Surgical Management and Radiographic Evaluation of Cavus Foot Deformity
Key Takeaway
Cavus foot deformity requires meticulous radiographic evaluation, including standing lateral and anteroposterior views, to quantify hindfoot, midfoot, and forefoot contributions. Operative management demands a staged, anatomical approach addressing each component. Key procedures include plantar fascia release for forefoot equinus and comprehensive soft tissue and bony corrections for fixed claw toe contractures. Postoperative protocols emphasize rigid immobilization to maintain the corrected alignment and optimize functional outcomes.
COMPREHENSIVE RADIOGRAPHIC EVALUATION OF CAVus FOOT DEFORMITY
The evaluation of a cavus foot deformity mandates a rigorous, standardized radiographic protocol. Because pes cavus is a complex, multiplanar deformity encompassing the hindfoot, midfoot, and forefoot, weight-bearing imaging is non-negotiable. The primary goal of radiographic assessment is to delineate the apex of the deformity, quantify the relative contributions of the osseous segments, and differentiate between flexible, positional adaptations and rigid, structural contractures. This information is invaluable in preoperative planning, dictating whether soft-tissue releases alone will suffice or if corrective osteotomies and arthrodeses are required.
The Standing Lateral Radiograph
A standing lateral view is the cornerstone of cavus foot imaging. It allows for the precise assessment of the ankle joint position, calcaneal pitch, and the alignment of the midfoot and forefoot.
Key parameters evaluated on the standing lateral view include:
* Calcaneal Pitch: An angle greater than 30 degrees typically indicates a cavus deformity. This helps quantify the hindfoot's contribution to the overall arch elevation.
* Meary’s Angle (Talo-First Metatarsal Angle): In a normal foot, the longitudinal axis of the talus intersects the longitudinal axis of the first metatarsal. In a cavus foot, this angle is disrupted, typically demonstrating a plantarflexed first ray. The degree of plantar flexion of the first ray is a critical metric, as a forefoot-driven cavus often originates here.
* Hibbs Angle: The angle between the longitudinal axis of the calcaneus and the first metatarsal. It approaches 90 degrees in severe cavus deformities.
Forefoot equinus, a frequent driver of the cavus posture, may require isolated soft-tissue procedures—such as the release of the plantar fascia and intrinsic muscles—or may necessitate bony intervention, including a dorsiflexion osteotomy of the first metatarsal or multiple closing wedge osteotomies at the Lisfranc or midtarsal joints.
The standing lateral radiograph also facilitates the estimation of the relative contributions of the hindfoot (talus and calcaneus), midfoot (navicular and cuboid-cuneiform), and forefoot (Lisfranc complex) to the global deformity. Furthermore, the extension deformity of the phalanges on the metatarsal heads during weight bearing helps determine the severity of the fixed deformity.
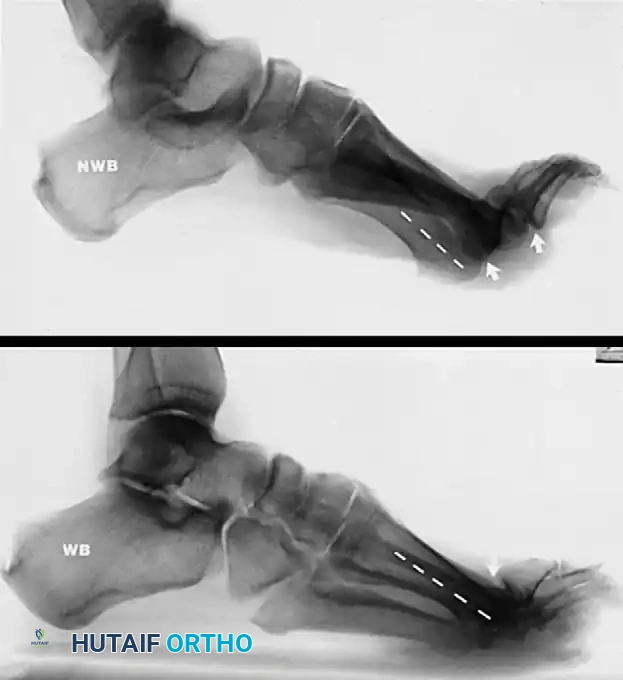
FIGURE 86-20: A, Non–weight bearing view of cavus and claw toe deformities in a patient with Charcot-Marie-Tooth disease. B, On the weight-bearing view, plantar flexion of the first ray is less noticeable, but the clawed hallux remains, indicating a fixed extension contracture at the first metatarsophalangeal joint.
Clinical Pearl: Always compare non-weight-bearing and weight-bearing lateral radiographs. A deformity that partially corrects upon weight bearing suggests a degree of flexibility, whereas a deformity that remains unchanged dictates the need for aggressive bony resection or arthrodesis.
The Standing Anteroposterior (AP) Radiograph
Standing anteroposterior views must be obtained with the hindfoot held in as neutral a position as clinically possible. This view is essential for corroborating any metatarsus adductus component that was suspected during the clinical examination.
Key parameters evaluated on the standing AP view include:
* Kite’s Angle (Talo-Calcaneal Angle): In a cavus foot with a varus hindfoot, the AP talocalcaneal angle is often decreased (less than 20 degrees), indicating parallelism between the talus and calcaneus.
* Talonavicular Coverage: Assesses the degree of midfoot supination and adduction.
* Metatarsus Adductus Angle: Helps differentiate between a true structural adductus of the metatarsals and a positional adductus secondary to midfoot supination.

FIGURE 86-21: Weight-bearing anteroposterior view of a cavus foot in a patient with Charcot-Marie-Tooth disease; note forefoot adduction and supination. The radiographic metatarsus adductus is partially positional and partially true adductus.
Specialized Views and Secondary Radiographic Findings
Beyond the standard AP and lateral views, specialized imaging can provide critical insights into the pathomechanics of the specific patient's deformity. The weight-bearing sesamoid view from a frontal projection is highly beneficial in assessing the rotational profile and the exact degree of first and second metatarsal plantar flexion.
Other radiographic findings that may dictate surgical decision-making include:
1. Degenerative Changes: Even slight osteoarthritic changes in the tibiotalar, subtalar, or midtarsal (Lisfranc) joints must be noted. The presence of arthritis often shifts the surgical plan from joint-sparing osteotomies to corrective arthrodeses.
2. Talar Rotation: Rotation of the talus within the ankle mortise is frequently observed. This is biomechanically driven by talar dorsiflexion coupled with varus alignment at the subtalar joint.
3. Dystrophic Ossification: The presence of dystrophic ossification in the soft tissues, particularly visible on oblique views, strongly suggests chronic tendon or ligament injury. In neuromuscular cavus, this is often seen along the peroneal tendons due to chronic overpull and repetitive microtrauma.

FIGURE 86-22: Dystrophic ossification in a patient with Charcot-Marie-Tooth disease. No peroneus longus function was palpable. The ossification was believed to be caused by repetitive small tears in the peroneal tendons rather than being an accessory ossicle.
PRINCIPLES OF OPERATIVE TREATMENT
The operative treatment of a cavus deformity is rarely a single procedure; rather, it requires the meticulous, staged correction of the separate components within the foot and ankle. The surgical philosophy dictates that all deforming forces must be neutralized, flexible deformities corrected with soft-tissue balancing, and rigid deformities corrected with osseous realignment. The recommended techniques are described below for each specific anatomical component.
SURGICAL MANAGEMENT OF CLAW TOES
Claw toe deformities are a hallmark of the cavus foot, particularly in neuromuscular etiologies such as Charcot-Marie-Tooth (CMT) disease. The deformity is characterized by hyperextension at the metatarsophalangeal (MTP) joint and flexion at the proximal and distal interphalangeal (PIP and DIP) joints. This is biomechanically driven by an "intrinsic-minus" state, where the strong extrinsic extensors (Extensor Digitorum Longus) overpower the weakened intrinsic muscles (lumbricals and interossei).
In patients with traumatic pes cavus or mild, flexible deformities, only the claw toe deformities and possibly a tight plantar fascia may require surgical treatment. In these select cases, the bony midfoot deformity can be managed non-operatively with appropriate shoe modifications and custom orthotics.
However, for fixed contractures at the metatarsophalangeal and interphalangeal joints, a comprehensive, multi-level surgical approach is mandatory. The following sequential steps are recommended to achieve a plantigrade, functional forefoot:
Step-by-Step Surgical Correction of Fixed Claw Toes
- Lengthening of the Extrinsic Extensors: Perform a Z-lengthening or fractional lengthening of the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons. This removes the primary deforming hyperextension force at the MTP joints.
- Tenotomy of the Short Extensors: Perform a tenotomy of the extensor digitorum brevis (EDB) and the extensor hallucis brevis (EHB).
- Dorsal Capsulotomy: Perform a thorough dorsal capsulotomy of the metatarsophalangeal joints. A McGlamry elevator can be utilized to release the dorsal capsule and collateral ligaments, allowing the proximal phalanx to reduce over the metatarsal head.
- Osseous Resection: For rigid deformities, soft tissue release alone is insufficient. Resection of the head and neck of the proximal phalanges (resection arthroplasty) or a formal proximal interphalangeal (PIP) joint arthrodesis is required to correct the fixed flexion contracture at the PIP joint.
- Plantar Fascia Release: Release of the plantar fascia is often indicated to address the underlying forefoot equinus and reduce the tension on the windlass mechanism (detailed in the subsequent section).
- Hallux Interphalangeal Joint Management: The hallux requires special attention due to its critical role in the windlass mechanism and terminal stance. Recommended procedures include:
- Arthrodesis of the interphalangeal (IP) joint of the hallux.
- Alternatively, a plantar plate release combined with sectioning of the collateral ligaments at the IP joint of the hallux, stabilized with temporary Kirschner wire (K-wire) fixation.
Surgical Warning: When performing multiple dorsal capsulotomies and PIP joint resections, meticulous care must be taken to protect the dorsal neurovascular bundles. Excessive traction or aggressive dissection can lead to digital ischemia or permanent sensory deficits.
PLANTAR FASCIA RELEASE (STEINDLER STRIPPING AND MODIFICATIONS)
The plantar fascia is a primary static stabilizer of the longitudinal arch. In the cavus foot, contracture of the plantar fascia acts as a bowstring, tethering the forefoot to the hindfoot and exacerbating the forefoot equinus and calcaneal pitch. Release of the plantar fascia is a foundational step in the surgical reconstruction of the cavus foot.
Indications and Preoperative Planning
Plantar fascia release is indicated for rigid forefoot equinus that does not correct with conservative measures. It is rarely performed as an isolated procedure; it is almost universally combined with intrinsic muscle releases, tendon transfers, or midfoot osteotomies.

FIGURE 86-23: Technique of plantar fascia release. The medial approach allows excellent visualization of the fascial bands while protecting the critical neurovascular structures of the plantar hindfoot.
🔪 Surgical Technique 86-5: Plantar Fascia Release
1. Incision and Exposure:
Make a longitudinal incision along the medial side of the calcaneus. Carry the incision distally to a point approximately 4 cm anterior to the medial tubercle of the calcaneus (see Fig. 86-23). This medial approach avoids the weight-bearing surface of the heel pad and minimizes the risk of painful scar formation.
2. Deep Dissection:
Carefully deepen the incision through the subcutaneous fat. Identify the medial border of the plantar fascia. Using blunt and sharp dissection, separate the superficial and deep surfaces of the plantar fascia from the underlying intrinsic muscle belly (flexor digitorum brevis) and the overlying plantar fat pad. It is critical to free the fascia completely throughout its entire breadth, from medial to lateral.
3. Fascial Transection:
Incise the fascia transversely close to its origin, where it blends into the plantar surface of the calcaneal tuberosity.
Surgical Pearl: Place a periosteal elevator, a right-angle retractor, or a Chandler retractor on the deep surface of the fascia as it is released. This maneuver protects the underlying lateral plantar nerve and vessels, as well as the first branch of the lateral plantar nerve (nerve to the abductor digiti minimi), which courses directly deep to the fascia in this region.

Anterior border of the stripped area, demonstrating the extent of the fascial release required to achieve adequate correction of the forefoot equinus.
4. Assessment and Secondary Release:
Following the primary release at the calcaneus, manually dorsiflex the forefoot to assess the correction. If the plantar fascia still feels tight and tethers the first ray, a secondary release is required.
* Incise the medial band of the plantar fascia again through a separate, small incision located 2 cm proximal to the first metatarsal head.
* Critical Anatomy: Protect the flexor hallucis longus (FHL) tendon during this distal release. Release the medial band of the plantar fascia down to, but not through, the flexor hallucis brevis muscle.
* Simultaneously dorsiflex the first metatarsal by applying firm upward pressure on the plantar aspect of the first metatarsal head to ensure complete release of the contracture.
5. Hemostasis and Closure:
Deflate the tourniquet (if used) and secure meticulous hemostasis. Hematoma formation in the plantar dead space can lead to severe fibrosis and recurrent contracture. Close the wound in layers, utilizing nonabsorbable sutures for the skin in adult patients to withstand the tension of the plantar skin.
Postoperative Care and Rehabilitation Protocol
Release of the plantar fascia is seldom performed as an isolated procedure; the postoperative protocol is usually dictated by the concomitant osseous or tendon procedures (e.g., triple arthrodesis, Jones transfer).
However, if performed as an isolated procedure or in conjunction with minor soft-tissue balancing:
* Initial Immobilization: A short-leg cast is applied immediately postoperatively. The cast must be molded gently into the arch to maintain the correction and flatten the longitudinal arch.
* Weight-Bearing Status: The patient is kept strictly non–weight bearing for the first 3 weeks to allow for soft tissue healing and to prevent wound dehiscence.
* Transition: At the 3-week mark, the sutures are removed. A well-molded, weight-bearing short-leg cast (or a rigid controlled ankle motion [CAM] boot, depending on surgeon preference and patient compliance) is applied.
* Continued Support: The weight-bearing cast is worn for an additional 3 weeks (total of 6 weeks of immobilization). Following cast removal, the patient is transitioned into a supportive shoe with a custom orthotic to support the newly aligned midfoot and prevent recurrence of the cavus posture. Aggressive physical therapy focusing on intrinsic foot strengthening and Achilles tendon stretching is initiated.
📚 Medical References
- Cavus foot deformity in children, J Am Acad Orthop Surg 11:201, 2003.
- Shapiro F, Bresnan MJ: Current concepts review: orthopaedic management of childhood neuromuscular disease II: diseases of muscle, J Bone Joint Surg 64A:1102, 1982.
- Shapiro F, Specht L: Current concepts review: the diagnosis and orthopaedic treatment of childhood spinal muscular atrophy, peripheral neuropathy, Friedreich ataxia, and arthrogryposis, J Bone Joint Surg 75A:1699, 1993.
- Shapiro F, Specht L: Current concepts review: the diagnosis and orthopaedic treatment of inherited muscular diseases of childhood, J Bone Joint Surg 75A:439, 1993.
- Shaw NJ, White CP, Fraser WD, et al: Osteopenia in cerebral palsy, Arch Dis Child 71:235, 1994.
- Siegel IM: The clinical management of muscle disease: a practical manual of diagnosis and treatment, London, 1977, William Heinemann. Siegel IM: Diagnosis, management, and orthopaedic treatment of muscular dystrophy, Instr Course Lect 30:3, 1981.
- Tachdjian MO: Pediatric orthopedics, 2nd ed, Philadelphia, 1990, Saunders. Vedantam R, Capelli AM, Schoenecker PL:
You Might Also Like