Calcaneonavicular Bar Resection: Surgical Technique
Key Takeaway
Calcaneonavicular bar resection is the primary surgical intervention for symptomatic calcaneonavicular tarsal coalitions failing conservative management. The procedure utilizes an Ollier approach to expose the sinus tarsi, followed by radical excision of the bony or cartilaginous bar. To prevent recurrence, the extensor digitorum brevis muscle is interposed into the defect. In cases of advanced degenerative arthritis or failed resection, a triple arthrodesis serves as the definitive salvage procedure.
PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
Tarsal coalitions represent a failure of mesenchymal segmentation during embryonic development, resulting in abnormal fibrous, cartilaginous, or osseous connections between adjacent tarsal bones. The calcaneonavicular coalition is one of the two most common types (alongside talocalcaneal coalitions) and typically presents in patients between 8 and 14 years of age as the cartilaginous bar begins to ossify and restrict normal peritalar motion.
Biomechanically, the subtalar and transverse tarsal joints function as a coupled unit (the coxa pedis). A calcaneonavicular bar rigidly tethers the anterior process of the calcaneus to the navicular, eliminating the normal kinematics of the hindfoot. This restriction leads to a rigid, painful flatfoot deformity, recurrent ankle sprains, and secondary "peroneal spasticity"—which is not a true neurologic spasticity, but rather a protective, reflex muscle spasm of the peroneal musculature attempting to splint the painful subtalar joint.
💡 Clinical Pearl
Always evaluate the flexibility of the hindfoot. A rigid valgus hindfoot that does not correct with the Jack test (great toe extension) or heel-rise test is highly suspicious for a tarsal coalition.
PREOPERATIVE PLANNING AND IMAGING
Thorough radiographic evaluation is mandatory before proceeding with a calcaneonavicular bar resection. Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the foot should be obtained. The 45-degree internal oblique view is the gold standard for visualizing a calcaneonavicular bar, which will appear as a solid bony bridge or an irregular, sclerotic pseudoarticulation between the anterior process of the calcaneus and the navicular.
Advanced imaging, particularly Computed Tomography (CT), is highly recommended to delineate the exact size of the coalition, assess for multiple coalitions (e.g., a concomitant middle facet talocalcaneal coalition), and evaluate the presence of degenerative arthritic changes in the talonavicular or subtalar joints.

FIGURE 82-79 A: Harris-Beath axial calcaneal (coalition) view utilized to identify middle facet tarsal coalitions. Note the normal middle facet on the right and an incomplete middle facet coalition on the left.
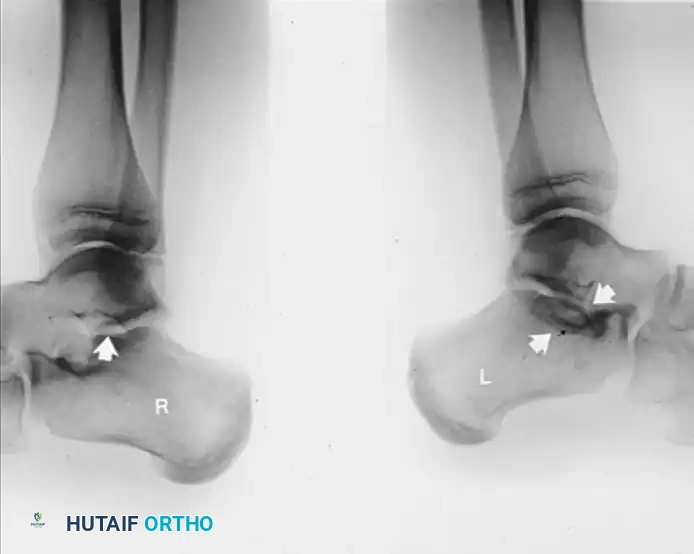
FIGURE 82-79 B: Lateral radiograph of the hindfeet of the same patient. Note the normal middle and posterior facets on the right. On the left, observe the loss of normal “space” at the middle facet, rounding of the lateral process of the talus, and a sclerotic semicircle in the calcaneus inferior to the middle facet, representing the overlap of the cortical margins of the sustentaculum and the bony bar.
SURGICAL INDICATIONS AND CONTRAINDICATIONS
Indications
- Symptomatic calcaneonavicular coalition failing conservative management (e.g., cast immobilization, custom orthotics, NSAIDs).
- Patient age typically between 8 and 14 years (prior to the onset of adaptive degenerative changes).
- Absence of advanced peritalar arthritis.
Contraindications
- Absolute: Active local infection, severe peripheral vascular disease.
- Relative: Advanced patient age (older adolescents or adults) with established degenerative arthritis in the subtalar or talonavicular joints. In these cases, isolated resection often fails to relieve pain, and primary arthrodesis is preferred.
- Concomitant, large talocalcaneal coalitions that dictate a primary fusion approach.
SURGICAL TECHNIQUE: CALCANEONAVICULAR BAR RESECTION
Patient Positioning and Anesthesia
The patient is placed in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg, providing excellent access to the lateral aspect of the foot. A well-padded thigh or calf tourniquet is applied. Regional anesthesia (popliteal block) combined with general anesthesia or deep sedation is preferred for optimal postoperative pain control.
Exposure of the Bar (Ollier Approach)
- Incision: Make an Ollier incision over the lateral aspect of the hindfoot. The incision begins at the dorsolateral margin of the talonavicular joint and extends obliquely and plantarward toward the inferior tip of the lateral malleolus.
- Nerve Protection: Carefully dissect through the subcutaneous tissues. It is critical to identify and preserve the branches of the intermediate dorsal cutaneous nerve (a branch of the superficial peroneal nerve) that cross the superior aspect of the incision.
- Tendon Sheath Preservation: Try to preserve the sheaths of the extensor digitorum longus and peroneus tertius tendons anteriorly, as well as the peroneal tendons posteriorly. Retract the peroneal tendons inferiorly and the extensor tendons superiorly.
- Muscle Elevation: Identify the muscle belly of the extensor digitorum brevis (EDB). Raise the muscle by sharp dissection from the confines of the sinus tarsi in a proximal-to-distal direction. Continue elevation until the entire sinus tarsi and the anterior process of the calcaneus are fully exposed.
Identification and Resection of the Bar
- Joint Identification: Identify the talonavicular and calcaneocuboid joints by manually rocking the forefoot-midfoot segment on the hindfoot. The calcaneonavicular bar runs from the anterior process of the calcaneus (just lateral to the anterior facet) anteriorly and medially to the lateral and dorsolateral margin of the navicular.
- Capsulotomy (If Necessary): If the exact location of the articular margins of the calcaneocuboid or talonavicular joints is questionable, open the capsules of these joints just enough to definitively identify the articular surfaces.

FIGURE 82-77 A: Diagrammatic representation of the calcaneonavicular tarsal coalition prior to surgical resection.
- Retraction: Use small Hohmann retractors placed carefully around the waist of the bar to protect surrounding soft tissues and improve exposure.
- Osteotomy Execution: At the calcaneal origin of the bar, place a 1/2-inch osteotome parallel to the floor of the sinus tarsi. Cut up to, but not completely through, the medial cortex of the bar.

FIGURE 82-78 A: Initial positioning of the osteotome for resection of the calcaneonavicular tarsal coalition.
- Direction of the Cut: Direct the upper cut at the dorsolateral aspect of the navicular medially, plantarward, and obliquely at an angle of approximately 30 degrees from the vertical plane. Complete this osteotomy through the bar.

FIGURE 82-78 B: Direction of the osteotome. Note the oblique, plantarward trajectory designed to safely excise the bar without violating the adjacent articular surfaces.
- Fracture and Excision: By placing the osteotome in the inferior cut, gently lever and fracture the bar through its medial cortex. Remove the rectangular piece of bone. Smooth the remaining medial cortical margins with a rongeur or a high-speed burr.
- Surgical Rationale: This specific geometric resection reduces the chance of iatrogenic damage to the anterior facet of the subtalar joint or the inferior aspect of the head and neck of the talus.
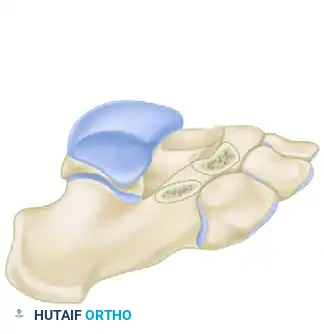
FIGURE 82-78 C: The surgical site after complete resection of the bony bar, demonstrating the resulting rectangular defect.
⚠️ Surgical Warning: Radical Resection is Mandatory
Generous resection of the bar is highly recommended to prevent recurrence. The most common surgical error is removing less than an optimal amount of bone.
- Verification of Resection: We strongly recommend a lateral oblique radiographic examination on the operating table after resection to confirm adequate removal. Usually, a 1.5- to 2.5-cm segment of the bar must be removed. Ensure that the lateral fourth of the articular surface of the talus is left uncovered by the navicular; this serves as an anatomic landmark confirming adequate excision.
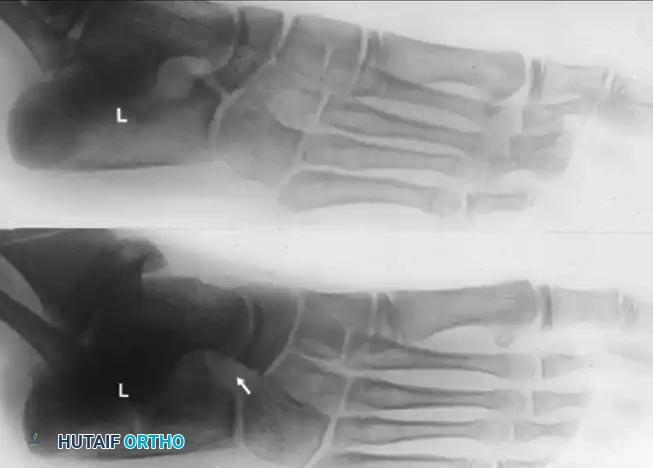
FIGURE 82-77 B: Diagrammatic representation of the surgical site after adequate resection of the calcaneonavicular bar.
Interposition of Muscle (Extensor Digitorum Brevis)
To prevent hematoma organization and subsequent re-ossification (recurrence of the bar), the dead space must be filled with vascularized tissue.
1. Suture Placement: Using a heavy absorbable suture (e.g., #1 Vicryl), weave a Krackow or figure-of-eight stitch through the proximal margin of the mobilized extensor digitorum brevis muscle belly.
2. Muscle Transposition: Interpose the muscle deep into the depths of the bony defect. Pass a small, straight Keith needle medially through the defect, exiting the medial skin of the midfoot, carrying the suture and drawing the muscle belly directly into the resected space.
3. Securing the Muscle: Bring the ends of the suture out through the skin medially, pass them through a broad felt pad or sterile button, and tie them firmly over the medial aspect of the foot.
4. Alternative: If the EDB is insufficient or damaged, the use of bone wax combined with Gelfoam applied directly to the raw cancellous bone surfaces is an acceptable alternative to muscle interposition.
Closure
- Deflate the tourniquet and secure meticulous hemostasis. Hematoma prevention is critical to reducing the risk of heterotopic ossification.
- Close the subcutaneous tissues and skin with absorbable sutures.
- Apply a well-padded, short-leg cast in the operating room while the foot is held in a neutral position.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the soft tissue repair while initiating early motion to prevent arthrofibrosis.
* Phase 1 (0-3 Weeks): The initial non-weight-bearing short-leg cast remains in place for 3 weeks, provided that the neurovascular status of the foot is satisfactory.
* Phase 2 (3-6 Weeks): At 3 weeks, the cast is removed. The transcutaneous medial retention suture (if used for the EDB) is cut and removed. Active, and gentle active-assisted, inversion-eversion range-of-motion exercises are begun immediately. Weight-bearing to tolerance with the aid of crutches is initiated.
* Phase 3 (>6 Weeks): Crutches are discontinued when full weight-bearing is comfortable. Physical therapy focuses on peroneal strengthening, proprioception, and restoring peritalar kinematics.
📊 Expectation Management
Although subtalar motion reliably improves following successful resection, it rarely equals that of the uninvolved side in unilateral cases. Achieving 50% of normal subtalar motion is considered a good clinical result. The patient and parents must clearly understand this limitation prior to surgery.
SALVAGE PROCEDURES AND ARTHRODESIS
Subtalar Arthrodesis
In cases where isolated subtalar arthritis is present, or if a concomitant middle facet coalition was addressed but failed, an isolated subtalar arthrodesis may be indicated.
Triple Arthrodesis for Calcaneonavicular Coalition
In an older adolescent or adult, resection of a complete bony bar between the calcaneus and the navicular may not improve subtalar motion or relieve symptoms. This is especially true if there is radiographic evidence of degenerative arthritis in the subtalar or talonavicular joints.
If the findings of arthritis are mild and consist primarily of talonavicular beaking (a traction osteophyte rather than true degenerative joint disease), the option of bar resection versus triple arthrodesis can be discussed with the patient. However, the definitive salvage for a failed bar resection, regardless of patient age, is a triple arthrodesis. We strongly prefer primary triple arthrodesis in adults or in patients with established degenerative changes in the peritalar joint complex.
Surgical Considerations for Triple Arthrodesis:
* In Situ vs. Corrective: If the hindfoot is in an acceptable, plantigrade position, an in situ triple arthrodesis is performed. If the position of the hindfoot must be corrected (e.g., severe rigid valgus), the calcaneonavicular bar must first be removed to mobilize the joints. Appropriate wedge resections of the articular surfaces at the subtalar and midtarsal joints are then made to anatomically reposition the hindfoot.
* Incision Strategy: A medial incision may not strictly be needed when performing a triple arthrodesis in the calcaneonavicular form of coalition. However, in adults, the additional medial exposure is highly helpful for adequately denuding the most medial aspect of the talar head and, especially, the navicular to ensure a robust fusion mass.
You Might Also Like
