Operative Management of Clavicle Fractures: A Surgical Guide
Key Takeaway
Clavicle fractures are common injuries traditionally treated nonoperatively. However, specific indications such as open fractures, neurovascular compromise, symptomatic nonunion, severe displacement (>2 cm shortening), and unstable lateral fractures (Neer Type II) necessitate surgical intervention. Operative management, utilizing either plate osteosynthesis or intramedullary fixation, restores anatomical length and alignment, significantly reducing nonunion rates and optimizing functional outcomes in the upper extremity.
Principles of Upper Extremity Trauma
Trauma to the upper extremity presents a uniquely difficult challenge for orthopaedic surgeons. Whether the encountered pathology is a simple fracture, a complex fracture-dislocation, or a severe crush injury involving vital soft tissues and neurovascular elements, the ultimate functional result depends as much on the viability of the surrounding soft-tissue envelope as it does on the osseous reconstruction.
In the lower extremity, a fracture may heal with mild contracture, slight loss of adjacent joint motion, or soft-tissue compromise, yet still yield a highly functional, weight-bearing result. Conversely, the upper extremity relies on intricate spatial positioning and fine motor dexterity. Severe functional impairment inevitably results if fracture healing is accompanied by soft-tissue contractures or joint stiffness, even if the bone itself has achieved radiographic union. Therefore, the surgical management of fractures and fracture-dislocations in the upper extremity and shoulder girdle demands meticulous handling of soft tissues, rigid internal fixation to allow early mobilization, and a profound understanding of regional biomechanics.
Clavicle Fractures: Epidemiology and Biomechanics
The clavicle is an S-shaped strut that connects the upper extremity to the axial skeleton. Fractures of the clavicle are among the most common bony injuries encountered in orthopaedic traumatology. Historically, it was widely taught that the most common mechanism of injury was a fall on an outstretched hand (FOOSH). However, modern biomechanical and epidemiological analyses have refuted this. In a landmark study of 122 patients with clavicular fractures, Stanley et al. demonstrated that in 94% of cases, the mechanism of injury was a direct blow to the lateral aspect of the shoulder.
Nonoperative Treatment and the Historical Perspective
The vast majority of clavicle fractures can be managed nonoperatively with a simple sling or figure-of-eight harness. The literature has historically supported high union rates with conservative care. In a massive review of 2,235 clavicular fractures treated closed, Neer reported a nonunion rate of only 0.1% (three cases). In contrast, his series of 45 fractures treated by open reduction yielded a nonunion rate of 4% (two cases). Similarly, Rowe reported nonunion in 0.8% of fractures treated by closed methods compared to 3.7% treated by open reduction.
More recent prospective data, however, suggest that the nonunion rate for displaced midshaft fractures treated nonoperatively may be higher than historically quoted. Nowak et al. reported a nonunion rate of 7% in a prospective study of 208 patients treated without surgery.
Clinical Pearl: Cosmesis is rarely an acceptable primary indication for surgery. Even if the fracture ends heal in an overlapped or bayonet apposition with a substantial bony prominence, this mass largely resorbs and remodels over time. The orthopaedic surgeon must not be tempted to perform an open reduction merely because the patient or family objects to a palpable bump. In many cases, the surgical scar over the anterior chest can be more unsightly and prone to keloid formation than the bony prominence itself.
Indications for Operative Intervention
While nonoperative management remains the gold standard for undisplaced or minimally displaced fractures, specific clinical scenarios mandate open reduction and internal fixation (ORIF).
1. Symptomatic Nonunion
Nonunion is the most frequent indication for delayed open reduction. A clavicle fracture that fails to show radiographic progression of healing by 6 months, accompanied by pain and motion at the fracture site, requires surgical intervention. Treatment necessitates rigid internal fixation with a plate and screws or an intramedullary device, invariably augmented with autologous cancellous bone grafting.
2. Neurovascular Compromise
The clavicle sits directly superior to the subclavian vessels and the brachial plexus. Neurovascular compromise that is not immediately resolved by closed reduction of the fracture requires emergent open exploration. If an open reduction is performed to decompress the neurovascular structures, the fracture must be internally stabilized to prevent secondary injury.
3. Displaced Lateral Clavicle Fractures (Neer Classification)
Fractures of the lateral end of the clavicle near the acromioclavicular (AC) joint present unique biomechanical challenges. Neer identified five distinct types of lateral clavicular fractures based on their relationship to the coracoclavicular (CC) ligaments:
- Type I: Minimally displaced, occurring lateral to the intact coracoacromial and coracoclavicular ligaments. Stable.
- Type III: Intra-articular fractures extending into the AC joint. Stable, though prone to late AC arthrosis.
- Type IV: Pediatric fractures involving a distal periosteal sleeve disruption. The medial fragment strips from the periosteum and rides superiorly. Open reduction is unnecessary as the periosteal sleeve rapidly fills with new bone, and massive remodeling occurs.
- Type II: Highly unstable fractures. The CC ligaments are detached from the medial fragment.
- Type IIA: The conoid and trapezoid ligaments remain attached to the distal fragment.
- Type IIB: The conoid ligament is torn, but the trapezoid remains attached to the distal fragment.
- Type V: Comminuted avulsion fractures leaving only an inferior cortical fragment attached to the CC ligaments. Highly unstable.
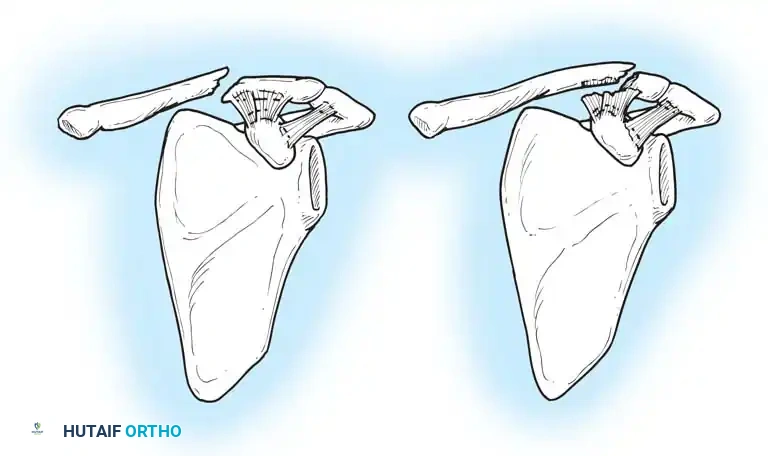
Fig. 54-1: Neer type II clavicular fractures. (IIA) Unstable lateral clavicular fracture. Coracoacromial ligaments and AC joint capsule are intact. (IIB) Unstable lateral fracture with disruption of the coracoacromial ligament.
Management of Type II and Type V Fractures:
The distal end of the medial fragment is pulled superiorly and posteriorly by the trapezius, while the small lateral fragment (often only 2.5 cm long) is held inferiorly by the weight of the arm and the intact AC joint. Closed reduction is notoriously difficult to maintain.
Robinson and Cairns reported that 14% of patients with displaced lateral fractures treated nonoperatively required delayed surgery for painful nonunion, with an overall nonunion rate of 21%. Anderson reported a 30% nonunion rate. Consequently, operative fixation is widely recommended for displaced Type II and Type V fractures.
Surgical options include:
1. Plate and screw fixation (often requiring specialized locking plates or hook plates).
2. Transacromial Kirschner wires with tension band wiring.
3. Coracoclavicular ligament reconstruction using Mersilene tape, Dacron, or PDS bands.
4. A single transacromial Knowles pin.
Surgical Warning: The use of smooth Kirschner wires in the clavicle carries a severe risk of catastrophic medial migration into the mediastinum, potentially injuring the heart or great vessels. Flinkkilä et al. reported K-wire migration in 54% of patients. If wires are used, their lateral ends must be bent 90 degrees to physically prevent medial translation.
4. Severe Displacement and Soft-Tissue Interposition
If the deltoid or trapezius muscle is impaled by a sharp cortical spike, closed reduction is impossible. These spikes may tent the skin, threatening necrosis. If closed reduction fails, ORIF is justified. Hill et al. demonstrated a 15% nonunion rate in midshaft fractures with initial shortening greater than 2 cm. Restoration of anatomical length is crucial to restore the resting tension of the shoulder girdle musculature.
5. The Floating Shoulder
A "floating shoulder" occurs when there are ipsilateral fractures of the clavicle and the surgical neck of the scapula, disrupting the Superior Shoulder Suspensory Complex (SSSC).
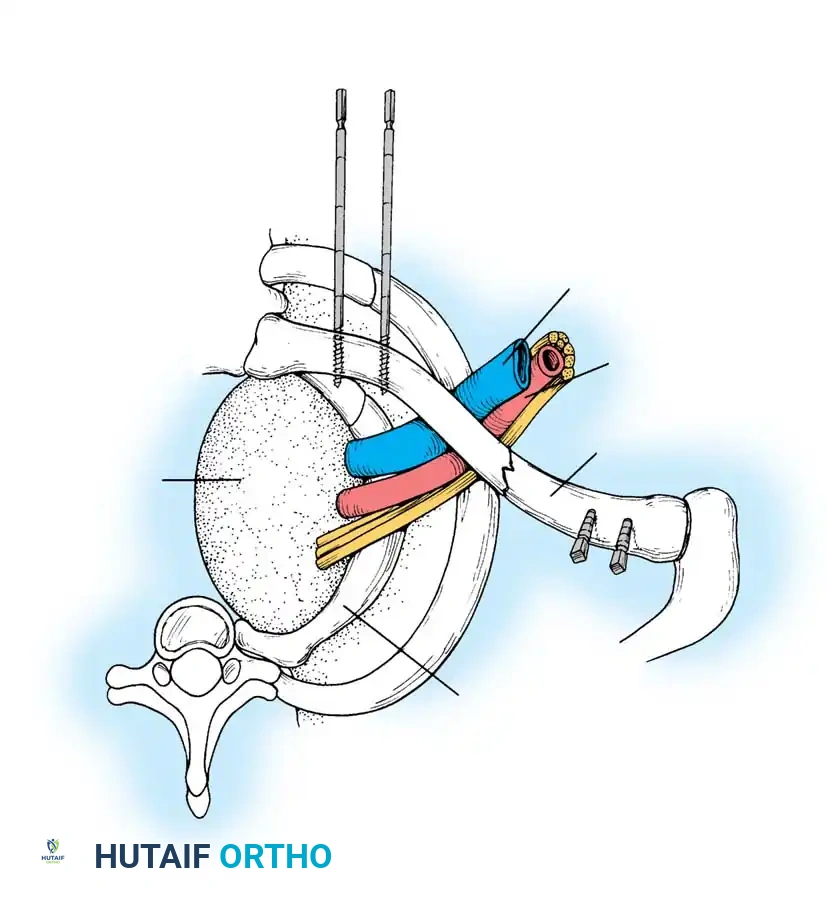
Fig. 54-2: Biomechanics of the floating shoulder. The weight of the arm and the pull of the shoulder girdle muscles rotate the glenoid fragment anteromedially, leading to severe drooping of the shoulder.
This double disruption renders the scapular fracture highly unstable. Herscovici et al. recommended ORIF of the clavicular fracture with a 3.5-mm plate to indirectly stabilize the scapular neck, preventing malunion and shoulder ptosis.

Fig. 54-3A: Preoperative radiograph demonstrating a severely displaced floating shoulder variant.
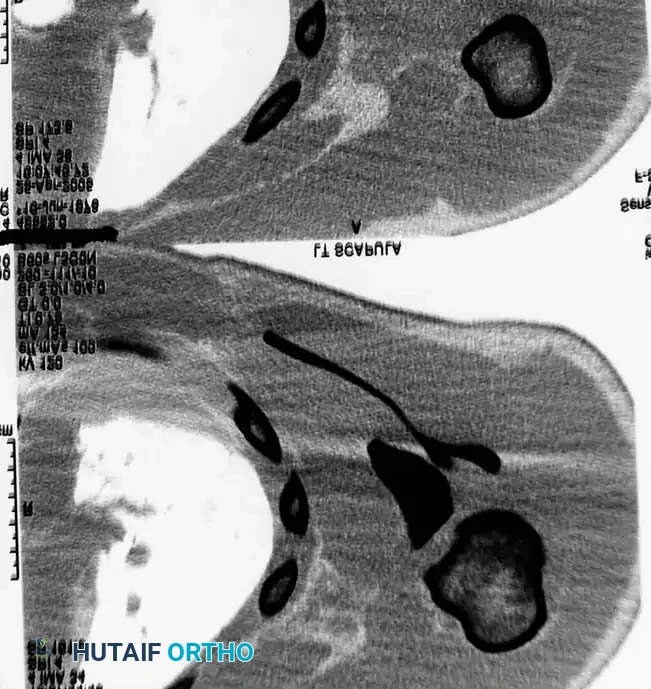
Fig. 54-3B: Axial CT scan detailing the severe displacement of the scapular body and neck.

Fig. 54-3C: Additional axial CT slice confirming intra-articular extension and comminution.
However, Edwards et al. reviewed 20 patients with floating shoulders and achieved union with nonoperative treatment in 19 cases, noting excellent functional results if displacement was less than 5 mm. Therefore, widely displaced fractures (>5 mm to 1 cm of translation or severe angulation) require operative fixation of the clavicle, and occasionally the scapula as well.
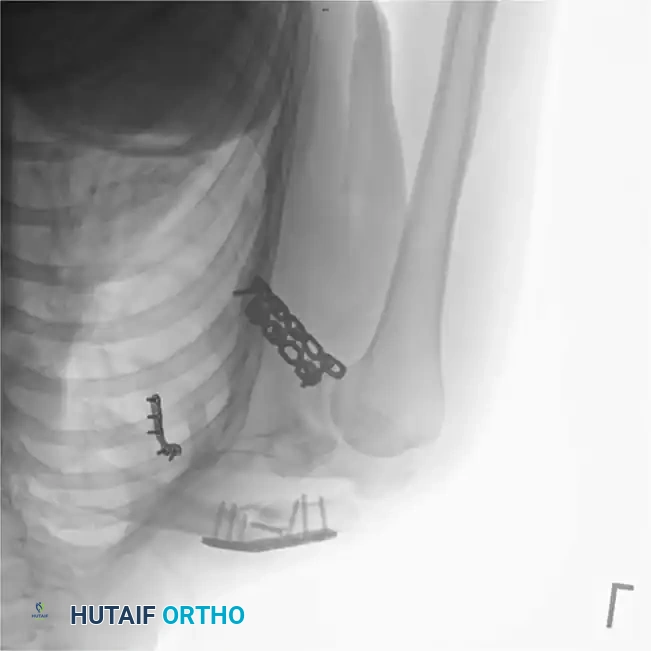
Fig. 54-3D: Postoperative radiograph showing restoration of the SSSC via plate osteosynthesis of both the clavicle and the lateral border of the scapula.
Special Consideration: The Throwing Athlete
There is a modern trend advocating for aggressive ORIF in throwing athletes to maintain absolute clavicular length. However, evidence-based practice dictates caution. Fractures that unite in a slightly shortened or angulated position rarely have a measurable negative influence on throwing mechanics or velocity. Indications for surgery in athletes should remain grounded in the standard criteria (displacement >2 cm, tenting, nonunion) rather than theoretical kinematic concerns.
Surgical Techniques
Intramedullary Fixation (Modified McKeever Technique)
Intramedullary (IM) fixation offers the advantage of a smaller incision, less periosteal stripping, and a cosmetically superior scar. However, the IM pin must be strongly tempered to withstand the unsupported weight of the upper extremity without bending. Rockwood developed a specialized IM clavicular nail with a lateral compression nut that allows dynamic compression across the fracture site.
Operative Steps:
1. Incision: Make a 2.5 cm incision directly over the fracture site (extend as necessary for comminution). Carry dissection down to the bone, strictly avoiding circumferential periosteal stripping to preserve the blood supply.
2. Medial Preparation: Pass a smooth 3.2-mm Steinmann pin into the medullary canal of the medial fragment for a distance of 3.8 to 7.5 cm to establish the pathway. Remove the pin.
3. Lateral Preparation: Pass the pin laterally into the medullary canal of the lateral fragment until it emerges through the posterior cortex near the conoid tubercle.
4. Skin Exit: Retract the skin slightly, make a small stab incision over the exiting pin, and drive the pin out posteriorly. Remove this smooth pin.
5. Threaded Pin Insertion: Select a 3.2-mm threaded Steinmann pin (pointed at both ends). Drill it retrograde through the lateral fragment from the posterior stab wound.
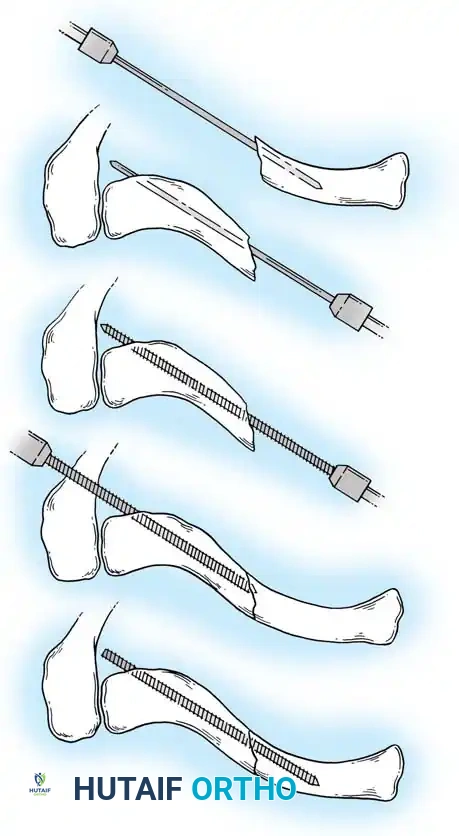
Fig. 54-4: Step-by-step illustration of the modified McKeever intramedullary pinning technique.
- Reduction and Advancement: When the blunt end of the pin is flush with the fracture site, anatomically reduce the fracture. Drill the pin antegrade into the prepared medial canal. Crucial: Do not distract the fracture site during subsequent arm motion, as this drastically increases the risk of pin breakage.
- Finalization: Verify position with fluoroscopy. Cut the redundant posterior end of the pin beneath the skin. If a smooth pin is used instead of a threaded one, the lateral end must be bent 90 degrees to prevent fatal medial migration.
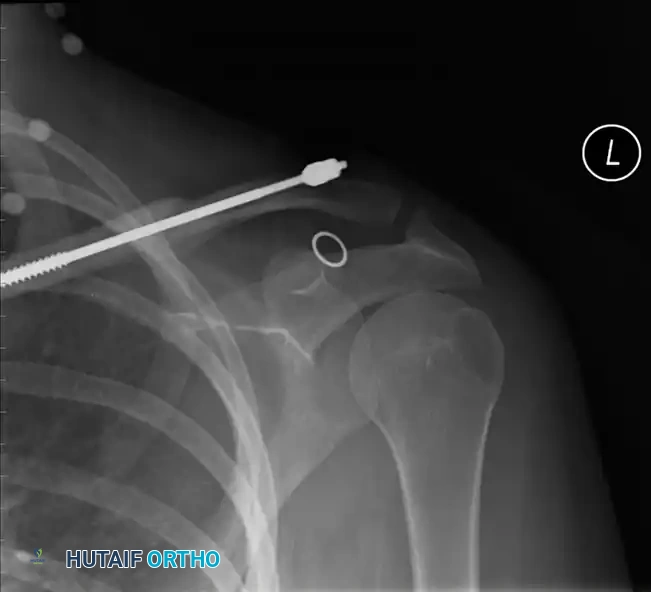
Fig. 54-5: Postoperative radiograph demonstrating successful intramedullary fixation of a midshaft clavicle fracture using a threaded device with a lateral compression nut.
Plate Osteosynthesis
Plate fixation is the workhorse for displaced midshaft and lateral clavicle fractures. It provides rigid biomechanical stability, controls rotation, and allows for immediate postoperative mobilization.
Biomechanical Considerations:
The plate must be meticulously contoured to follow the complex S-shape of the clavicle. Superior plating acts as a tension band against the inferiorly directed deforming forces of the arm's weight. Anteroinferior plating is an alternative that utilizes longer screws (anterior to posterior) and reduces hardware prominence under the skin, though it may be biomechanically slightly weaker in cantilever bending.
Operative Steps:
1. Positioning: The patient is placed in the beach-chair position with a bump between the scapulae to allow the shoulder to fall posteriorly, aiding in reduction.
2. Approach: An incision is made centered over the clavicle. The supraclavicular nerves should be identified and protected to prevent painful postoperative neuromas and anterior chest wall numbness.
3. Reduction: The fracture is exposed, and the hematoma is evacuated. If an oblique fracture pattern is present, an independent lag screw should be placed to achieve absolute stability and interfragmentary compression.
4. Plating: An AO 3.5-mm pelvic reconstruction plate, locking compression plate (LCP), or pre-contoured anatomical clavicle plate is applied.

Fig. 54-6: Intraoperative photograph demonstrating superior application of a contoured 3.5-mm reconstruction plate. Note the meticulous preservation of soft tissue attachments to the comminuted butterfly fragments.
- Fixation: A minimum of three bicortical screws (six cortices) must be obtained in both the medial and lateral main fragments to ensure adequate pull-out strength. In osteoporotic bone, locking screws are highly recommended.
- Bone Grafting: If there is severe comminution or a segmental defect, autologous cancellous bone graft (often harvested from the proximal humerus or iliac crest) should be packed into the defect.
Postoperative Care and Rehabilitation
Following rigid internal fixation, the arm is supported in a sling for comfort for 1 to 2 weeks.
* Phase I (0-2 weeks): Immediate pendulum exercises and passive range of motion (ROM) of the elbow, wrist, and hand are initiated.
* Phase II (2-6 weeks): Active-assisted ROM of the shoulder is permitted up to 90 degrees of forward flexion and abduction. Overhead elevation and heavy lifting are strictly prohibited.
* Phase III (6-10 weeks): Once radiographic evidence of bridging callus is observed (typically 8 to 10 weeks), full active ROM and progressive strengthening are initiated.
Hardware Removal:
Routine removal of clavicular plates is not recommended due to the risk of refracture through empty screw holes. However, if the hardware becomes highly symptomatic or prominent beneath the skin (especially in thin individuals
📚 Medical References
- clavicle fractures in children: a review of 21 years, J Pediatr Orthop 22:736, 2002.
- Larsen CL, Kiaer T, Lindequist S: Fractures of the proximal humerus in children: nine-year follow-up of 64 unoperated cases, Acta Orthop Scand 61:255, 1990.
- Lloyd-Roberts GC, Apley AG, Owen R: Refl ections upon the aetiology of congenital pseudarthrosis of the clavicle, J Bone Joint Surg 57B:24, 1975.
- Neer CS II: Fractures of the distal third of the clavicle, Clin Orthop Relat Res 58:43, 1968.
- Neer CS, Horowitz BS: Fractures of the proximal humeral epiphyseal plate, Clin Orthop Relat Res 41:24, 1965.
- Rockwood CA: Dislocations of the sternoclavicular joint, Instr Course Lect 24:144, 1975.
- Rockwood CA: Fractures of the outer clavicle in children and adults, J Bone Joint Surg 64B:642, 1982.
- Rockwood CA Jr: Fractures and dislocations of the shoulder: III. Fractures and dislocations of the ends of the clavicle, scapula, and glenohumeral joint. In Rockwood CA Jr, Wilkins KE, King RE, eds: Fractures in children, Philadelphia, 1984, Lippincott. Rowe CR, Pierce DS, Clark JG: Voluntary dislocation of the shoulder, J Bone Joint Surg 55A:445, 1973.
- Sherk HH, Probst C: Fractures of the proximal humeral epiphysis, Orthop Clin North Am 6:401, 1975.
- Siambanes D, Martinez JW, Butler EW, et al: Infl uence of school backpacks on adolescent back pain, J Pediatr Orthop 24:211, 2004.
- Torode I, Donnan L: Posterior dislocation of the humeral head in association with obstetric paralysis, J Pediatr Orthop 18:611, 1998.
- Waters PM, Bae DS, Kadiyala RK: Short-term outcomes after surgical treatment of traumatic posterior sternoclavicular fracture-dislocations in children and adolescents, J Pediatr Orthop 23:464, 2003.
- Wilkes JA, Hoffer MM: Clavicle fractures in head-injured children, J Orthop Trauma 1:55, 1987.
- Zenni EJ, Krieg JK, Rosen MJ: Open reduction and internal fi xation of clavicular fractures, J Bone Joint Surg 63A:147, 1981.
- Spine Fractures and Dislocations Anderson LD, D’Alonzo RT: Fractures of the odontoid process of the axis, J Bone Joint Surg 56A:1663, 1974.
- Bailey DK: The normal cervical spine in infants and children, Radiology 59:712, 1952.
- Carrion WV, Dormans JP, Drummond DS, et al: Circumferential growth plate fracture of the thoracolumbar spine from child abuse, J Pediatr Orthop 16:210, 1996.
- Cattell HS, Filtzer DL: Pseudosubluxation and other normal variations in the cervical spine in children, J Bone Joint Surg 47A:1295, 1965.
- Clark JE: Apophyseal fracture of the lumbar spine in adolescence, Orthop Rev 20:512, 1991.
- Crawford AH: Operative treatment of spine fractures in children, Orthop Clin North Am 21:325, 1990.
- Crockard HA, Rogers MA: Open reduction of traumatic atlantoaxial rotatory dislocation with use of the extreme lateral approach, J Bone Joint Surg 78A:431, 1996.
- Edmonson AS: The spine. In Edmonson AS, Crenshaw AH, eds: Campbell’s
You Might Also Like

