Comprehensive Surgical Management and Clinical Evaluation of the Cavus Foot Deformity
Key Takeaway
The cavus foot presents a complex multiplanar deformity characterized by abnormal elevation of the medial longitudinal arch. Effective orthopedic management requires a rigorous understanding of its underlying neuromuscular etiology, such as Charcot-Marie-Tooth disease, and precise biomechanical evaluation. This guide details the clinical findings, radiographic parameters, and step-by-step surgical interventions—ranging from soft-tissue balancing to corrective osteotomies—necessary to restore a plantigrade, stable, and pain-free foot.
INTRODUCTION TO CAVus FOOT DEFORMITY
The cavus foot is a complex, multiplanar deformity characterized by an abnormally high medial longitudinal arch, frequently accompanied by hindfoot varus, forefoot pronation, and clawing of the toes. Patients seek orthopedic intervention for a variety of reasons, ranging from intractable metatarsalgia and recurrent ankle instability to progressive gait deterioration and pre-ulcerative plantar callosities.
It is a fundamental orthopedic maxim that a cavus foot is a symptom of an underlying neurological disorder until proven otherwise. While idiopathic cases exist, a meticulous clinical, neurological, and radiographic evaluation is mandatory to rule out progressive neuromuscular pathologies before formulating a surgical plan.
ETIOLOGY AND NEUROMUSCULAR PATHOGENESIS
Idiopathic Cavus Deformity
In patients presenting with an adducted, pronated forefoot (relative to the hindfoot), a plantar flexed first ray, midfoot equinus, and heel varus, the diagnosis of idiopathic pes cavus must strictly be one of exclusion. A subset of patients possesses no discernible neuromuscular disease, spinal dysraphism, or history of trauma. These patients, who maintain normal sensory and proprioceptive feedback, generally respond well to both conservative and surgical treatments, provided the procedures are carefully tailored to correct the specific components of the deformity.
Charcot-Marie-Tooth Disease (Hereditary Motor Sensory Neuropathy)
A patient presenting with progressive muscular and sensory deficits presents a profoundly different clinical challenge. Charcot-Marie-Tooth (CMT) disease, or peroneal muscular atrophy, is the most common cause of the neuromuscular cavus foot. It is more prevalent in males (2:1) but often manifests more severely in females.
Clinical Pearl: A detailed family history is paramount. CMT exhibits striking variability in penetration and clinical expression—even within immediate family members. Furthermore, penetrance is often asymmetric, necessitating individualized treatment recommendations for each extremity.
- Type I CMT (Demyelinating): The most common variant, typically presenting in the second or third decade of life with a less severe clinical course.
- Type II CMT (Axonal): Usually manifests between 5 and 15 years of age, presenting as a severe motor-sensory deficit.
The deformity in CMT is driven by specific muscle imbalances. The peroneus brevis weakens before the peroneus longus, leading to unopposed plantar flexion of the first ray. Simultaneously, the tibialis anterior weakens before the tibialis posterior, contributing to forefoot equinus. Intrinsic muscle wasting leads to the classic claw toe deformity.

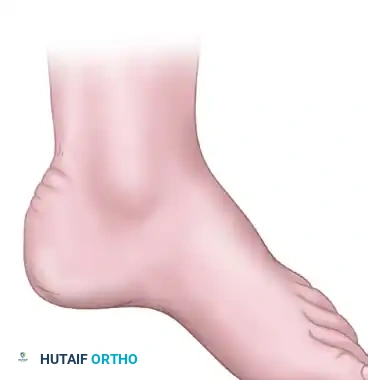
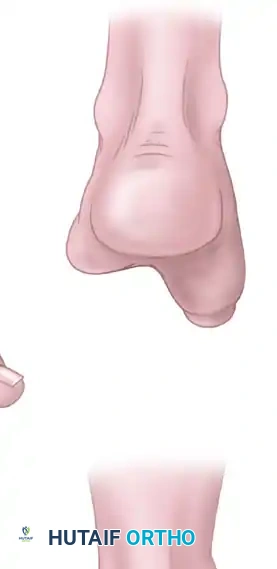
Lateral and frontal view of a plantar flexed first ray as seen in Charcot-Marie-Tooth disease compared with a normal foot.
Postpoliomyelitis Cavus Deformity
Patients with cavus deformity secondary to residual poliomyelitis exhibit distinct physical findings compared to those with CMT. The post-polio foot typically features a combination of anterior and posterior deformities driven by static muscle imbalance rather than progressive neuropathy.
A weak gastrocnemius-soleus complex opposing a strong anterior tibial muscle may cause a calcaneocavus deformity. Conversely, a strong gastrocnemius-soleus and posterior tibial muscle combined with weak toe extensors and anterior tibial muscles results in severe equinocavus. Because sensation remains intact and the deformity is non-progressive, post-polio patients generally have a more predictable surgical prognosis than those with CMT.
BIOMECHANICS OF THE CAVUS FOOT
Understanding the biomechanics of the cavus foot is essential for surgical decision-making. The deformity is primarily driven by the "tripod effect." The rigid, plantar flexed first ray acts as the anterior medial leg of the tripod.


During the stance phase of gait, as the rigidly plantar flexed first metatarsal strikes the ground, it prematurely loads the medial column. To accommodate this, the hindfoot is mechanically forced into a compensatory varus position.

When the plantar flexed first ray strikes the ground, the heel is forced into varus.
Over time, this chronic compensatory hindfoot varus leads to attenuation of the lateral ligamentous complex, recurrent ankle sprains, and eventually, rigid degenerative changes in the subtalar joint.
CLINICAL EVALUATION AND DIAGNOSTIC FINDINGS
A detailed motor-sensory examination must precede any treatment plan. Assess for spasticity, intrinsic muscle wasting, and sensory deficits.
Surgical Warning: Surgery in the presence of profound decreased plantar sensation is fraught with complications, including Charcot neuroarthropathy and chronic ulceration. Patients with pre-ulcerative lesions and severe sensory deficits should initially be managed nonoperatively with custom ankle-foot orthoses (AFOs).
Assessing Hindfoot Flexibility: The Coleman Block Test
The cornerstone of the cavus foot physical examination is the Coleman block test (lateral block test). This test determines whether the hindfoot varus is flexible (driven by the forefoot) or fixed (rigid structural change).
- The patient stands with the heel and lateral border of the foot on a 1-inch wooden block.
- The plantar flexed first metatarsal is allowed to hang free off the medial edge of the block.
- If the hindfoot varus corrects to a neutral or valgus position, the deformity is flexible and driven entirely by the forefoot. Surgical correction can focus on the forefoot (e.g., 1st metatarsal osteotomy).
- If the hindfoot remains in varus, the deformity is fixed. Surgical correction must address both the forefoot and the hindfoot (e.g., calcaneal osteotomy).
Lateral block test. The plantar flexed first metatarsal is allowed to hang free from the block; a supple hindfoot will subsequently correct to neutral.
RADIOGRAPHIC EVALUATION
Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot, along with an AP and mortise of the ankle, are required.
Key radiographic parameters include:
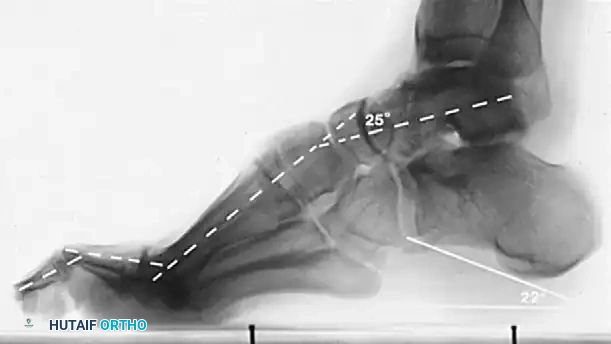
* Meary’s Angle (Talus-First Metatarsal Angle): Normally 0 degrees. In a cavus foot, the angle is increased, with the apex directed dorsally.
* Hibbs Angle: Intersection of the longitudinal axis of the calcaneus and the first metatarsal. Normal is < 45 degrees; it approaches 90 degrees in severe cavus.
* Calcaneal Pitch: Measures the degree of calcaneal deformity. Normal is 20-30 degrees.


Normal calcaneal pitch, but forefoot equinus in a patient with Charcot-Marie-Tooth disease. The calcaneal pitch angle measures the degree of calcaneus deformity.
In CMT, patients typically exhibit forefoot equinus with a relatively normal calcaneal pitch. In contrast, post-polio patients often present with a severe calcaneocavus deformity characterized by a drastically increased calcaneal pitch.
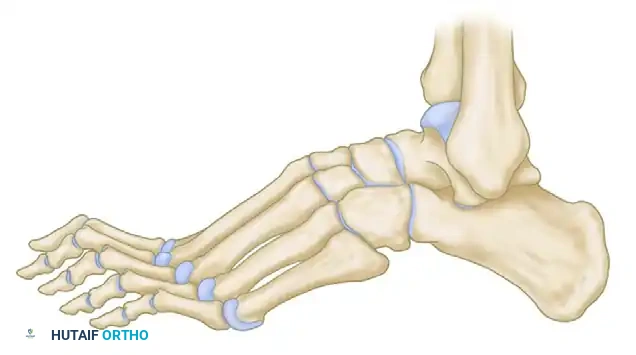
Calcaneal pitch variations in idiopathic and postpoliomyelitis deformities.
NONOPERATIVE MANAGEMENT
Patients with mild, flexible, idiopathic non-progressive cavus deformities almost invariably do well with conservative treatment. The primary goals are to accommodate the deformity, distribute plantar pressures, and prevent ulceration.
* Orthotics: Custom insoles with metatarsal pads or metatarsal bars relieve pressure under the metatarsal heads.
* Shoe Wear: Extra-depth shoes with a wide toe box accommodate claw toes.
* Callus Care: Routine debridement of painful plantar callosities.
SURGICAL MANAGEMENT: PRINCIPLES AND STEP-BY-STEP APPROACHES
When conservative measures fail, or in the presence of a progressive neuromuscular deformity with fixed pronation of the forefoot and painful callosities, surgical intervention is indicated. The overarching goal is to create a plantigrade, stable, and braceable foot while preserving as much joint mobility as possible. Joint-sparing procedures should be prioritized, though selected arthrodesis remains a viable option for rigid, end-stage deformities.
Preoperative Positioning and Anesthesia
- Positioning: The patient is placed supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral position for lateral approaches.
- Tourniquet: A thigh or calf tourniquet is applied.
- Anesthesia: General anesthesia or regional anesthesia (popliteal block) is utilized based on patient comorbidities and anesthesiologist preference.
Step 1: Soft Tissue Releases (Plantar Fascia and Tendons)
Soft tissue contractures must be addressed before osseous correction.
Radical Plantar Fascia Release (Steindler Stripping):
1. Make a medial incision over the calcaneal tuberosity.
2. Identify and protect the medial calcaneal nerve branches.
3. Release the plantar fascia and the origins of the short plantar muscles (abductor hallucis, flexor digitorum brevis, abductor digiti minimi) directly off the calcaneus.

Surgical diagrams illustrating the release of the plantar fascial bands and intrinsic musculature to mobilize the medial column.
Step 2: Tendon Transfers
Tendon transfers are utilized to rebalance the foot and remove the deforming forces.
Peroneus Longus to Peroneus Brevis Transfer:
In CMT, the overactive peroneus longus drives the first ray into plantar flexion, while the weak peroneus brevis fails to evert the foot.
1. Identify both tendons through a lateral incision over the fibula.
2. Transect the peroneus longus distally and tenodese it to the peroneus brevis. This removes the plantar-flexing force on the first ray and augments hindfoot eversion.
Jones Transfer (for Claw Toes):
1. Transfer the Extensor Hallucis Longus (EHL) to the neck of the first metatarsal to elevate the first ray.
2. Perform an interphalangeal joint arthrodesis of the hallux to prevent a drop toe.
Step 3: Osseous Procedures (Osteotomies)
If the deformity remains after soft tissue release, osseous correction is required.
First Metatarsal Dorsiflexion Osteotomy:
Indicated for a rigid plantar flexed first ray.
1. Make a dorsal incision over the first metatarsal base.
2. Perform a dorsally based closing wedge osteotomy approximately 1 cm distal to the tarsometatarsal joint.
3. Close the osteotomy, elevating the metatarsal head, and fixate with a dorsal plate or compression screws.

Diagrammatic representation of the first metatarsal dorsiflexion osteotomy to correct the rigid anterior pillar.
Calcaneal Osteotomy:
Indicated if the Coleman block test demonstrates a fixed hindfoot varus.
Dwyer Closing Wedge Osteotomy:
1. Make an oblique lateral incision posterior to the sural nerve and peroneal tendons.
2. Expose the lateral wall of the calcaneus.
3. Remove a laterally based wedge of bone.
4. Close the osteotomy to valgus and fixate with headless compression screws or a lateral plate.


Surgical diagrams demonstrating the lateral closing wedge (Dwyer) calcaneal osteotomy and lateralizing sliding osteotomy to correct fixed hindfoot varus.
Step 4: Arthrodesis
In severe, rigid deformities with degenerative joint disease, joint-sparing osteotomies are insufficient. A Triple Arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is indicated.
1. Extensive cartilage debridement is performed.
2. The foot is manually corrected to a plantigrade position.
3. Rigid internal fixation is achieved using large fragment screws or specialized midfoot/hindfoot plating systems.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Strict adherence to postoperative protocols is vital for successful outcomes, particularly when managing osteotomies and tendon transfers in neuropathic patients.
- Weeks 0-2: The patient is placed in a well-padded, short-leg non-weight-bearing (NWB) splint. Elevation is critical to manage edema.
- Weeks 2-6: Sutures are removed. The patient is transitioned to a NWB short-leg cast.
- Weeks 6-10: Radiographs are obtained to confirm osseous union. If healing is adequate, the patient is transitioned to a Controlled Ankle Motion (CAM) boot and begins progressive weight-bearing.
- Weeks 10+: Transition to regular shoe wear, often requiring custom orthotics or an AFO depending on the underlying neurological deficit. Physical therapy focuses on proprioception, gait training, and strengthening of transferred tendons.
COMPLICATIONS AND PITFALLS
- Under-correction: The most common pitfall. Failure to recognize a fixed hindfoot varus (ignoring the Coleman block test) leads to isolated forefoot surgery and persistent lateral column overload.
- Over-correction: Excessive dorsiflexion of the first metatarsal can lead to transfer metatarsalgia to the lesser metatarsal heads.
- Nonunion/Delayed Union: Particularly a risk in the first metatarsal base osteotomy and triple arthrodesis. Meticulous joint preparation and rigid fixation are required.
- Neurovascular Injury: The sural nerve is at high risk during lateral calcaneal osteotomies. Careful soft tissue handling and retractor placement are mandatory.
You Might Also Like
