Anterior Calcaneal Osteotomy: Lateral Column Lengthening Guide
Key Takeaway
The anterior calcaneal osteotomy, or lateral column lengthening, is a powerful surgical technique utilized to correct severe flexible flatfoot deformities. By inserting a structural graft into the anterior calcaneus, surgeons can effectively restore the medial longitudinal arch and correct forefoot abduction. This comprehensive guide details the biomechanical principles, strict patient selection criteria, step-by-step surgical execution, and evidence-based postoperative protocols essential for optimizing patient outcomes and minimizing complications like nonunion or adjacent joint arthritis.
INTRODUCTION TO LATERAL COLUMN LENGTHENING
The anterior calcaneal osteotomy, frequently referred to as lateral column lengthening (LCL) or the Evans osteotomy, is a cornerstone procedure in the surgical management of adult acquired flatfoot deformity (AAFD), specifically secondary to posterior tibial tendon insufficiency (PTTI). Extensively studied in both biomechanical laboratories and clinical settings, this procedure has proven highly efficacious in correcting multiplanar peritalar subluxation.
By strategically lengthening the lateral column of the foot, the osteotomy acts as a structural wedge that indirectly reduces the talonavicular joint, significantly improves forefoot abduction, and restores the height of the medial longitudinal arch. While clinical studies often characterize the outcomes of flatfoot reconstruction as intermediate due to the progressive nature of the disease, meticulous execution of the anterior calcaneal osteotomy yields high rates of patient satisfaction and functional restoration when applied to the correct indications.
BIOMECHANICS AND CLINICAL EVIDENCE
The fundamental biomechanical principle of the anterior calcaneal osteotomy relies on the concept of the foot as a functional triangle. Shortening of the medial column or lengthening of the lateral column effectively adducts the midfoot and forefoot around the talus. Lengthening the calcaneus 1.0 to 1.5 cm proximal to the calcaneocuboid (CC) joint tensions the plantar fascia and the long plantar ligament, creating a "windlass-like" effect that elevates the arch and corrects the characteristic "too-many-toes" sign associated with forefoot abduction.
Evidence-Based Outcomes
The literature robustly supports the use of LCL in appropriately selected patients:
* Hinterman and Gachter: In a review of 19 patients treated with lateral column lengthening combined with medial soft tissue reconstruction for Stage II and III PTTI, outcomes were highly favorable. At a mean follow-up of approximately 2 years, 18 of 19 patients were satisfied. Clinical results were rated as excellent in 6, good in 11, and fair in 2 patients.
* Bolt et al.: In a direct comparison between lateral column lengthening and medial displacement calcaneal osteotomy (MDCO), Bolt and colleagues found that LCL achieved superior initial radiographic realignment and maintained this correction more effectively over time. Furthermore, LCL demonstrated a lower overall reoperation rate, despite a higher incidence of nonunion and radiographic progression of adjacent calcaneocuboid joint arthritis.
Clinical Pearl: While LCL provides superior multiplanar correction compared to MDCO, the increased risk of lateral column overload and CC joint arthritis dictates that it should be reserved for patients with significant, flexible forefoot abduction that cannot be corrected by medializing the heel alone.
INDICATIONS AND PATIENT SELECTION
Patient selection is the most critical determinant of success in lateral column lengthening. The procedure is highly powerful but unforgiving in the presence of contraindications.
Primary Indications:
* Stage IIb Adult Acquired Flatfoot Deformity (PTTI) characterized by significant forefoot abduction (>30% talonavicular uncoverage on standing AP radiographs).
* A flexible hindfoot and midfoot.
* Failure of exhaustive conservative management (custom orthotics, AFOs, physical therapy).
Ideal Patient Profile:
In our extensive clinical experience, this procedure is most successful in patients who meet the following strict criteria:
* Weight: Patients weighing less than 170 to 180 pounds. Heavier patients exert excessive force on the lateral column graft, significantly increasing the risk of graft collapse, nonunion, and hardware failure.
* Deformity: Presence of a distinct abduction deformity of the forefoot on standing anteroposterior (AP) radiographs.
* Flexibility: A fully flexible hindfoot without fixed forefoot supination. If fixed forefoot supination is present, a concurrent medial column procedure (e.g., plantarflexing first tarsometatarsal arthrodesis or naviculocuneiform arthrodesis) is mandatory to ensure a plantigrade foot.
Contraindications:
* Rigid or fixed hindfoot deformity (requires triple arthrodesis).
* Severe pre-existing calcaneocuboid joint arthritis.
* Morbid obesity (>180 lbs is a relative contraindication; >250 lbs is an absolute contraindication for isolated LCL).
* Severe peripheral neuropathy or vascular compromise.
PREOPERATIVE PLANNING AND GRAFT SELECTION
Graft Options
The choice of interpositional graft is critical for maintaining the lengthened lateral column while bony union occurs.
* Tricortical Iliac Crest Autograft: Historically the gold standard, providing osteoconductive, osteoinductive, and osteogenic properties.
* Tricortical Allograft: Studies by Grier et al. and Dolan et al. have demonstrated that structural allograft (e.g., femoral head, iliac crest, or patellar wedges) yields roughly equivalent healing and complication rates compared to autograft, while eliminating donor-site morbidity.
Depending on the size of the patient and the severity of the deformity, the graft should typically measure 8 to 10 mm in width.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Medial Soft Tissue Preparation
The procedure begins on the medial side of the foot. The posterior tibial tendon is debrided or excised depending on its viability. The flexor digitorum longus (FDL) tendon is harvested and prepared for transfer into the navicular.
If the spring ligament is severely attenuated, a reconstruction using a peroneus longus autograft tendon transfer may be performed. The medial soft tissues are prepared, and bone tunnels are drilled, but final tensioning is delayed until after the lateral column lengthening is complete to avoid tearing the medial repair during lateral distraction.
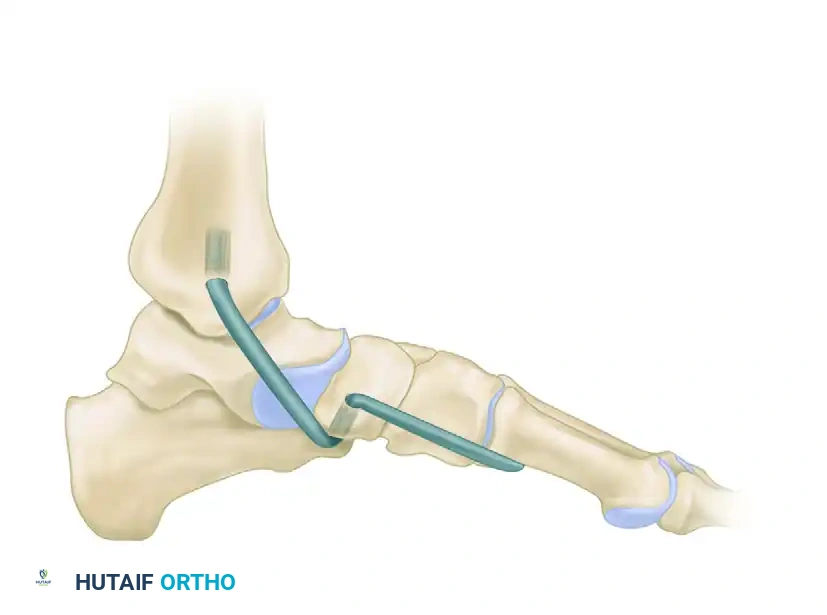
Figure 1: Reconstruction of the spring ligament using a peroneus longus autograft tendon transfer. Lateral view demonstrating the calcaneal bone tunnel reconstruction.
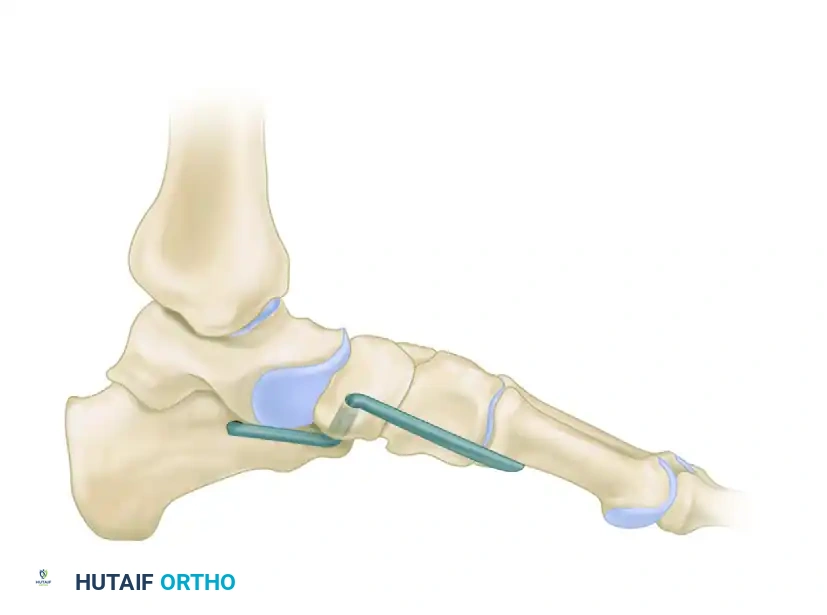
Figure 2: Anteroposterior view demonstrating the tibial bone tunnel reconstruction for spring ligament augmentation.
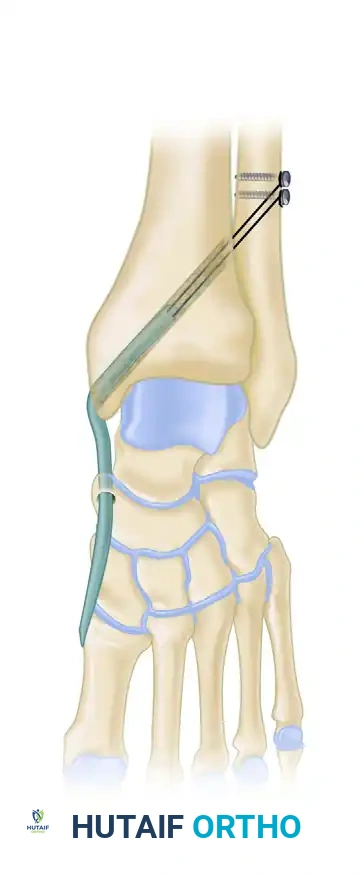
Figure 3: Lateral view detailing the tibial bone tunnel reconstruction trajectory.
2. Lateral Approach and Exposure
- Make a 4 to 5 cm longitudinal incision over the lateral anterior process of the calcaneus, centered approximately 1.5 cm proximal to the calcaneocuboid joint.
- Surgical Warning: Take meticulous care to identify, mobilize, and protect the sural nerve, which frequently crosses the operative field.
- Elevate the extensor digitorum brevis (EDB) muscle belly dorsally to expose the anterior process of the calcaneus and the CC joint.
- Identify the peroneal tendons and retract them plantarly.
3. The Osteotomy
- Identify the calcaneocuboid joint line using a Keith needle or fluoroscopy.
- Perform the osteotomy 1.0 to 1.5 cm proximal to the articular surface of the calcaneocuboid joint using an oscillating sagittal saw.
- Trajectory: Aim the saw carefully between the anterior facet and the middle facet of the calcaneus.
Surgical Pitfall: Do not plunge the saw blade through the medial cortex. Overpenetration risks catastrophic injury to the medial soft tissues, specifically the medial plantar nerve and artery, as well as the FHL tendon. Complete the medial cortex osteotomy with a sharp osteotome.
4. Distraction of the Osteotomy
- Distract the osteotomy site using a combination of manual adduction of the forefoot and mechanical distraction.
- Place two 3/32-inch Steinmann pins: one into the anterior process (distal fragment) and one into the anterior body of the calcaneus (proximal fragment).
- Apply a hinged cervical lamina spreader (smooth or with very small teeth) between the pins or directly into the osteotomy to gently open the lateral column.
5. Graft Insertion and Alignment Assessment
- Harvest or prepare the appropriately sized tricortical graft (typically 8 to 10 mm wide at its lateral base, tapering medially to fit the wedge defect).
- Insert the graft into the distracted osteotomy. The cortical margin of the graft should sit flush with the lateral wall of the calcaneus.
- Critical Step: Assess the foot for clinical and radiographic alignment before final fixation. Ensure the heel is in neutral to slight valgus and the forefoot abduction is corrected.
- Do not overcorrect. Overcorrection leads to a rigid, supinated forefoot and severe lateral column overload, which is poorly tolerated by the patient.
6. Fixation
- Fix the graft securely to prevent displacement or collapse.
- Options include:
- Smooth or threaded Steinmann pins (often buried beneath the skin).
- Bone staples.
- A cervical H-plate or dedicated lateral column locking plate.
- Note: The subcutaneous nature of hardware in this region frequently causes irritation, necessitating hardware removal at a later date. Discuss this possibility with the patient preoperatively.
7. Alternative: Calcaneocuboid Joint Distraction Arthrodesis
Sangeorzan et al. demonstrated success with lateral column lengthening performed directly through the calcaneocuboid joint (distraction arthrodesis).
* If this technique is chosen, carry the incision more distally.
* Denude the opposing cartilaginous surfaces of the calcaneus and cuboid down to bleeding cancellous bone.
* A larger graft is required; a 1.5-cm graft is routinely used in this situation.
* A cervical H-plate is generally utilized for distraction and rigid fixation.
* Author's Experience: It is significantly more difficult to obtain reliable bony union with this joint-spanning osteotomy compared to the extra-articular anterior calcaneal osteotomy.
8. Final Medial Tensioning and Closure
- Return to the medial side of the foot.
- With the lateral column now lengthened and the arch restored, tension and secure the FDL transfer into the navicular and finalize the spring ligament reconstruction.
- Close both wounds in layers. Apply a sterile dressing and a well-padded, short-leg plaster splint in neutral dorsiflexion.
RADIOGRAPHIC CASE EXAMPLES
The following radiographs demonstrate a severe, decompensated flatfoot deformity treated with a comprehensive reconstruction, including lateral column lengthening with an allograft, a medial displacement calcaneal osteotomy (MDCO), and a naviculocuneiform (NC) arthrodesis to address fixed forefoot supination.

Figure 4: Anteroposterior (AP) radiograph demonstrating lateral column lengthening with a structural allograft secured by an H-plate, alongside a medial displacement calcaneal osteotomy and naviculocuneiform arthrodesis.
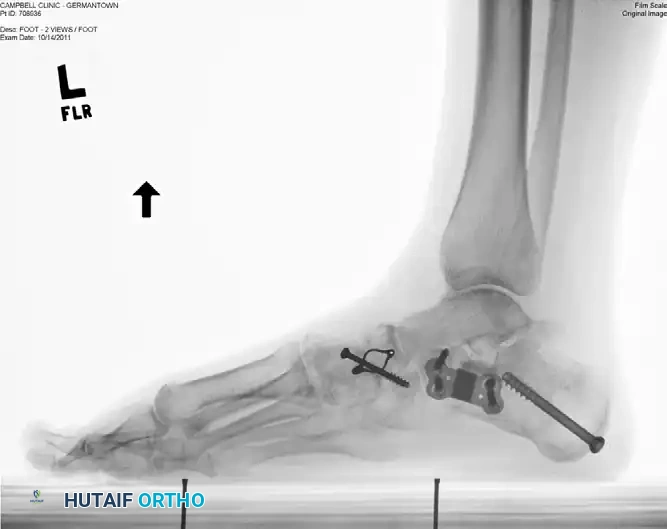
Figure 5: Lateral radiograph of the same patient, showing excellent restoration of the medial longitudinal arch, proper graft placement, and hardware integration.
COMPLICATIONS AND MANAGEMENT
While highly effective, the anterior calcaneal osteotomy carries a distinct complication profile that must be discussed with the patient during the informed consent process:
- Graft Collapse and Nonunion: More common in heavier patients (>180 lbs) or when using non-structural allografts. Nonunion rates can approach 10-15%. Management requires revision grafting and rigid plate fixation.
- Lateral Column Pain and Overload: Often a result of over-lengthening the lateral column (using a graft >10mm). This leads to increased pressures in the CC joint and fifth metatarsal base.
- Calcaneocuboid Joint Arthritis: The increased pressure across the CC joint can lead to radiographic and clinical arthritis over time. If symptomatic, this may eventually require a CC joint arthrodesis.
- Sural Neuritis: The sural nerve is highly vulnerable during the lateral approach. Meticulous soft tissue handling is required. Neuromas may require excision and burying of the nerve stump.
- Painful Hardware: Due to the thin soft tissue envelope over the lateral calcaneus, plates and staples frequently become prominent and painful, necessitating a secondary procedure for hardware removal once union is achieved.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
Postoperative management must be strictly adhered to, as premature weight-bearing is the leading cause of graft collapse and failure.
Phase 1: Immediate Postoperative (Weeks 0-2)
* The patient is placed in a well-padded short-leg splint in the operating room.
* Hospital admission for 2 to 3 days is typical for intravenous pain control and elevation.
* Strict non-weight-bearing (NWB) status is enforced.
* At 2 weeks, the splint is removed, wounds are inspected, and sutures are removed.
Phase 2: Protection and Bone Healing (Weeks 2-12)
* The patient is transitioned into a fiberglass non-weight-bearing cast.
* Cast changes are routinely performed at 6 weeks and 12 weeks postoperatively.
* Continued strict NWB is recommended for a total of 8 to 12 weeks.
* Imaging: At the 10 to 12-week mark, anteroposterior and lateral radiographs are obtained. If plain films are equivocal, a CT scan at 12 weeks is highly recommended to definitively confirm bony incorporation of the graft.
Phase 3: Transition to Weight-Bearing (Months 3-4)
* Once radiographic evidence of bony union is confirmed, the patient is transitioned to a weight-bearing cast or a prefabricated removable walking boot (typically around 3 to 3.5 months postoperatively).
* Progressive weight-bearing is initiated.
* Formal physical therapy begins, focusing on gentle stretching, restoration of ankle and subtalar range of motion, and appropriate calf strengthening.
* Patients are advised that maximal medical improvement and complete resolution of swelling may take up to 12 to 18 months.
You Might Also Like