First Metacarpal Corrective Osteotomy and Management of Rolando Fractures
Key Takeaway
The management of first carpometacarpal joint trauma, including Rolando fractures and malunions requiring corrective osteotomy, demands meticulous surgical precision. This guide details the Giachino corrective osteotomy technique for intra-articular malunions and advanced fixation strategies for comminuted first metacarpal base fractures. Emphasizing anatomic reduction, rigid fixation, and biomechanical restoration, these evidence-based protocols optimize functional outcomes and mitigate post-traumatic arthritis in the thumb carpometacarpal joint.
INTRODUCTION TO FIRST CARPOMETACARPAL JOINT TRAUMA
The first carpometacarpal (CMC) joint, or trapeziometacarpal joint, is a highly specialized biconcave saddle joint that provides the thumb with its unique combination of extensive mobility and profound stability. Because the thumb accounts for approximately 40% to 50% of overall hand function, traumatic disruptions to the first CMC joint—whether acute fractures or chronic malunions—can lead to devastating functional impairment.
During forceful pinch and grasp, the compressive loads transmitted across the first CMC joint can exceed 12 times the applied force at the thumb tip. Consequently, even minor articular step-offs or malalignments can drastically alter contact mechanics, leading to accelerated articular cartilage wear and early-onset post-traumatic osteoarthritis. The management of these complex injuries requires a profound understanding of local pathoanatomy, precise surgical execution, and rigid fixation to restore articular congruity and biomechanical axis.
CORRECTIVE OSTEOTOMY FOR FIRST METACARPAL MALUNION
Intra-articular fractures of the first metacarpal base that heal in a malunited position present a significant reconstructive challenge. When an articular step-off is left unreduced, the incongruity between the metacarpal base and the trapezium inevitably leads to degenerative joint disease. The Giachino corrective osteotomy is a highly effective, joint-preserving surgical technique designed to restore articular congruity in cases of intra-articular malunion.
Indications and Preoperative Planning
Corrective osteotomy is indicated for symptomatic intra-articular malunions of the first metacarpal base where the articular cartilage remains viable, and advanced osteoarthritic changes have not yet developed. Preoperative evaluation must include true anteroposterior (AP), lateral, and Robert’s view radiographs of the thumb to accurately quantify the articular step-off and angular deformity. Computed tomography (CT) with 3D reconstructions is highly recommended to map the exact topography of the malunited osteochondral fragment.
Surgical Pearl: The success of a corrective osteotomy relies heavily on the viability of the articular cartilage. If preoperative imaging or intraoperative inspection reveals full-thickness cartilage loss or diffuse eburnation, a salvage procedure such as trapeziometacarpal arthrodesis or suspensionplasty should be considered instead.
Surgical Anatomy and Approach
The base of the first metacarpal and the trapezium are approached through a modified Wagner or standard radial incision.
- Incision: Make a longitudinal or slightly curved incision along the radial border of the first metacarpal, extending proximally over the CMC joint.
- Superficial Dissection: Carefully identify and retract the sensory branches of the superficial radial nerve. The radial artery, which passes dorsally through the anatomic snuffbox and dives between the two heads of the first dorsal interosseous muscle, must be meticulously protected.
- Deep Dissection: Elevate the thenar musculature subperiosteally from the volar-radial aspect of the metacarpal shaft. Perform a longitudinal capsulotomy to expose the trapeziometacarpal joint, allowing direct visualization of the articular surface and the malunited step-off.
The Giachino Osteotomy Technique: Step-by-Step
The Giachino technique utilizes a precisely measured bone block resection to allow the malunited articular fragment to be mobilized, rotated, and anatomically reduced.
- Templating the Bone Block: Outline a rectangular block of bone to be removed from the radial aspect of the first metacarpal shaft. The width of this bone block must be slightly greater than the measured articular step-off. Crucially, the block must be long enough to accommodate subsequent internal fixation without risking iatrogenic splitting of the diaphyseal bone.
- Executing the Osteotomy: Utilizing a microsagittal saw under continuous saline irrigation to prevent thermal necrosis, make two transverse cuts into the metacarpal shaft. The distance between these two cuts should be the length of the articular step-off plus an additional 2 mm (Distance = b + 2 mm). This extra 2 mm provides the necessary spatial tolerance to manipulate and fit the fragments together seamlessly.
- Mobilizing the Fragments: Adduct the thumb shaft. This maneuver opens the radial aspect of the joint, providing an unobstructed view of the malaligned articular surface. Drive a fine, sharp osteotome parallel to the metacarpal shaft to free the fragments.
- Bone Graft Preservation: Retain the excised diaphyseal bone block (the stippled area in preoperative templating); this cancellous-rich bone will be utilized as local autograft to fill any resulting voids once the articular segment is reduced.
- Articular Reduction: Abduct the thumb to line up the proximal diaphyseal fragment with the original osteochondral piece that had healed in the malunited position. The primary objective is absolute articular congruity. The articular surface of the reconstructed metacarpal must perfectly match the biconcave articular surface of the trapezium.
- Fine-Tuning: Slightly rotate the mobilized osteochondral fragment as needed to ensure the articular contours are perfectly aligned.
- Provisional Fixation: Temporarily secure the reduced articular fragment to the metacarpal shaft using a 0.035-inch or 0.045-inch Kirschner wire (K-wire). Once provisionally fixed, thoroughly inspect the articular surface visually and fluoroscopically to confirm absolute congruity.
- Definitive Fixation: Once anatomic reduction is confirmed, definitive fixation is achieved using either multiple K-wires or, preferably, a small headless compression screw or minifragment lag screw, depending on the size of the osteochondral fragment. Pack the preserved local bone graft into any metaphyseal defects to promote rapid osteointegration.
- Closure: Repair the joint capsule meticulously to restore static stability, followed by standard layered closure of the subcutaneous tissues and skin.
Postoperative Rehabilitation Protocol
Postoperative care must balance the need for rigid immobilization to allow bone healing with the goal of preventing debilitating joint stiffness.
- Weeks 0-6: The patient is placed in a rigid, well-molded thumb spica cast. Absolute immobilization of the CMC joint is required during this phase to protect the osteotomy and allow primary bone healing.
- Weeks 6-8: The cast is removed, and clinical/radiographic evaluation is performed. If radiographic evidence of union is present, the patient is transitioned to a custom thermoplastic thumb spica splint, worn between exercise sessions. Active range of motion (AROM) exercises for the CMC, metacarpophalangeal (MCP), and interphalangeal (IP) joints are initiated.
- Weeks 8-12: Passive range of motion (PROM) and progressive strengthening exercises are introduced. Unrestricted activity is typically permitted after 12 weeks, contingent upon complete radiographic consolidation.
MANAGEMENT OF ROLANDO FRACTURES AND CMC COMMINUTION
While the Bennett fracture represents a simple, two-part intra-articular fracture-dislocation of the first metacarpal base, the Rolando fracture represents a significantly more complex injury pattern. First described by Silvio Rolando in 1910, this injury is classically defined as a Y-shaped or T-shaped intra-articular comminuted fracture of the thumb metacarpal base.
Pathoanatomy and Biomechanics
Unlike a Bennett fracture, where the strong anterior oblique ligament (beak ligament) retains the volar-ulnar fragment while the abductor pollicis longus (APL) subluxates the metacarpal shaft dorsally and proximally, a Rolando fracture typically does not result in severe diaphyseal displacement. Because the fracture is comminuted and involves both volar and dorsal articular fragments, the deforming forces of the APL and adductor pollicis tend to cause axial shortening and severe articular splaying rather than a classic subluxation.
Preoperative radiograph demonstrating a highly comminuted, intra-articular fracture of the first metacarpal base (Rolando variant) with significant axial shortening and articular splaying.
Because of the severe disruption to the articular surface, the likelihood of post-traumatic osteoarthritis is exceptionally high following a Rolando fracture. Therefore, the primary surgical objective is the anatomic restoration of the articular surface, combined with the restoration of metacarpal length and alignment.
Surgical Decision Making and Treatment Algorithm
The treatment of Rolando fractures is dictated by the degree of comminution and the size of the articular fragments.
- Large Articular Fragments (3-Part Fractures): Amenable to Open Reduction and Internal Fixation (ORIF) using minifragment T-plates or lag screws.
- Moderate Comminution: Best managed with Closed Reduction and Percutaneous Pinning (CRPP) or limited open reduction with K-wire fixation.
- Severe Comminution (Pilon-type): Requires joint-spanning external fixation (ligamentotaxis) combined with limited internal fixation and bone grafting.
Surgical Warning: Extensive soft tissue stripping to achieve perfect radiographic reduction in highly comminuted Rolando fractures often leads to devascularization of the small articular fragments, resulting in avascular necrosis and catastrophic joint failure. In severe comminution, prioritize length, alignment, and rotation over absolute anatomic reduction of every microscopic fragment.
Closed Reduction and Percutaneous Pinning (CRPP)
In many Rolando-type fractures, the joint surface fragments can be reasonably well reduced via longitudinal traction and closed manipulation, followed by percutaneous pinning.
- Reduction: Apply longitudinal traction to the thumb to overcome the deforming forces of the APL and adductor pollicis. Apply direct manual pressure over the volar and dorsal aspects of the metacarpal base to compress the splayed articular fragments.
- Articular Pinning: Under fluoroscopic guidance, introduce 0.035-inch K-wires transversely or obliquely directly under the subchondral bone to capture and compress the articular fragments together.
- Transarticular Pinning: Once the articular block is reconstituted, it must be secured to the trapezium to maintain length and prevent axial settling. Advance a larger 0.062-inch K-wire from the metacarpal shaft, across the CMC joint, and into the trapezium. Occasionally, a transmetacarpal pin into the second metacarpal is utilized for additional rotational stability.

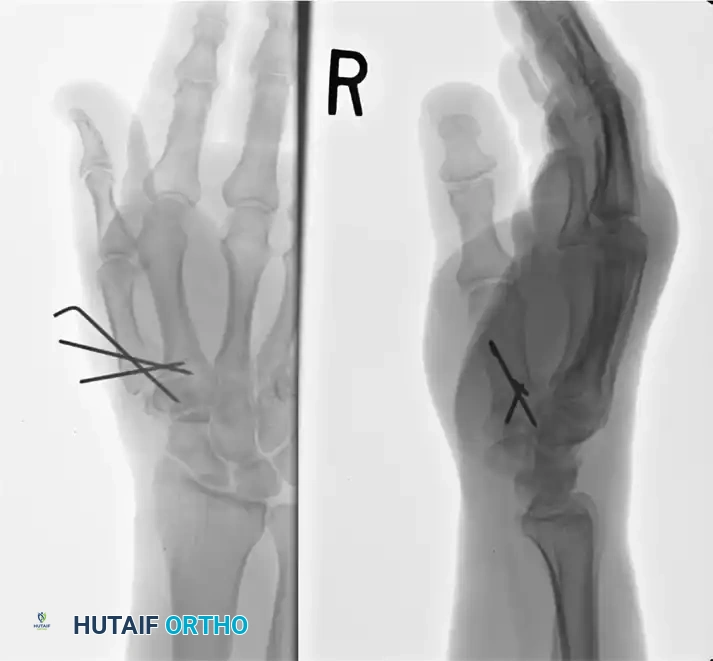
Postoperative radiograph demonstrating successful reconstruction. The articular segments were initially reduced and stabilized with 0.035-inch K-wires, followed by rigid metacarpal-trapezial transarticular pinning utilizing a 0.062-inch K-wire to maintain length and alignment.
Open Reduction and Internal Fixation (ORIF) with Plating
If the articular fragments are of sufficient size to accept screw fixation without shattering, ORIF provides the most biomechanically stable construct, allowing for earlier mobilization.
- Approach: A standard Wagner incision is utilized.
- Reduction: The joint is opened, and the hematoma is evacuated. The articular fragments are anatomically reduced under direct vision and provisionally held with reduction forceps or fine K-wires.
- Plating: A 1.5 mm or 2.0 mm minifragment T-plate or L-plate is applied to the radial or dorsal-radial aspect of the metacarpal. The transverse limb of the plate supports the articular fragments (acting as a buttress), while the longitudinal limb secures the construct to the metacarpal diaphysis.
External Fixation and Tension Band Constructs
For fractures with moderate to severe comminution where plating is impossible, the combination of tension band wiring and an external fixator is a highly effective strategy.
- External Fixation: A mini-external fixator is applied spanning the first CMC joint. Pins are placed in the trapezium (or distal radius) and the distal shaft of the first metacarpal. Distraction is applied to utilize the principle of ligamentotaxis, which restores metacarpal length and helps align the comminuted articular fragments via tension on the intact capsuloligamentous structures.
- Tension Band Wiring: Once length is restored, a tension band wire construct can be applied to the base of the metacarpal to provide dynamic compression and stability to the major fracture fragments.
- Fixator Management: If the resulting fracture construct is deemed highly stable, the external fixator may be removed relatively early. However, in most cases of severe comminution, the fixator should remain in place for 6 to 8 weeks to prevent axial collapse during the early phases of bone healing.
Management of Severe Comminution (Thumb Pilon Fractures)
Severely comminuted fractures—often referred to as thumb pilon fractures—represent the most extreme end of the spectrum. These injuries require a multimodal approach combining external fixation, limited internal fixation (K-wires), and structural bone grafting.
- Ligamentotaxis: An external fixator is applied to restore length.
- Limited Fixation: Fine K-wires are used to piece together the largest articular fragments.
- Bone Grafting: Because the metaphyseal cancellous bone is often severely impacted, restoring length via distraction creates a significant metaphyseal void. This void must be filled with cancellous autograft (typically harvested from the distal radius) to provide subchondral support and prevent late articular subsidence.
Clinical studies have demonstrated that this combined technique yields good functional results, even in the presence of persistent radiographic joint irregularities. Interestingly, in the context of severe first CMC joint trauma, the radiographic quality of the final reduction does not always strictly correlate with the late occurrence of clinical symptoms or the severity of osteoarthritic pain. Nonetheless, the fundamental surgical mandate remains: the joint articulation must be restored as close to its normal anatomic state as technically feasible to optimize long-term survivorship of the thumb carpometacarpal joint.
You Might Also Like

