommended to realign the mechanical axis and protect the subtalar joint.
- Lateral Column Lengthening (Evans Osteotomy): An anterior lengthening osteotomy of the calcaneus is utilized when the primary deformity is forefoot abduction driven by a shortened lateral column.
- Medial Displacement Calcaneal Osteotomy (MDCO): A posterior calcaneal slide osteotomy is indicated when the deformity is primarily severe heel valgus without significant forefoot abduction. This shifts the mechanical pull of the Achilles tendon medially, converting it from an evertor to an invertor of the hindfoot.
Sinus Tarsi Implants (Arthroereisis)
In certain pediatric or adolescent cases, extra-articular subtalar arthroereisis may be utilized as an adjunct to maintain subtalar alignment and prevent excessive valgus while soft tissues adapt post-resection. The Maxwell and Cerniglia biomechanical classification categorizes these implants based on their mechanism of action:

FIGURE 82-86 A: Self-locking wedge implant. Designed to sit within the sinus tarsi and mechanically block excessive eversion.

FIGURE 82-86 B: Axis-altering device. Alters the axis of rotation of the subtalar joint to prevent valgus collapse.

FIGURE 82-86 C: Impact-blocking device. Functions as a direct physical stop between the lateral process of the talus and the floor of the sinus tarsi.
POSTOPERATIVE CARE PROTOCOL
A strict, phased postoperative rehabilitation protocol is essential to ensure wound healing, prevent recurrence, and restore functional mobility.
Phase 1: 0 to 10-12 Days
- Immediately postoperatively, the patient is placed in a well-padded, short-leg, non–weight-bearing (NWB) cast or rigid splint.
- Strict elevation is mandated to minimize edema and protect the incision.
- At 10 to 12 days, the cast is bi-valved, and sutures are removed.
Phase 2: 2 to 4 Weeks
- If the surgical wound has healed satisfactorily, the patient is transitioned to a removable, short-leg controlled ankle motion (CAM) boot.
- Crucial Step: The patient must begin active range of motion (ROM) exercises of the ankle, subtalar, and midtarsal joints immediately. Early mobilization is the primary defense against arthrofibrosis and recurrent coalition formation.
- The patient remains strictly non–weight-bearing during this phase.
Phase 3: 4 to 6 Weeks
- At 4 weeks postoperative, partial weight-bearing (PWB) is initiated in the CAM boot.
- Physical therapy is intensified, focusing on subtalar kinematics, peroneal stretching, and posterior tibial tendon strengthening.
Phase 4: 6 Weeks and Beyond
- Full weight-bearing (FWB) is permitted at 6 weeks.
- The patient is gradually transitioned from the CAM boot to supportive athletic footwear, often utilizing a custom orthotic to support the medial longitudinal arch.
- Return to high-impact sports or heavy labor is typically delayed until 3 to 4 months postoperatively, contingent upon the recovery of strength and pain-free subtalar motion.
COMPLICATIONS AND PITFALLS
- Recurrence of Coalition: The most devastating complication. Usually secondary to inadequate primary resection or failure to interpose a sufficient fat graft. Requires revision resection or, more commonly, progression to subtalar arthrodesis.
- Neurovascular Injury: Iatrogenic injury to the posterior tibial artery or tibial nerve (or its medial/lateral plantar branches) can occur during the initial exposure or if the osteotome plunges too deeply.
- Continued Pain: May result from unrecognized posterior facet arthrosis, failure to correct concurrent flatfoot deformity, or complex regional pain syndrome (CRPS).
- Tendon Injury: Laceration or aggressive retraction of the FDL or FHL can lead to postoperative toe dysfunction or tenosynovitis.
💡 Master Author's Note
The decision to resect a middle facet coalition versus proceeding directly to arthrodesis requires profound clinical judgment. While resection offers the distinct advantage of joint preservation, the surgeon must critically evaluate the patient's age, the percentage of joint involvement, and the rigidity of the surrounding soft tissues. When combined with appropriate biomechanical realignment (e.g., calcaneal osteotomies), resection provides excellent long-term outcomes in the appropriately selected patient.
You Might Also Like

