Operative Orthopaedics: Comprehensive Management of the Cavus Foot
Key Takeaway
The cavus foot is a complex triplanar deformity characterized by an abnormally high medial longitudinal arch, forefoot pronation, and hindfoot varus. Driven primarily by neuromuscular imbalances, such as Charcot-Marie-Tooth disease, the deformity progresses from flexible to rigid. Successful management requires a meticulous understanding of intrinsic-extrinsic muscle biomechanics, precise clinical evaluation using the Coleman block test, and tailored surgical interventions ranging from soft-tissue releases to corrective osteotomies and arthrodesis.
Introduction to the Cavus Foot
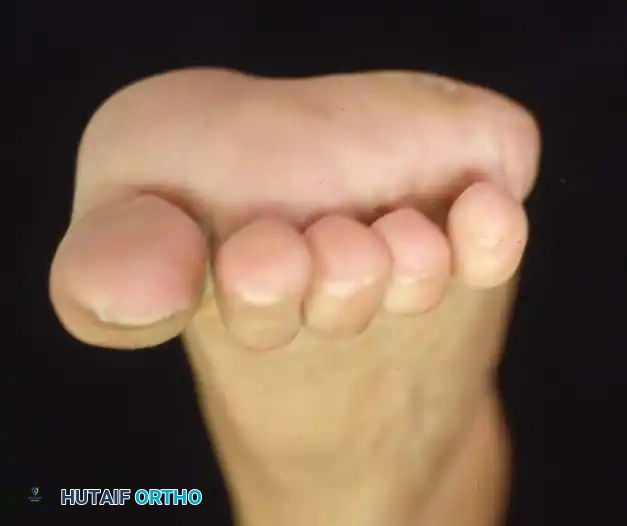
In its simplest anatomical definition, a cavus foot is characterized by an abnormally high medial longitudinal arch. However, in clinical orthopedic practice, it is recognized as a complex, triplanar deformity that encompasses a spectrum of structural abnormalities. This high arch rarely exists in isolation; it is almost universally accompanied by hyperextension of the toes at the metatarsophalangeal (MTP) joints and hyperflexion at the interphalangeal (IP) joints (claw toes).
Furthermore, the deformity presents with pronation and adduction of the forefoot (forefoot valgus), a prominent "bony" dorsum of the midfoot with wrinkled skin folds on the medial plantar aspect, a lengthened lateral border of the foot, and a shortened medial border. Patients frequently develop painful calluses beneath the metatarsal heads due to altered weight-bearing mechanics. The subtalar joint exhibits varied degrees of stiffness, often accompanied by a fixed or flexible varus deformity of the heel, and tightness of the Achilles tendon with or without a frank equinus contracture.

Although pes cavus with multiple deformities is difficult to define mathematically, it is easily recognized upon clinical inspection. However, it remains one of the most challenging conditions to treat, both operatively and nonoperatively, requiring a profound understanding of foot and ankle biomechanics.

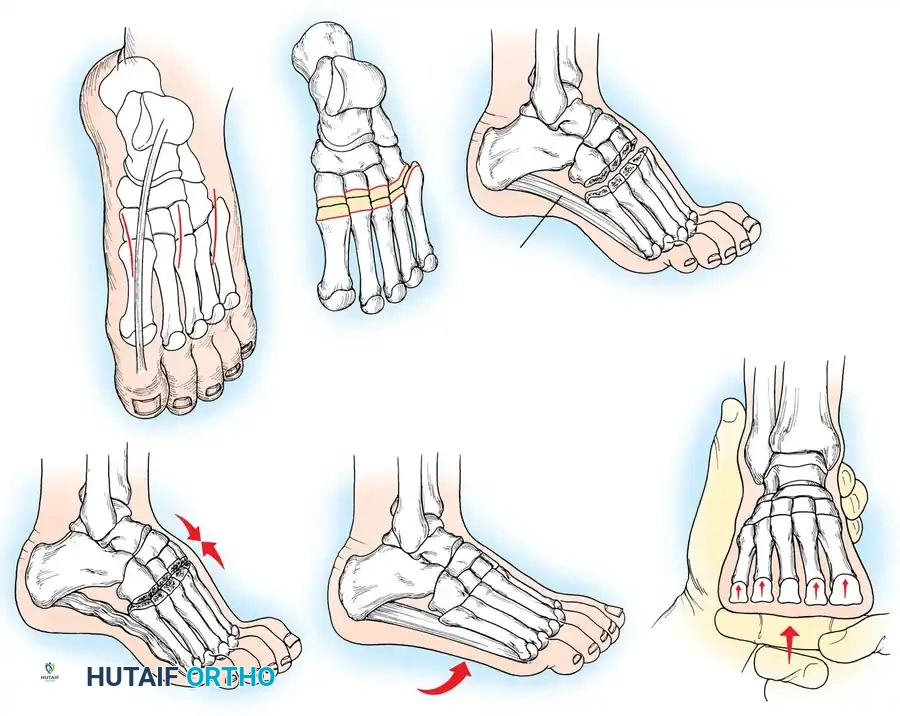
Fig. 1: A, Mild cavus deformity and clawing of toes. B, Calluses beneath metatarsal heads are the most common symptom prompting orthopaedic consultation. C, Marked forefoot equinus and resulting dorsal prominence of the tarsus. D, Forefoot is pronated in relation to the hindfoot during weight bearing. E, Shortening of the medial column of the foot.
Etiology and Pathogenesis
What causes such a relentless combination of deformities? How does a mildly elevated medial longitudinal arch progress to a rigid equinovarus deformity with fixed claw toes? The progression of the deformity is inextricably linked to its underlying etiology.
Historically, up to 80% of cavus foot deformities were classified as "idiopathic." Today, with the advent of detailed neurological examinations, electromyography (EMG), nerve conduction velocities (NCV), magnetic resonance imaging (MRI) of the neuroaxis, and advanced genetic testing, a definitive cause can be identified in more than 80% of patients.
Neuromuscular Disease
In skeletally mature patients, the etiology is most frequently neuromuscular. The most common neuromuscular diseases causing pes cavus are Charcot-Marie-Tooth (CMT) disease (hereditary motor and sensory neuropathy) and residual poliomyelitis.
Other conditions that may present with a cavus deformity include:
* Spinal dysraphism (tethered cord, diastematomyelia)
* Cerebral palsy
* Primary cerebellar disease (Friedreich's ataxia)
* Arthrogryposis multiplex congenita
* Severe, untreated, or relapsed clubfeet
Clinical Pearl: A unilateral cavus foot in a previously normal child or young adult should raise immediate suspicion for a spinal cord lesion (e.g., tethered cord, syrinx, or intraspinal tumor) until proven otherwise. MRI of the entire spine is mandatory.
Traumatic Cavus Deformity
Traumatic cavus deformity is typically the sequela of a deep posterior compartment syndrome following a fracture of the tibia or fibula, or malunion of midfoot/hindfoot fractures (such as a talar neck fracture). The deformity may not manifest for several months following the initial ischemic insult. Fibrosis and contracture of the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) lead to a relentless progression toward a rigid cavovarus and claw toe deformity.
Idiopathic Pes Cavus
In a small subset of patients, no definitive neuromuscular, genetic, or traumatic cause is discovered despite exhaustive diagnostic efforts. These patients possess normal sensory and proprioceptive feedback and generally respond well to carefully selected surgical procedures aimed at correcting specific anatomical components of the deformity.

Fig. 2: Fifteen-year-old boy with “idiopathic” pes cavus after extensive neurological evaluation.
Biomechanics and Pathoanatomy
The underlying pathological mechanism of the cavus deformity is an imbalance between the extrinsic and intrinsic musculature of the foot.
The Intrinsic-Extrinsic Imbalance
The intrinsic muscles of the plantar foot function to flex the MTP joints and extend the IP joints. Weakness of these muscles—whether absolute or relative to their extrinsic antagonists—disrupts the delicate balance of the foot. This leads to extensor substitution or overpull, resulting in the classic claw toe deformity.
Charcot-Marie-Tooth (CMT) Disease Biomechanics
In progressive neuromuscular diseases like CMT, the deformity follows a predictable pattern of muscle denervation. The intrinsic muscles are affected first, followed by the anterior compartment (tibialis anterior) and lateral compartment (peroneus brevis).
Crucially, the peroneus longus and tibialis posterior are relatively spared.
1. Forefoot Valgus: The unopposed pull of the strong peroneus longus against a weak tibialis anterior forcefully plantarflexes the first ray, causing fixed pronation of the forefoot (forefoot valgus).
2. Hindfoot Varus: With weakness of the peroneus brevis, the strong tibialis posterior exacerbates forefoot equinus and forcefully inverts the midtarsal joints.
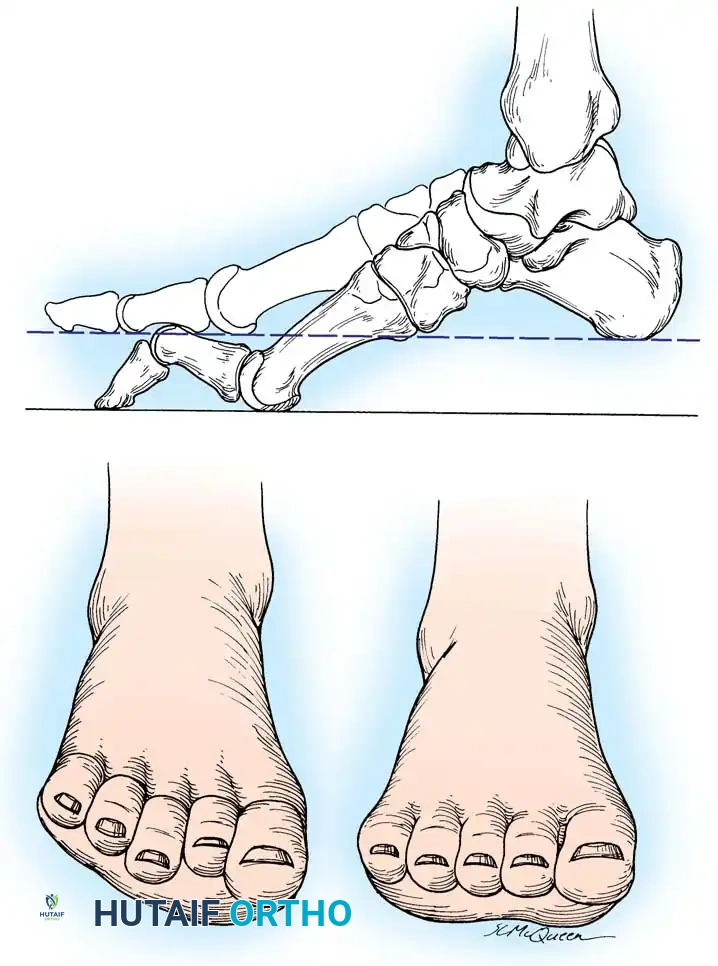
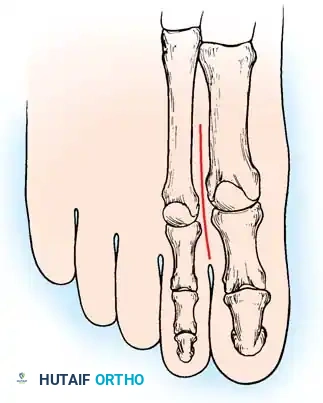
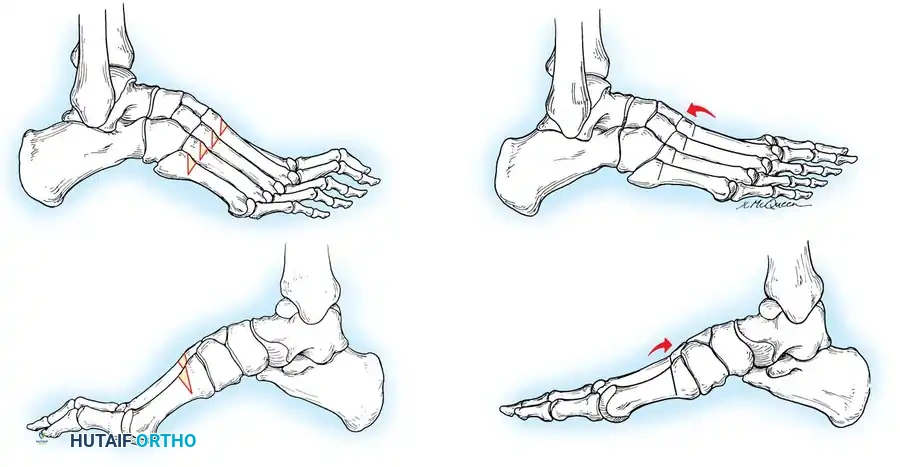
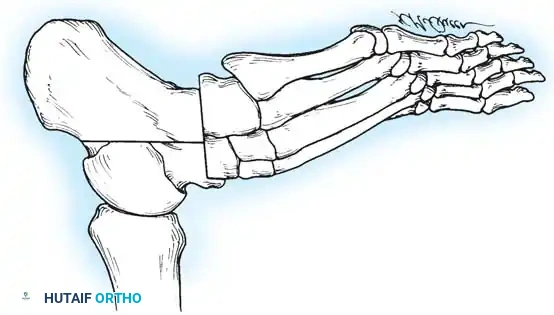
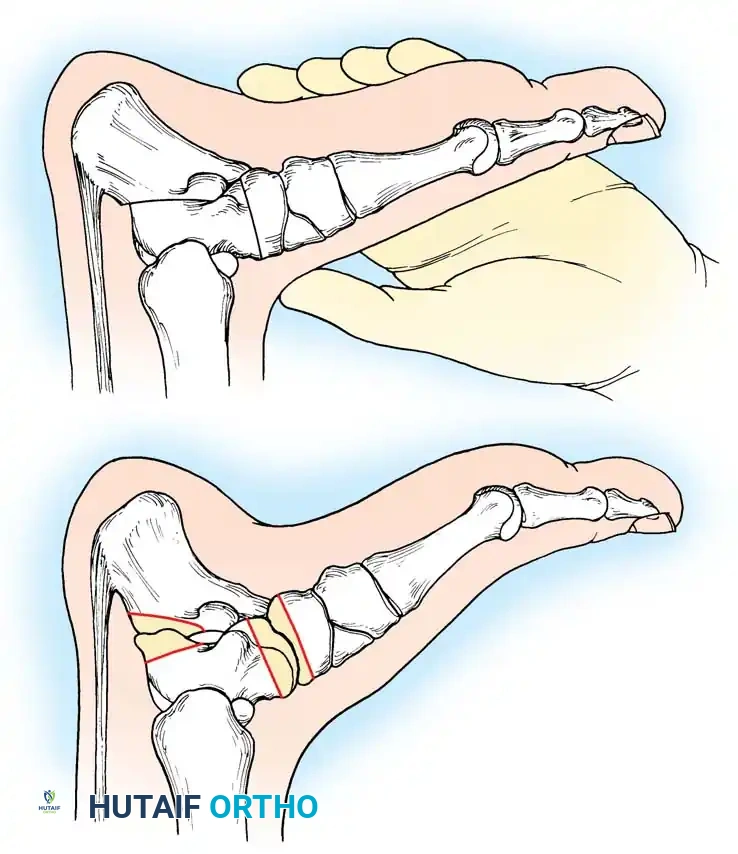
Fig. 3: Lateral and frontal view of a rigidly plantar flexed first ray, the hallmark of Charcot-Marie-Tooth disease.
As the first ray becomes rigidly plantarflexed, it acts as a kickstand. When the foot strikes the ground, the plantarflexed first metatarsal forces the hindfoot into a compensatory varus position. Over time, the plantar fascia contracts, and what began as a flexible, forefoot-driven hindfoot varus becomes a rigid, fixed bony deformity.
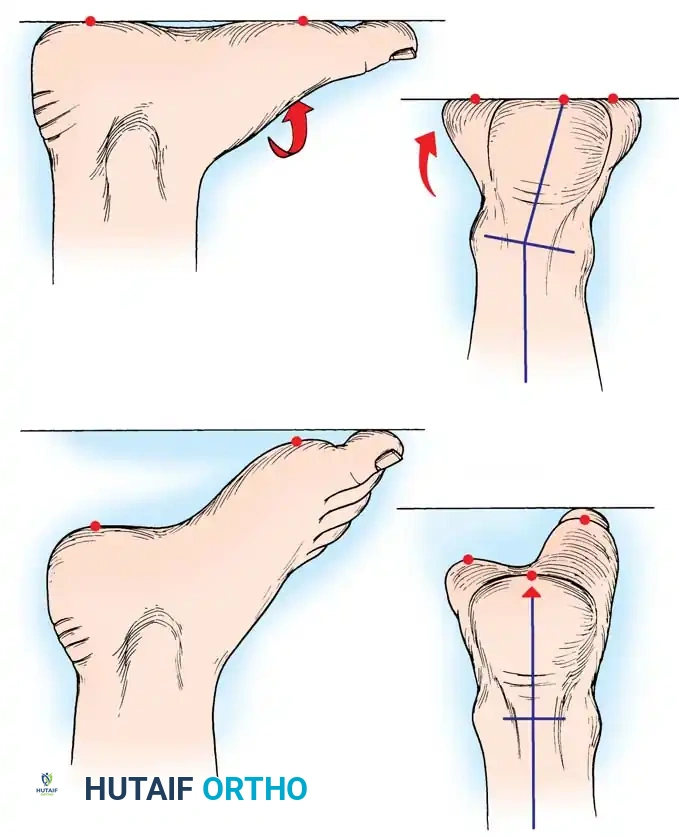
Fig. 4: The "Kickstand Effect." When the rigidly plantar flexed first ray strikes the ground, the heel is mechanically forced into varus.
Poliomyelitis Biomechanics
Patients with cavus deformity secondary to poliomyelitis present with a different pathoanatomical cascade. A weak gastrocnemius-soleus complex opposite a strong tibialis anterior causes a calcaneocavus deformity. The post-polio foot has distinct anterior and posterior components, contrasting with CMT patients who typically exhibit an equinocavus posture.

Fig. 5: Eighteen-year-old man with CMT demonstrating fixed hindfoot varus, marked forefoot equinus, tight plantar fascia, and contracted Achilles tendon.
Clinical Evaluation
A meticulous clinical examination is paramount. Patients with idiopathic, nonprogressive cavus deformities often present with metatarsalgia and callosities that correct with weight-bearing. Conversely, patients with progressive neuromuscular deficits present a complex reconstructive challenge.
The Coleman Block Test
The flexibility of the anatomical components of the cavus foot dictates the surgical algorithm. The Coleman and Chesnut block test is the gold standard for determining the hindfoot-forefoot relationship and assessing whether the hindfoot varus is flexible or fixed.
Technique:
1. The patient stands with the heel and lateral border of the foot on a 1-inch wooden block.
2. The plantarflexed first metatarsal is allowed to hang free off the medial edge of the block.
3. If the hindfoot varus corrects to neutral or valgus, the hindfoot is flexible, and the deformity is entirely driven by the forefoot (the plantarflexed first ray).
4. If the hindfoot remains in varus, the deformity is fixed, necessitating a calcaneal osteotomy or hindfoot arthrodesis.
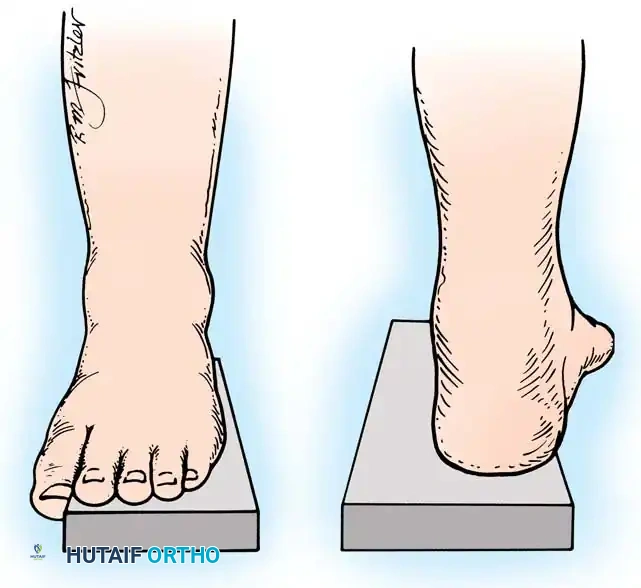
Fig. 6: Lateral block test. The plantar flexed first metatarsal hangs free; if the supple hindpart of the foot corrects, the varus is forefoot-driven.
Radiographic Evaluation
Brockway’s 1940 axiom remains true: "Cavus feet should never be operated upon until radiographs with the patient standing have been taken."
Standard weight-bearing anteroposterior (AP) and lateral radiographs of the foot, along with a weight-bearing AP of the ankle, are required.
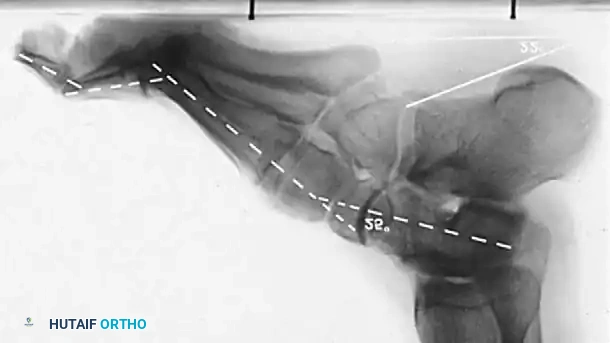
Key Radiographic Parameters:
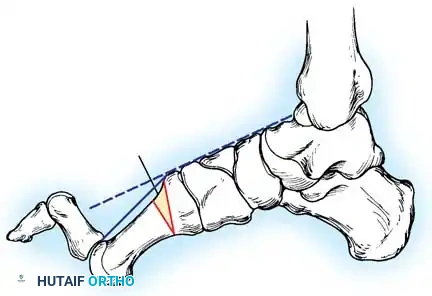
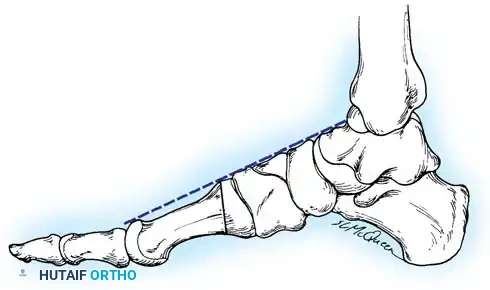
* Meary’s Angle (Talus-First Metatarsal Angle): Normally 0 degrees. In a cavus foot, the angle is convex upward (apex dorsal), indicating midfoot/forefoot equinus.
* Calcaneal Pitch: Normally 15 to 20 degrees. In a cavus foot, it is significantly increased (>30 degrees).
* Hibbs Angle: The angle between the longitudinal axis of the calcaneus and the first metatarsal. It approaches 90 degrees in severe cavus (normal is ~140 degrees).
* Talonavicular Coverage: Assessed on the AP view to quantify midfoot adduction.
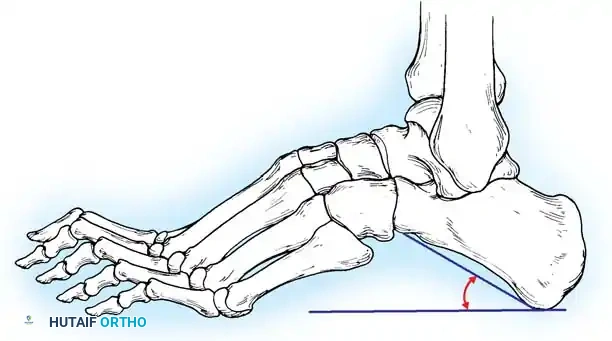
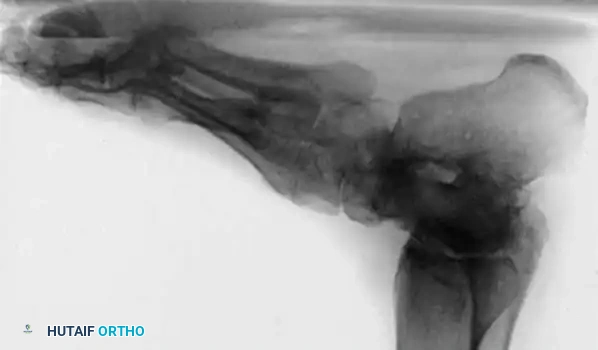
Fig. 7: Standing lateral radiograph demonstrating an increased calcaneal pitch and a severe apex-dorsal Meary's angle.
Nonoperative Management
Conservative management is primarily reserved for mild, flexible, idiopathic deformities or as a temporizing measure in patients unfit for surgery.
* Orthotics: Custom-molded total contact inserts with a lateral heel wedge (to accommodate, not correct, fixed varus) and a first ray cutout (to allow the plantarflexed first ray to drop, preventing secondary hindfoot varus).
* Shoe Modifications: Extra-depth shoes to accommodate claw toes, and metatarsal bars to relieve forefoot pressure.
* Physical Therapy: Stretching of the Achilles tendon and plantar fascia.
Surgical Management: Principles and Step-by-Step Approaches
The goal of surgery is to create a plantigrade, stable, and braceable foot while preserving as much joint mobility as possible. The surgical algorithm is dictated by the Coleman block test and the rigidity of the deformity.
Surgical Warning: Never attempt to correct a rigid cavovarus foot with soft-tissue procedures alone. Bony architecture must be realigned before tendon transfers are performed.
Phase 1: Soft Tissue Releases
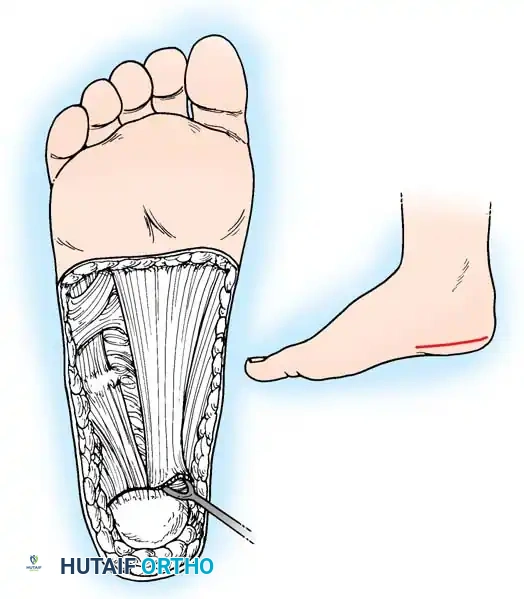
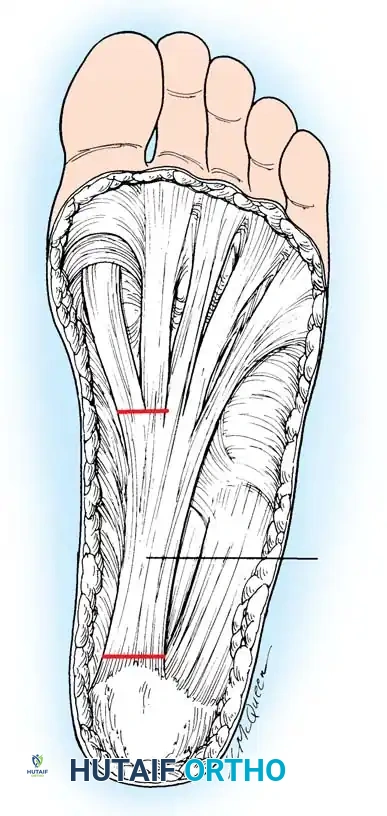
1. Plantar Fasciotomy (Steindler Stripping)
Almost all cavus reconstructions begin with a release of the contracted plantar fascia and intrinsic musculature.
* Positioning: Supine with a bump under the ipsilateral hip.
* Incision: A 3-cm medial longitudinal incision over the medial calcaneal tuberosity.
* Dissection: Identify the medial band of the plantar fascia. Retract the abductor hallucis muscle belly dorsally.
* Release: Sharply divide the plantar fascia off its calcaneal origin. In severe cases, the origin of the short flexors (Steindler stripping) is also released from the periosteum of the calcaneus.
Phase 2: Forefoot and Midfoot Bony Correction
If the Coleman block test demonstrates a flexible hindfoot, correcting the plantarflexed first ray will spontaneously correct the hindfoot varus.
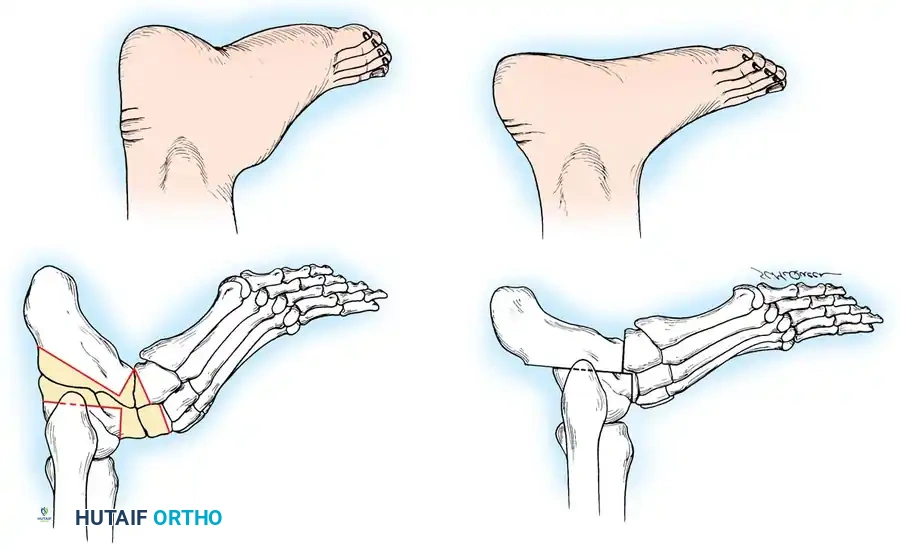
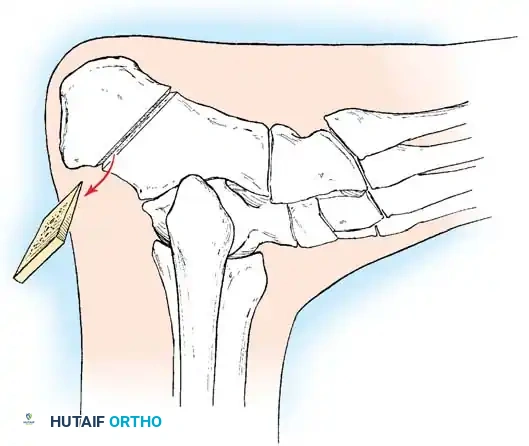
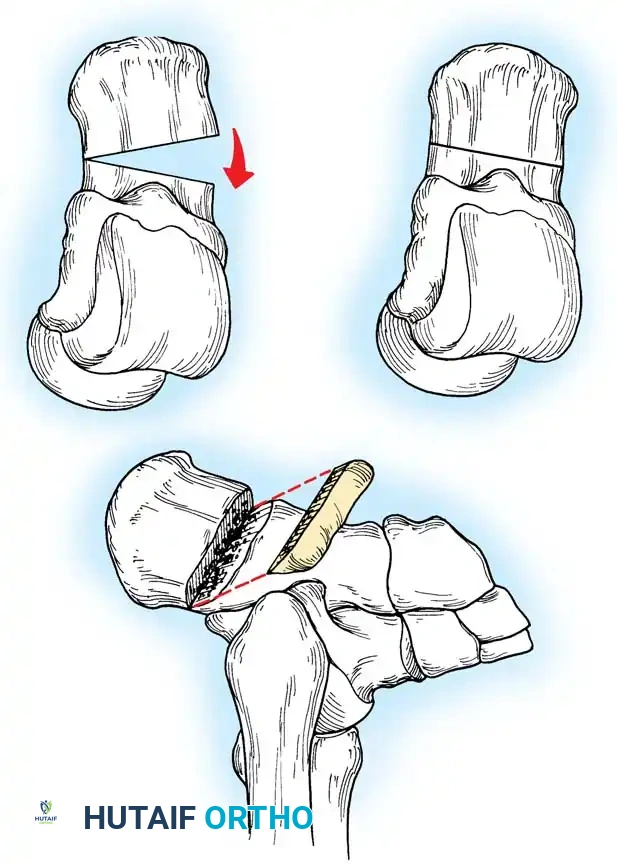
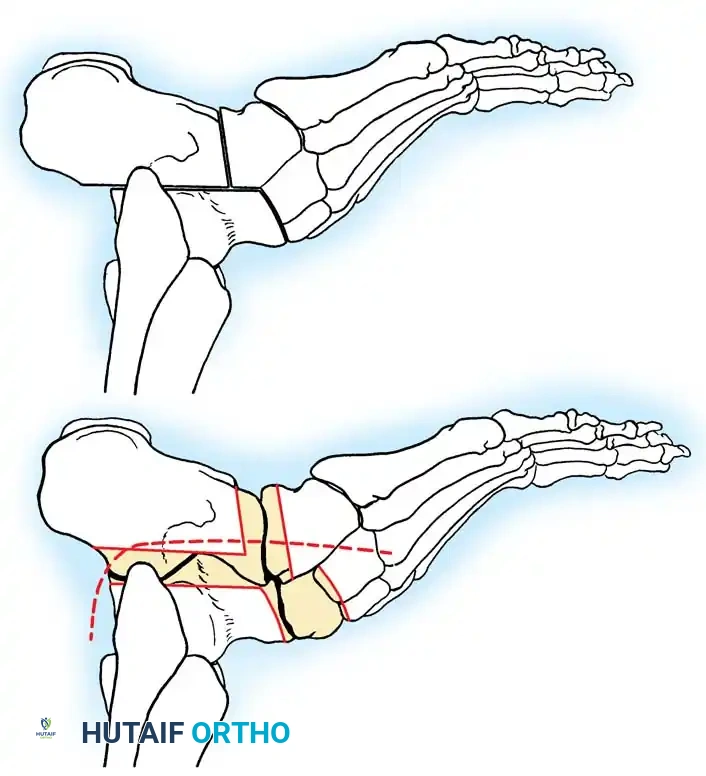
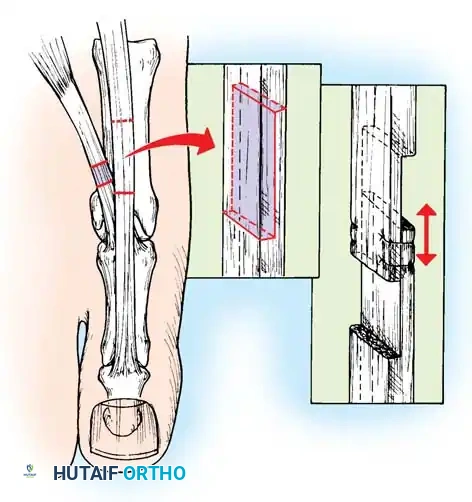
1. First Metatarsal Dorsiflexion Osteotomy
* Indications: Rigid plantarflexed first ray.
* Approach: Dorsal longitudinal incision over the proximal first metatarsal.
* Osteotomy: Protect the extensor hallucis longus (EHL) tendon. Perform a dorsal closing-wedge osteotomy approximately 1.5 cm distal to the tarsometatarsal joint.
* Fixation: Elevate the metatarsal head to neutral alignment with the lesser metatarsals. Fixate with a dorsal titanium plate, crossed K-wires, or a compression staple.
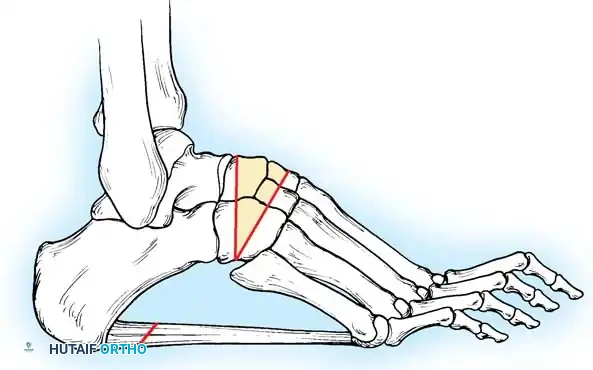
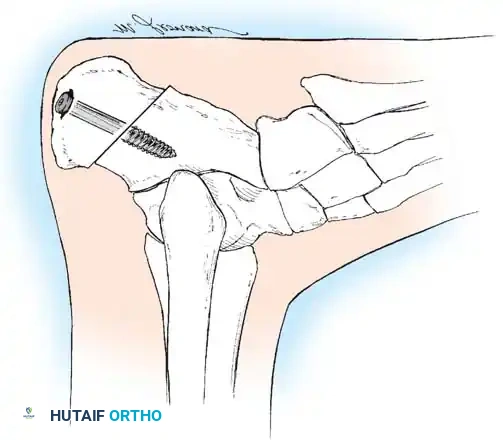
Fig. 8: Planning the dorsal closing wedge osteotomy of the first metatarsal to correct forefoot equinus.
Phase 3: Hindfoot Bony Correction
If the Coleman block test reveals a fixed hindfoot varus, a calcaneal osteotomy is mandatory.
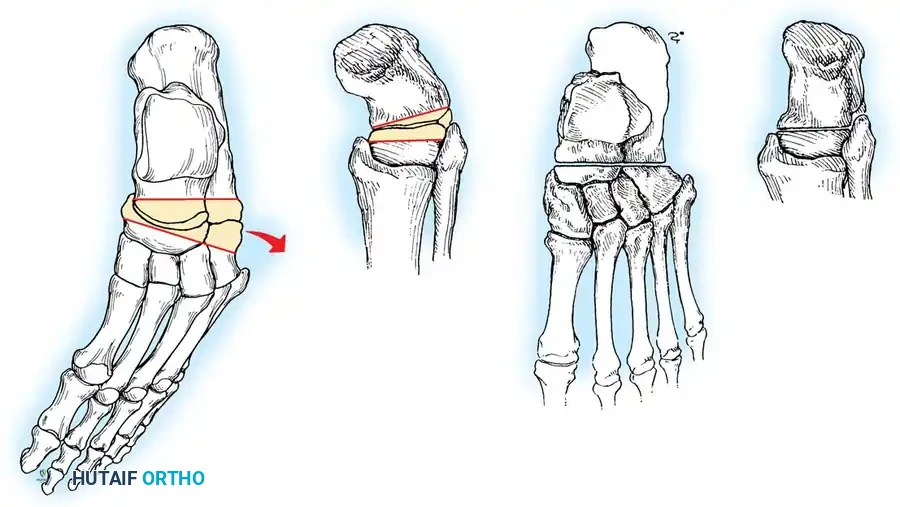
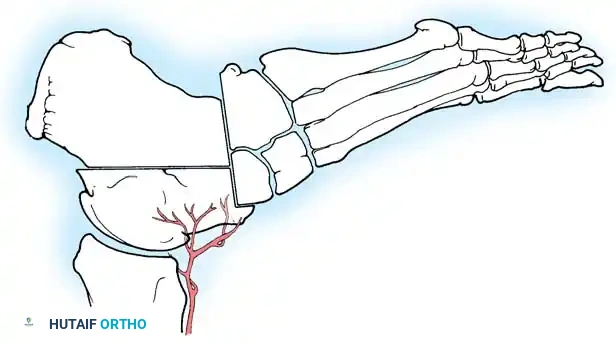
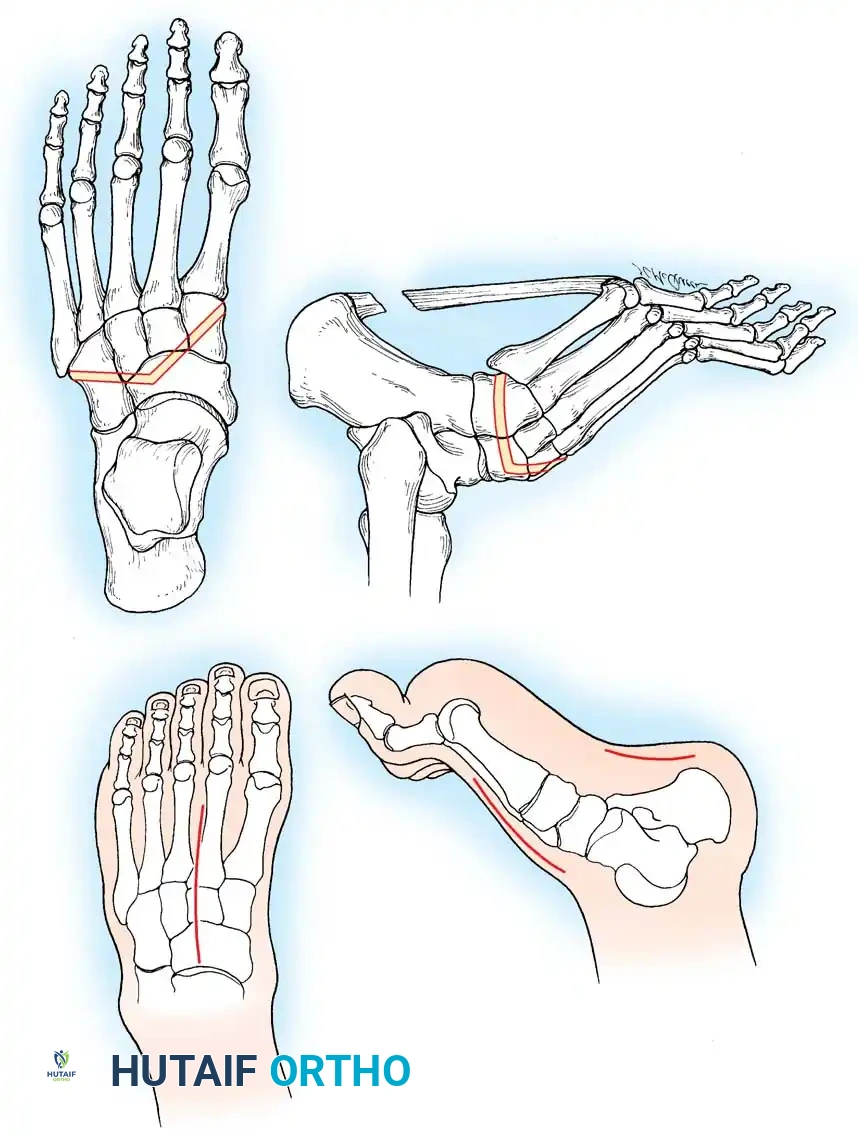
1. Lateralizing Calcaneal Osteotomy (Dwyer or Sliding)
* Indications: Fixed hindfoot varus with a preserved, non-arthritic subtalar joint.
* Approach: Oblique lateral incision posterior to the sural nerve and peroneal tendons.
* Osteotomy: A lateral closing-wedge (Dwyer) or a lateral sliding step-cut osteotomy is performed using an oscillating saw.
* Translation: The posterior tuberosity is translated laterally by 10 to 15 mm and rotated out of varus.
* Fixation: Secure with one or two large-fragment (6.5 mm or 7.3 mm) cannulated screws directed from the posterior heel into the anterior calcaneus.
Phase 4: Tendon Transfers
Once the bony architecture is plantigrade, muscle balance must be restored to prevent recurrence.
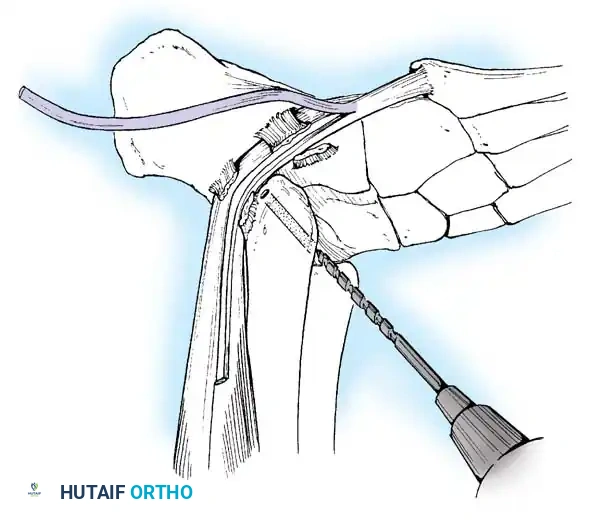
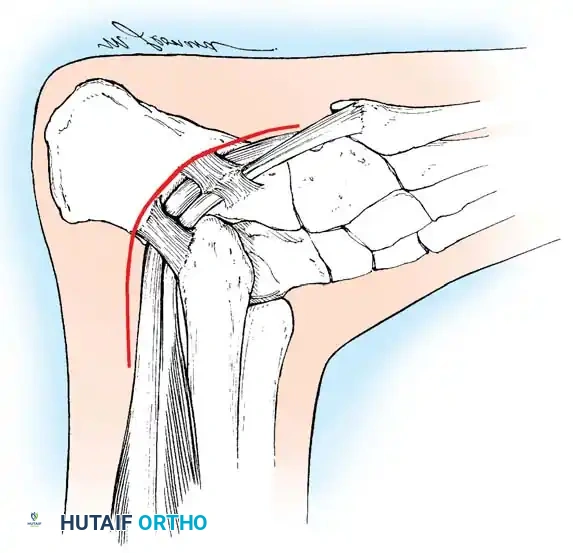
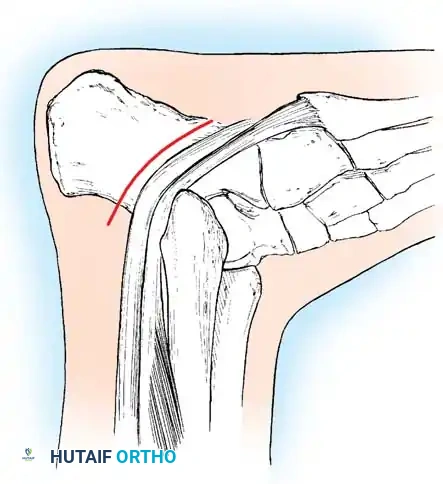
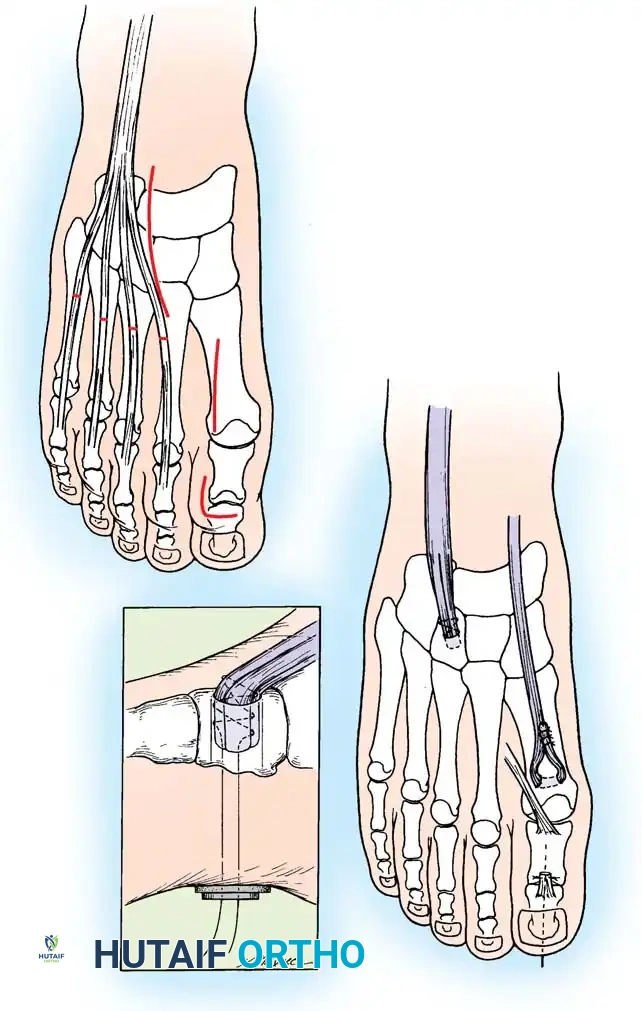
1. Peroneus Longus to Peroneus Brevis Transfer
* Rationale: Removes the deforming plantarflexion force on the first ray and augments eversion.
* Technique: Identify both tendons through a lateral incision over the cuboid. Transect the peroneus longus as distally as possible. Tenodese the proximal stump of the longus to the intact peroneus brevis tendon under physiological tension with the foot in neutral eversion.
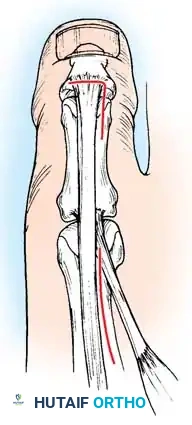
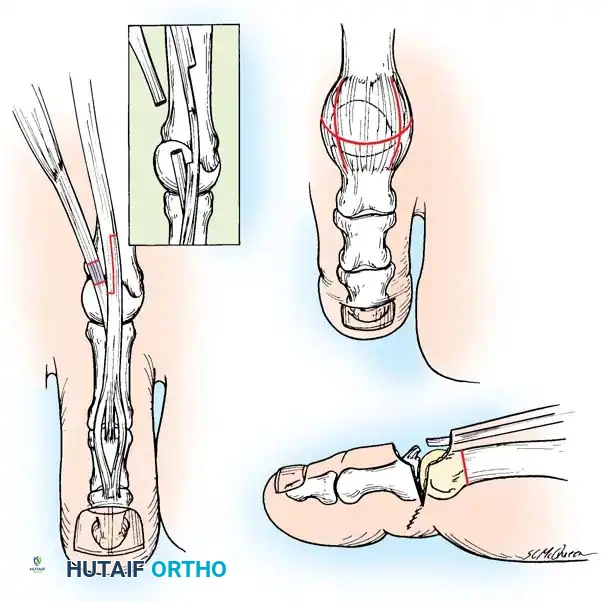
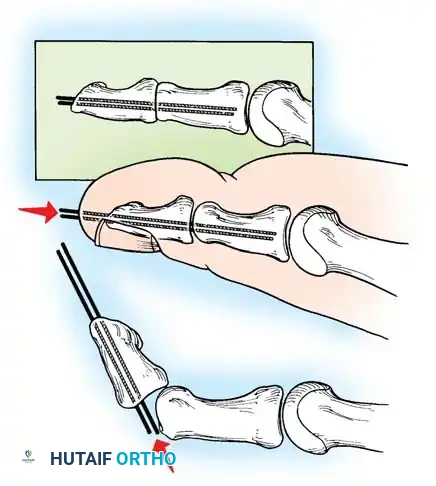
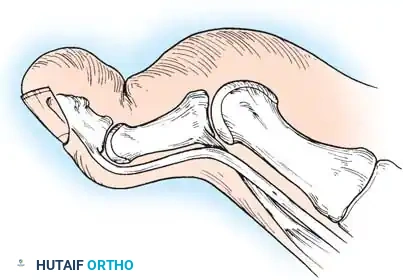
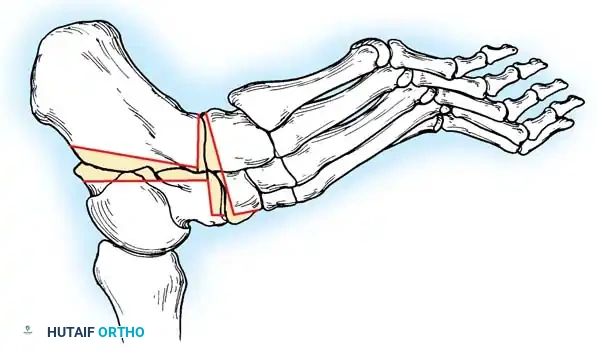
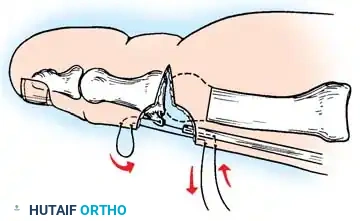
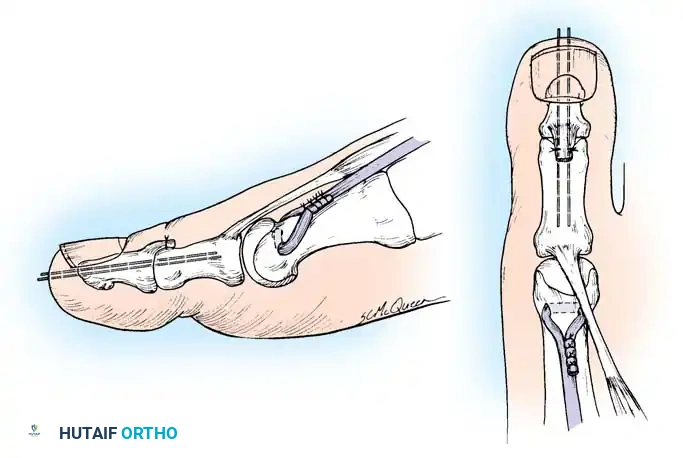
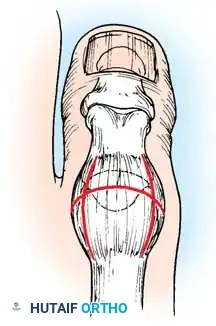
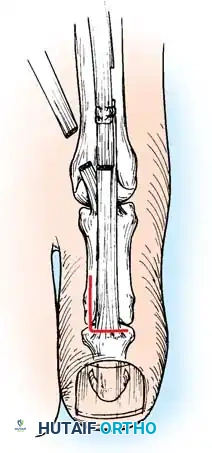
2. Jones Procedure (EHL to First Metatarsal Neck)
* Rationale: Corrects flexible clawing of the hallux and elevates the first ray.
* Technique: Transect the EHL at the IP joint. Reroute it through a drill hole in the neck of the first metatarsal and suture it back onto itself. The IP joint of the hallux must be arthrodesed to prevent a secondary drop-toe deformity.
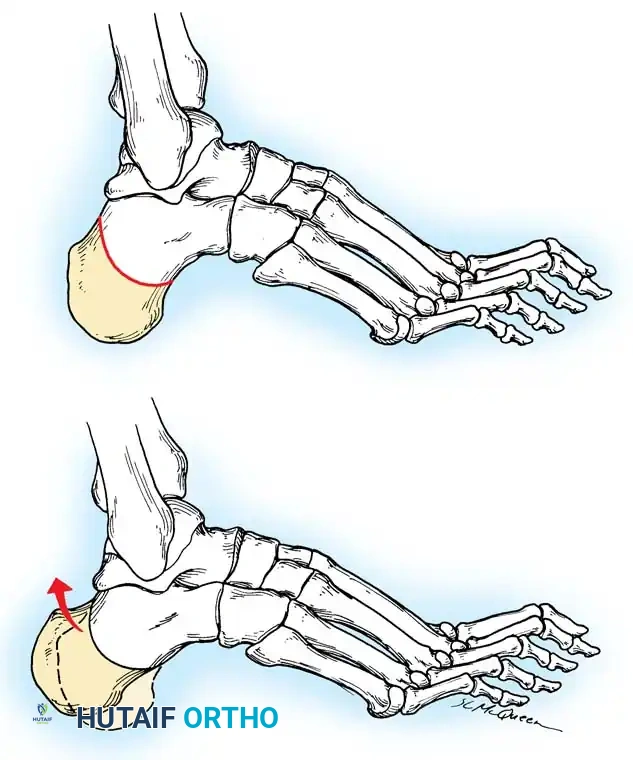
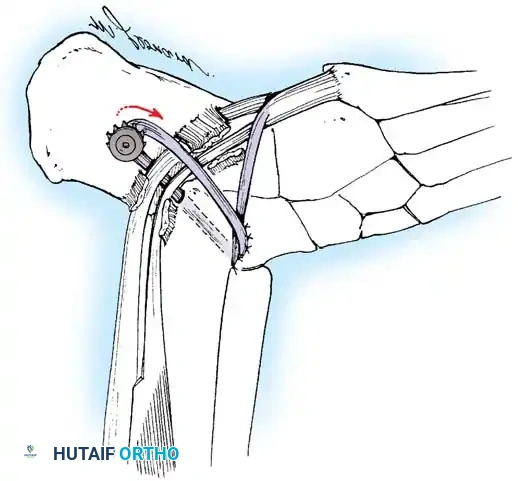
Fig. 9: Biomechanical routing for tendon transfers in the correction of claw toe and forefoot equinus.
Phase 5: Salvage Procedures (Triple Arthrodesis)
In older patients with severe, rigid, neglected deformities, or those with advanced degenerative joint disease of the subtalar and transverse tarsal joints, joint-sparing osteotomies will fail.
Triple Arthrodesis
* Joints Included: Subtalar, talonavicular, and calcaneocuboid joints.
* Technique: Extensive medial and lateral approaches are required. Aggressive biplanar wedge resections are necessary to correct the rigid varus and midfoot cavus. The joints are rigidly fixed with large-fragment screws and anatomic plates.
* Caveat: While powerful, triple arthrodesis sacrifices hindfoot motion and increases stress on the ankle joint, potentially accelerating ankle osteoarthritis in the long term.
Postoperative Protocols and Rehabilitation
Meticulous postoperative care is critical to the success of cavus foot reconstruction.
- 0 to 2 Weeks: The patient is placed in a bulky, non-weight-bearing (NWB) posterior splint. Strict elevation is enforced to mitigate edema and prevent wound breakdown, which is a high risk over the lateral calcaneal incision.
- 2 to 6 Weeks: Sutures are removed. The patient is transitioned to a NWB short-leg cast.
- 6 to 10 Weeks: Radiographs are obtained to confirm bony consolidation of osteotomies/arthrodeses. If healing is adequate, the patient is transitioned to a controlled ankle motion (CAM) boot and begins progressive partial weight-bearing.
- 10+ Weeks: Transition to supportive athletic shoes with custom orthotics. Physical therapy focuses on proprioception, peroneal strengthening, and gait retraining.
Complications and Pitfalls
- Under-correction: The most common pitfall is failing to recognize a fixed hindfoot varus, leading to omission of the calcaneal osteotomy. The deformity will rapidly recur.
- Over-correction: Excessive lateral translation of the calcaneus or over-dorsiflexion of the first metatarsal can result in a painful flatfoot (pes planovalgus) and transfer metatarsalgia to the lesser metatarsals.
- Wound Healing: The lateral incision for the calcaneal osteotomy is notoriously prone to dehiscence, especially in patients with CMT who may have compromised microvascular tone.
- Nerve Injury: The sural nerve is at high risk during the lateral calcaneal approach; meticulous retraction is mandatory.
In conclusion, the operative management of the cavus foot is a formidable orthopedic challenge. It demands a rigorous preoperative assessment of flexibility, a deep understanding of the deforming neuromuscular forces, and a meticulously executed
Associated Surgical & Radiographic Imaging












📚 Medical References
- Cavus foot in cerebral palsy, Foot Ankle 4:185, 1984.
- Engstrom A, Erikson V, Hjelmstedt A: The results of extraarticular subtalar arthrodesis according to the Green-Grice method in cerebral palsy, Acta Orthop Scand 45:945, 1974.
- Fulford GE: Surgical management of ankle and foot deformities in cerebral palsy, Clin Orthop Relat Res 253:55, 1990.
- Gaines RW, Ford TD: A systematic approach to the amount of Achilles tendon lengthening in cerebral palsy, J Pediatr Orthop 4:448, 1984.
- Garbarino JL, Clancy M: A geometric method of calculating tendo Achilles lengthening, J Pediatr Orthop 5:573, 1985.
- Graham HK, Fixsen JA: Lengthening of the calcaneal tendon in spastic hemiplegia by the White slide technique: a long-term review, J Bone Joint Surg 70B:472, 1988.
- Green NE, Griffi n PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy, J Bone Joint Surg 65A:748, 1983.
- Greene WB: Achilles tendon lengthening in cerebral palsy: comparison of inpatient versus ambulatory surgery, J Pediatr Orthop 7:256, 1987.
- Grice DS: An extra-articular arthrodesis of the subastragalar joint for correction of paralytic fl at feet in children, J Bone Joint Surg 34A:927, 1952.
- Grice DS: Further experience with extra-articular arthrodesis of the subtalar joint, J Bone Joint Surg 36A:246, 1955.
- Grice DS: The role of subtalar fusion in the treatment of valgus deformities of the feet, Instr Course Lect 16:127, 1959.
- Gritzka TL, Staheli LT, Duncan WR: Posterior tibial tendon transfer through the interosseous membrane to correct equinovarus deformity in cerebral palsy: an initial experience, Clin Orthop Relat Res 89:201, 1972.
- Gross RH: A clinical study of the Batchelor subtalar arthrodesis, J Bone Joint Surg 58A:343, 1976.
- Guttman G: Modifi cation of the Grice-Green subtalar arthrodesis in children, J Pediatr Orthop 1:219, 1981.
- Hadley N, Rahm M, Cain TE: Dennyson-Fulford subtalar arthrodesis, J Pediatr Orthop 14:363, 1994.
- Hauser ED: Diseases of the foot, Philadelphia, 1939, Saunders. Hicks R, Durinick N, Gage JR: Differentiation of idiopathic toe-walking and cerebral palsy, J Pediatr Orthop 8:160, 1988.
- Hiroshima K, Hamada S, Shimizu N, et al: Anterior transfer of the long toe fl exors for the treatment of spastic equinovarus and equinus foot in cerebral palsy, J Pediatr Orthop 8:164, 1988.
- Hoffer MM, Perry J: Pathodynamics of gait alterations in cerebral palsy and the signifi cance of kinetic electromyography in evaluating foot and ankle problems, Foot Ankle 4:128, 1983.
- Hoffer MM, Reiswig JA, Garrett AM, et al: The split
You Might Also Like

