Osteochondritis Dissecans: Comprehensive Surgical Management
Key Takeaway
Osteochondritis dissecans (OCD) is a focal idiopathic alteration of subchondral bone with risk for instability and disruption of adjacent articular cartilage. Most commonly affecting the medial femoral condyle, OCD presents distinct clinical challenges depending on physeal maturity. This guide provides an evidence-based approach to the diagnosis, imaging, and surgical management of OCD, including arthroscopic drilling, internal fixation, and osteochondral grafting techniques for both juvenile and adult populations.
Introduction to Osteochondritis Dissecans
Osteochondritis dissecans (OCD) is a focal, idiopathic condition characterized by the necrosis of subchondral bone, which subsequently induces secondary degenerative changes in the overlying articular cartilage. If left untreated, the necrotic bone and its cartilaginous cap may progressively separate from the surrounding healthy osteochondral bed, ultimately resulting in a loose body within the joint. Indeed, OCD remains the most common source of intra-articular loose bodies in the knee joint, followed by synovial chondromatosis, osteophytes, fractured articular surfaces, and damaged menisci.
The condition predominantly affects the knee, though it is also documented in the elbow (capitellum), ankle (talus), shoulder, and hip. Within the knee, the anatomic distribution is highly specific. The classic presentation involves the lateral aspect of the medial femoral condyle, near the attachment of the posterior cruciate ligament.
While medial femoral condylar lesions are the most prevalent, lateral femoral condylar lesions account for approximately 15% of cases, and patellar lesions (typically in the inferomedial quadrant) account for less than 5%.
OCD exhibits a strong male predilection, occurring twice as often in males as in females, and typically presents during adolescence. Clinically and prognostically, patients are stratified into two distinct cohorts:
1. Juvenile Osteochondritis Dissecans (JOCD): Occurs in young patients prior to physeal closure. This cohort generally responds well to nonoperative management, with a high potential for spontaneous healing.
2. Adult Osteochondritis Dissecans (AOCD): Occurs in skeletally mature patients. The etiology is often linked to vascular phenomena, and the prognosis is markedly less satisfactory, frequently necessitating surgical intervention.
Etiology and Pathogenesis
The precise etiology of osteochondritis dissecans remains a subject of academic debate. The pathogenesis is likely multifactorial, with several proposed theories:
- Repetitive Microtrauma: The most widely accepted theory suggests that repetitive mechanical stress leads to subchondral microfractures. Subsequent interruption of the interosseous blood supply to the subchondral epiphysis results in localized ischemia and necrosis.
- Ischemia: Primary vascular insufficiency to the subchondral bone, potentially exacerbated by anatomic variations in the knee's vascular supply.
- Genetic and Familial Predisposition: A familial tendency has been observed in multiple cohorts, suggesting a genetic component affecting subchondral ossification.
- Endocrine and Growth Disorders: Epiphyseal abnormalities, accessory centers of ossification, and endocrine imbalances have been implicated.
Clinical Pearl: The stark contrast in clinical behavior between JOCD and AOCD has led some authorities to postulate that JOCD may represent a variant of normal physeal growth rather than a true pathological entity. The high frequency of bilaterally symmetrical lesions that heal spontaneously in juveniles strongly supports the theory of an ossification anomaly rather than true osteonecrosis.
Clinical Evaluation
Patient History
OCD is rare in patients younger than 10 or older than 50 years. The hallmark symptom is a vague, poorly localized, aching discomfort in the knee that is exacerbated by activity. In the juvenile population, symptoms are often insidious; approximately 80% of juvenile patients experience symptoms for an average of 14 months prior to initial orthopedic evaluation. A distinct history of trauma is reported in 40% to 60% of cases.
As the lesion progresses to partial or complete separation, mechanical symptoms such as catching, locking, and popping become prominent. These mechanical symptoms can closely mimic meniscal pathology. Once complete detachment occurs, the patient may report palpable loose bodies migrating within the joint capsule.
Physical Examination
A meticulous physical examination is required to differentiate OCD from other intra-articular pathologies. Key findings may include:
* Effusion: Typically mild; a massive effusion is rare unless a large fragment has acutely detached.
* Tenderness: Focal joint line tenderness or direct tenderness over the affected condyle (most commonly the medial femoral condyle).
* Range of Motion: Terminal extension may be limited due to pain or mechanical block.
* Muscle Atrophy: Chronic cases frequently present with measurable quadriceps atrophy.
* Wilson Sign: A classic, though not universally present, clinical sign. The patient walks with an externally rotated gait to prevent the medial tibial spine from impinging on the classic OCD lesion of the medial femoral condyle. Elicited on the exam table by internally rotating the tibia during knee extension; pain at approximately 30 degrees of flexion that is relieved by external rotation is considered a positive Wilson sign.
Diagnostic Imaging
Radiography
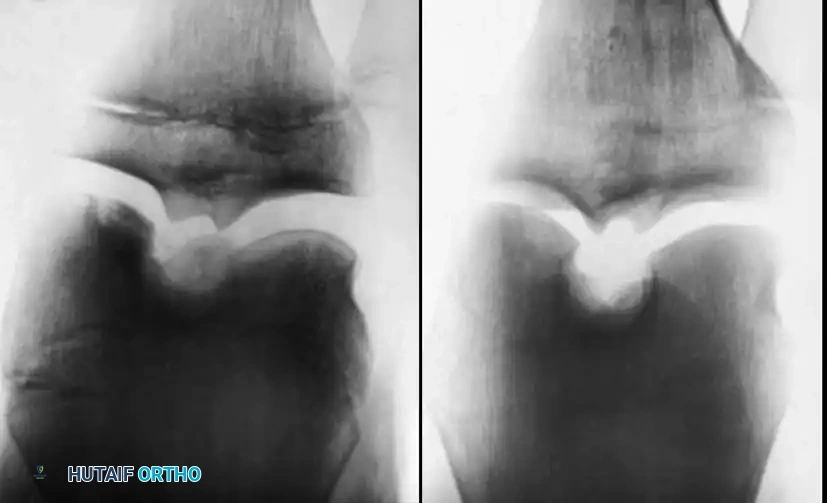
Standard radiographic evaluation is the first-line diagnostic modality. A complete knee series must include weight-bearing anteroposterior (AP), lateral, skyline (patellar), and tunnel (intercondylar notch) views.
Surgical Warning: Because the most common location for an OCD lesion is the posterolateral aspect of the medial femoral condyle, standard AP views may obscure the defect. The tunnel view (flexed knee posteroanterior radiograph) is absolutely critical for visualizing these lesions.
Comparison radiographs of the contralateral knee are highly recommended in juvenile and adolescent patients. OCD is bilateral in approximately 30% of patients, and comparison views help differentiate true OCD from bilateral anomalous ossification centers, which typically resolve spontaneously within 6 to 12 months.
Scintigraphy (Bone Scan)
Technetium-99m bone scintigraphy has historically been utilized to assess the healing activity of lesions and predict treatment outcomes. Cahill and Berg developed a widely recognized scintigraphic classification system (Table 1) that helps distinguish between scan-negative ossific anomalies and scan-positive unhealed OCD lesions. Sequential SPECT scans at 8-week intervals can monitor healing progression.
Table 1: Cahill and Berg Scintigraphic Classification of OCD
* Stage 0: Normal radiographic and scintigraphic appearance.
* Stage I: Lesion visible on plain radiographs; bone scan normal.
* Stage II: Increased uptake focal to the area of the lesion.
* Stage III: Increased isotopic uptake throughout the entire femoral condyle.
* Stage IV: Increased uptake in the tibial plateau opposite the lesion (kissing lesion).
Magnetic Resonance Imaging (MRI)
MRI is the gold standard for evaluating fragment stability, viability, and the integrity of the overlying articular cartilage. A spoiled gradient-echo sequence utilizing fat suppression and three-dimensional acquisition is currently considered the optimal technique for evaluating articular cartilage.
MRI Signs of Instability:
1. A high-signal intensity line (fluid) interposing between the fragment and the crater on T2-weighted or STIR images.
2. Focal cystic areas beneath the fragment.
3. A high-signal intensity line breaching the articular cartilage.
Conversely, the absence of a high-signal zone at the fragment-bone interface is a highly reliable indicator of lesion stability. Dipaola et al. established a comprehensive staging system correlating MRI findings with arthroscopic and radiographic appearances.
Table 2: Dipaola Staging System for Osteochondritis Dissecans
* Stage I: Thickening of articular cartilage; low signal changes. (Arthroscopy: Irregularity/softening; no definable fragment).
* Stage II: Articular cartilage breached; low signal rim behind fragment indicating fibrous attachment. (Arthroscopy: Definable fragment, not displaceable).
* Stage III: Articular cartilage breached; high signal changes behind fragment indicating synovial fluid. (Arthroscopy: Definable fragment, displaceable but attached).
* Stage IV: Loose body present. Displaced fragment. (Arthroscopy: Empty crater and loose body).
Nonoperative Management
The primary goal of treatment is to promote healing of the subchondral bone before physeal closure while preventing fragment detachment. Nonoperative management is the standard of care for stable JOCD lesions in skeletally immature patients.

Protocols and Outcomes
Conservative treatment modalities include activity modification, protected weight-bearing (crutches), and occasionally, brief periods of immobilization (cylinder cast or brace).
Pitfall: Prolonged rigid immobilization must be strictly avoided. The absence of joint motion accelerates articular cartilage attrition and joint stiffness. Controlled, protected motion is preferred.
While nonoperative treatment is highly successful in young patients with open physes, Cahill et al. noted a 50% failure rate in certain juvenile populations. In older adolescents and adults (AOCD), conservative management has a limited role, as the prognosis for spontaneous healing is exceedingly poor regardless of the nonoperative protocol employed.
Operative Management
Surgical intervention is indicated for:
1. Skeletally mature patients (AOCD).
2. JOCD lesions that fail 6 to 9 months of conservative management.
3. Lesions exhibiting clinical or MRI signs of instability (fluid behind the fragment).
4. Detached loose bodies.
5. Lesions larger than 1 cm in diameter involving the primary weight-bearing surface.
Arthroscopic Evaluation and Drilling
Arthroscopy offers the advantage of direct visualization of surface topography, dynamic probing for stability, and minimal morbidity. For stable lesions with intact articular cartilage that have failed conservative care, drilling is the procedure of choice. Drilling breaches the sclerotic margin of the crater, creating vascular channels that stimulate angiogenesis and subsequent bone healing.
- Transarticular Drilling: Performed directly through the articular cartilage into the subchondral bone using a 0.062-inch Kirschner wire. Multiple perforations are made.
- Retroarticular Drilling: Utilized to preserve the intact articular cartilage. Under fluoroscopic guidance, a drill guide is used to approach the lesion from the extra-articular metaphysis, drilling into the subchondral bed without violating the chondral surface.
Arthroscopic Fixation and Bone Grafting
For lesions demonstrating early separation (Stage II or III), stabilization is required. Because partial detachment allows synovial fluid to enter the interface and promotes fibrous tissue interposition, simple pinning is insufficient.
Surgical Steps for Fixation:
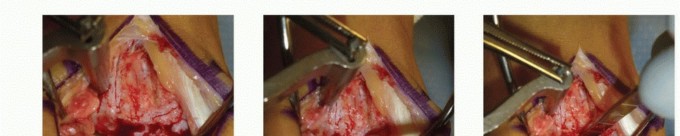
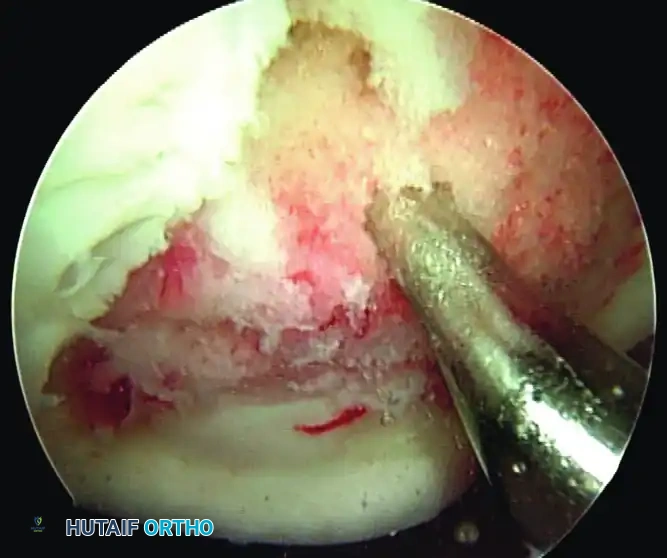
1. Debridement: The fragment is hinged open (like a trapdoor) using a probe. All fibrous tissue at the base of the crater and the undersurface of the fragment must be meticulously curetted down to bleeding, healthy cancellous bone.
2. Bone Grafting: If a volumetric defect exists, cancellous autograft (often harvested from the proximal tibia or distal femur) is packed into the crater to restore joint congruity.
3. Fixation: The fragment is reduced and compressed. Fixation can be achieved using multiple modalities:
* Bioabsorbable pins/darts: Eliminate the need for hardware removal but may cause sterile synovitis or osteolysis.
* Metallic Fixation: Herbert screws or threaded Kirschner wires provide excellent compression.

Clinical Pearl: When using metallic Kirschner wires or screws, they must be countersunk below the articular surface to prevent kissing lesions on the opposing tibial plateau. Guhl advocated for the removal of metallic fixation pins once laminographic or radiographic evidence of early union is observed (typically 8 to 12 weeks postoperatively).
Open Arthrotomy
While arthroscopic techniques are preferred, open arthrotomy remains highly relevant and is indicated when:
* The surgeon's arthroscopic proficiency is insufficient for complex grafting.
* The lesion is located in an area inaccessible to arthroscopic instrumentation (e.g., extreme posterior condyle, certain lateral condyle or patellar lesions).
* The lesion is massive (>3 cm) requiring multiple structural grafts.
* A large loose body requires reshaping and complex internal fixation.
Surgical Tip: During arthrotomy, the intra-articular injection of methylene blue can help delineate the margins of the cartilaginous defect. The knee must be fully flexed to expose posterior lesions adequately.
Salvage and Cartilage Restoration Techniques
In cases where the osteochondral fragment is fragmented, necrotic, or unsalvageable, the loose bodies must be excised, and the crater managed to prevent early-onset osteoarthritis.
* Microfracture: Suitable for small defects (<2 cm²).
* Osteochondral Autograft Transfer System (OATS): Cylindrical osteochondral plugs are harvested from non-weight-bearing areas (e.g., the intercondylar notch or periphery of the trochlea) and press-fit into the debrided crater.
* Osteochondral Allograft Transplantation: Indicated for large defects (>3 cm²) where autograft harvest would cause unacceptable donor-site morbidity.
* Autologous Chondrocyte Implantation (ACI): A two-stage procedure involving the harvest and expansion of chondrocytes, followed by implantation under a periosteal patch or collagen membrane.
Postoperative Rehabilitation
Postoperative protocols are dictated by the specific surgical intervention performed:
* Following Drilling/Fixation: Patients are typically restricted to non-weight-bearing or toe-touch weight-bearing for 6 to 8 weeks to protect the healing subchondral bed. Continuous Passive Motion (CPM) is initiated immediately to nourish the articular cartilage and prevent arthrofibrosis.
* Following Excision/Microfracture: Weight-bearing is restricted, but aggressive early range of motion is encouraged to stimulate fibrocartilage formation.
* Return to Play: Return to high-impact sports is delayed until complete radiographic union is confirmed, full pain-free range of motion is restored, and quadriceps strength is at least 90% of the contralateral limb. This process frequently requires 6 to 9 months of dedicated rehabilitation.
Osteochondritis dissecans remains a complex pathology requiring a nuanced understanding of joint biomechanics, patient biology, and advanced surgical techniques. Careful patient selection, precise imaging interpretation, and meticulous surgical execution are paramount to achieving joint preservation and optimal long-term outcomes.
📚 Medical References
- osteochondritis dissecans, J Bone Joint Surg 79A:471, 1997.
- Duri ZA, Aichroth PM, Wilkins R, et al: Patellar tendonitis and anterior knee pain, Am J Knee Surg 12:99:1999.
- Ferciot C: Surgical management of anterior tibial epiphysis, Clin Orthop 5:204, 1955.
- Ferguson AB, Howorth MB: Coxa plana and related conditions at the hip, J Bone Joint Surg 16:781, 1934.
- Hefti F, Buguiristain J, Krauspe R, et al: Osteochondritis dissecans: a multicenter study of the European Pediatric Orthopaedic Society, J Pediatr Orthop 8B:231, 1999.
- Hoerr NL, Pyle SI, Francis CC: Radiographic atlas of skeletal development of the foot and ankle, Springfi eld, Ill, 1962, Charles C Thomas. Iselin H: Wachstumsbeschwerden zur Zeit der Knochernen Entwicklung der Tuberosital metatarsi quint, Deutsch Zeit Chir 117:529, 1912.
- Lehman RC, Gregg JR, Torg E: Iselin’s disease, Am J Sports Med 14:494, 1986.
- Lloyd-Roberts GC, Wetherhill MH, Fraser M: Trochanteric advancement for premature arrest of the capital femoral epiphysis, J Bone Joint Surg 67B:20, 1985.
- MacEwen GD, Ramsey PL: The hip. In Lovell WW, Winter RB, eds: Pediatric orthopedics, Philadelphia, 1978, Lippincott. Miura H, Nagamine R, Urabe K, et al: Complications associated with Poly-L-lactic acid pins used for treating osteochondritis dissecans of the knee, Arthroscopy 15:1, 1999.
- Nowinski RJ, Mehlman CT: Hyphenated history: OsgoodSchlatter disease, Am J Orthop 27:584, 1998.
- Ogden JA: Skeletal injury in the child, Philadelphia, 1982, Lea & Febiger. Peck DM: Apo
You Might Also Like