Masterclass in Calcaneal Fractures: Evaluation and Surgical Management
Key Takeaway
Calcaneal fractures are complex injuries often resulting from high-energy axial loads. Successful management requires a profound understanding of hindfoot biomechanics, meticulous soft-tissue handling, and precise articular reduction. This guide details the evidence-based evaluation, CT-based Sanders classification, and step-by-step surgical techniques—including the extensile lateral approach—necessary to optimize functional outcomes and minimize debilitating complications such as subtalar arthritis and wound necrosis.
Introduction to Calcaneal Fractures
The management of calcaneal fractures has evolved significantly from historical nonoperative nihilism to modern, precise surgical reconstruction. Studies in fracture patterns, soft-tissue management, and long-term outcomes have provided a clear, evidence-based understanding of which injuries benefit from early surgical intervention and which are prone to high complication rates.
Regardless of the chosen treatment modality, calcaneal fractures are notorious for their association with numerous complications and significant long-term quality-of-life detriments. In a landmark study, van Tetering and Buckley evaluated patients with calcaneal fractures using the validated Short-Form 36 (SF-36) Health Status Survey. When comparing these patients to normal individuals and those with other major health issues, they concluded that outcomes in patients with calcaneal fractures were significantly worse than those with other orthopedic conditions, and remarkably, worse than patients recovering from myocardial infarctions or organ transplants. This underscores the critical need for meticulous, anatomically precise management.
Anatomy and Biomechanics
The calcaneus is the largest tarsal bone, serving as the foundation of the longitudinal arch and the primary lever arm for the Achilles tendon. It articulates superiorly with the talus (via the anterior, middle, and posterior facets) and anteriorly with the cuboid.
Extraarticular Fractures
Calcaneal fractures are broadly divided into extraarticular (sparing the subtalar joint) and intraarticular (involving the subtalar joint) patterns. Extraarticular fractures typically involve the calcaneal body, anterior process, or tuberosity. Most can be managed with cast or brace immobilization and strict non-weight-bearing protocols for 6 weeks.
A critical exception is the displaced tuberosity avulsion fracture.
Clinical Pearl: A "beak" fracture that does not involve the Achilles tendon insertion can often be treated nonoperatively if displacement is minimal (< 1 cm). However, a true avulsion fracture involving the Achilles insertion demands urgent open reduction and internal fixation (ORIF). Failure to intervene leads to loss of plantarflexion power, severe skin compromise posteriorly, and a widened heel that complicates shoe wear. Fixation is typically achieved using large, partially threaded cancellous screws.
Another easily missed extraarticular injury is the avulsion of the anterior process by the bifurcate ligament. Often misdiagnosed as a severe lateral ankle sprain, this fracture should be suspected in patients with prolonged lateral midfoot pain following an inversion injury. If the fragment is small or the diagnosis is delayed, simple excision yields excellent results.
Intraarticular Fractures
Intraarticular fractures account for approximately 75% of all calcaneal fractures. Historically associated with dismal functional outcomes, these fractures are uniformly caused by high-energy axial loading mechanisms, such as falls from a height or motor vehicle collisions.
Due to the high-energy nature of the injury, surgeons must maintain a high index of suspicion for associated axial load injuries. Approximately 10% of patients will have an associated lumbar spine fracture, and others may present with pelvic ring disruptions or tibial plateau fractures.
Mechanism of Injury and Fracture Pathoanatomy
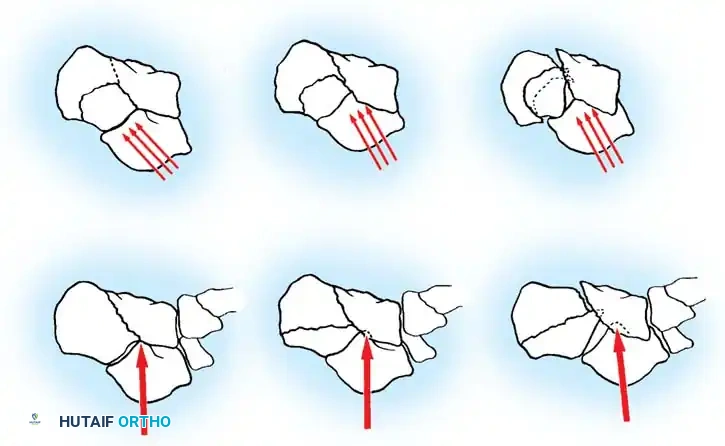
Cadaveric studies, anatomical dissections, and advanced computed tomography (CT) have elucidated the precise mechanism of intraarticular calcaneal fractures. The contact point of the calcaneus with the ground is situated lateral to the primary weight-bearing axis of the lower extremity.
When an axial load is applied, the lateral process of the talus acts as a wedge, driving into the crucial angle of Gissane. Shear forces are directed through the posterior facet toward the medial wall of the calcaneus.
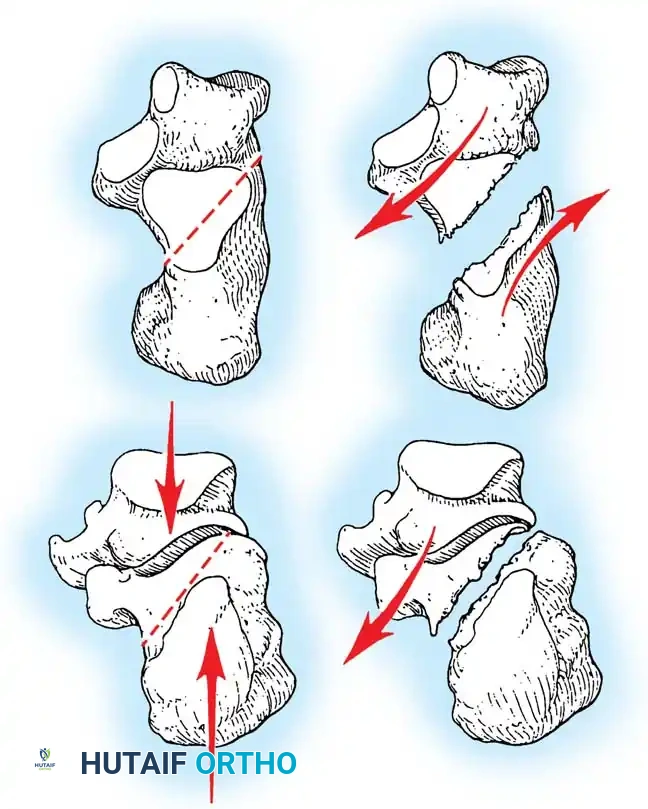
The Primary Fracture Line
This shear force creates the primary fracture line, which is almost universally present. It extends from the proximal, medial aspect of the calcaneal tuberosity, obliquely through the anterolateral wall, typically exiting near the crucial angle of Gissane. The position of this line through the posterior facet is variable; it may occur in the medial third (near the sustentaculum tali), the central third, or the lateral third.
This primary line divides the calcaneus into two main fragments:
1. The Sustentacular (Anteromedial) Fragment: This fragment remains securely attached to the talus via the robust interosseous talocalcaneal and deltoid ligaments. It is considered the "constant fragment" and serves as the foundation for surgical reconstruction.
2. The Tuberosity (Posterolateral) Fragment: This fragment is displaced superiorly, laterally, and into varus by the pull of the Achilles tendon and the impact of the injury.
Secondary Fracture Lines and the Essex-Lopresti Classification
As the axial force continues, the medial spike of the sustentacular fragment is driven medially, threatening the neurovascular bundle, while secondary fracture lines propagate through the posterior facet.
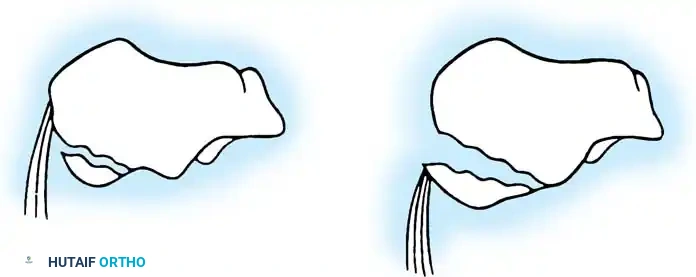
Essex-Lopresti classically described two distinct patterns based on the exit point of the secondary fracture line:
- Joint Depression Type: The secondary fracture line exits posterior to the posterior facet but anterior to the Achilles tendon insertion. The articular fragment is driven deep into the cancellous body of the calcaneus.
- Tongue Type: The secondary fracture line exits posterior to the Achilles tendon insertion. The posterior facet remains attached to the posterior tuberosity, creating a single, large "tongue" piece that rotates dorsally.
Surgical Warning: As the talus impacts the calcaneus, it blows out the lateral wall, severely compressing the subfibular space. This leads to peroneal tendon impingement or dislocation. Furthermore, the medial spike is driven deep into the medial soft tissues. Medially open fractures require meticulous deep dissection to expose, irrigate, and debride this medial spike; superficial skin debridement is grossly inadequate.
Radiographic Evaluation
A comprehensive radiographic series is mandatory for initial assessment. The standard trauma series should include five specific views:
- Lateral View: Assesses the loss of calcaneal height, rotation of the posterior facet, and the Böhler angle.
- Axial (Harris) View: Evaluates the varus/valgus alignment of the tuberosity, heel widening, and lateral wall blowout.
- Anteroposterior (AP) View: Assesses calcaneocuboid joint involvement.
- Oblique View: Highlights the anterior process and the calcaneocuboid articulation.
- Brodén View: Used intraoperatively and postoperatively to evaluate the congruency of the posterior facet.
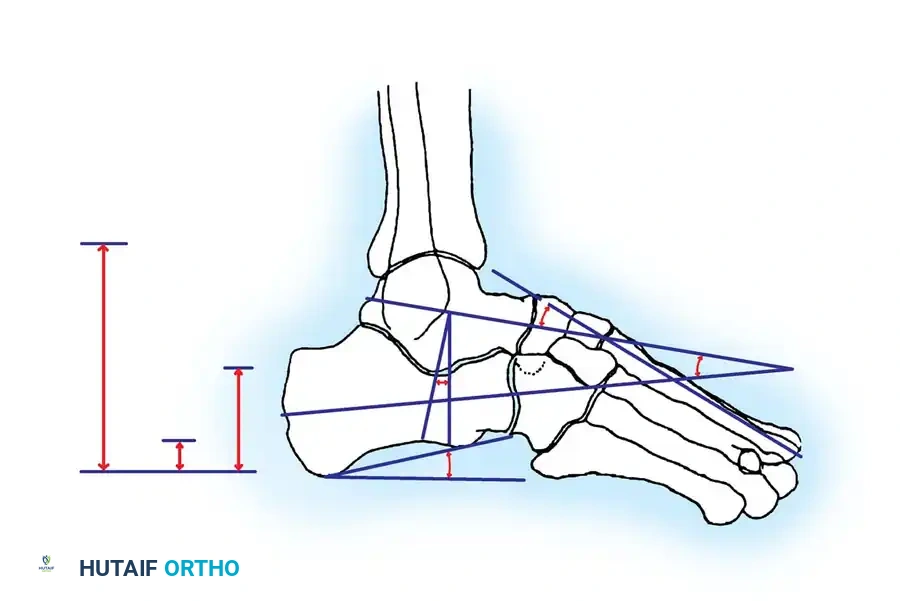
Böhler's Angle
The Böhler angle is formed by the intersection of two lines on the lateral radiograph: one drawn from the highest point of the anterior process to the highest point of the posterior facet, and another from the highest point of the posterior facet to the highest point of the calcaneal tuberosity.
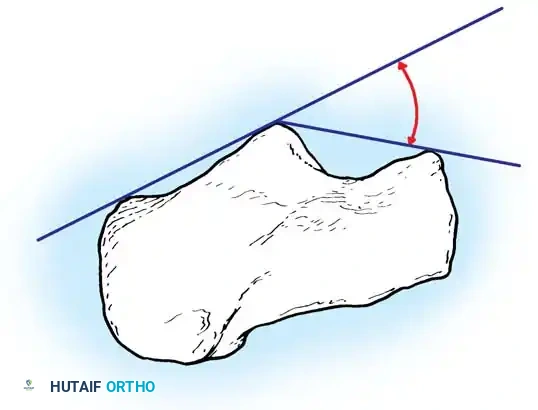
A normal Böhler angle ranges from 25° to 40°. In intraarticular fractures, this angle is typically flattened or reversed, indicating severe collapse of the posterior facet and loss of calcaneal height.

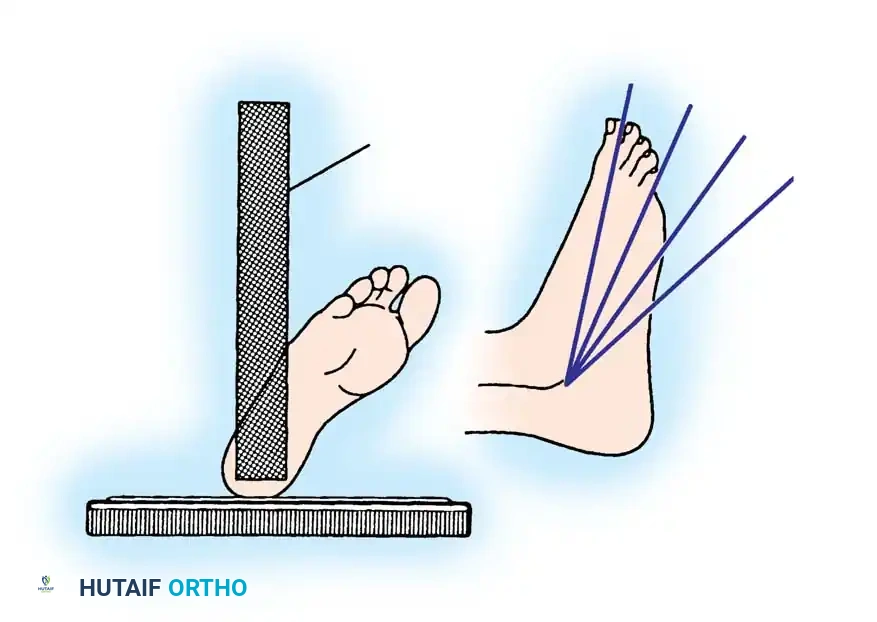
The Brodén View
The Brodén view is critical for visualizing the posterior facet. It is obtained by internally rotating the leg 40 degrees with the ankle in neutral dorsiflexion. The x-ray beam is then angled cephalad at 10, 20, 30, and 40 degrees to visualize different portions of the facet from posterior to anterior.
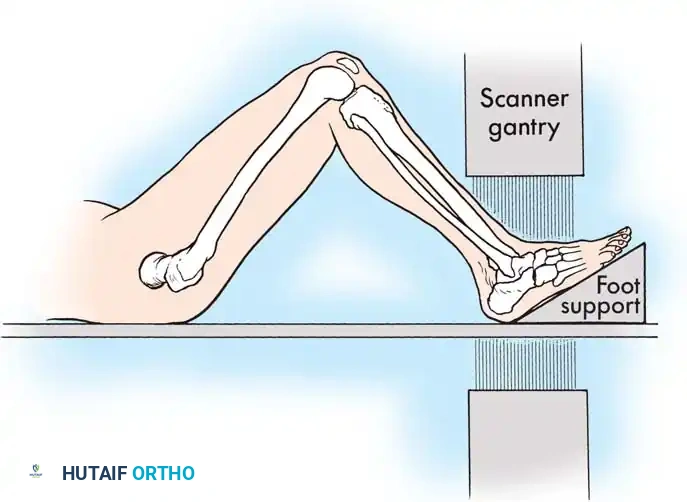
Computed Tomography (CT)
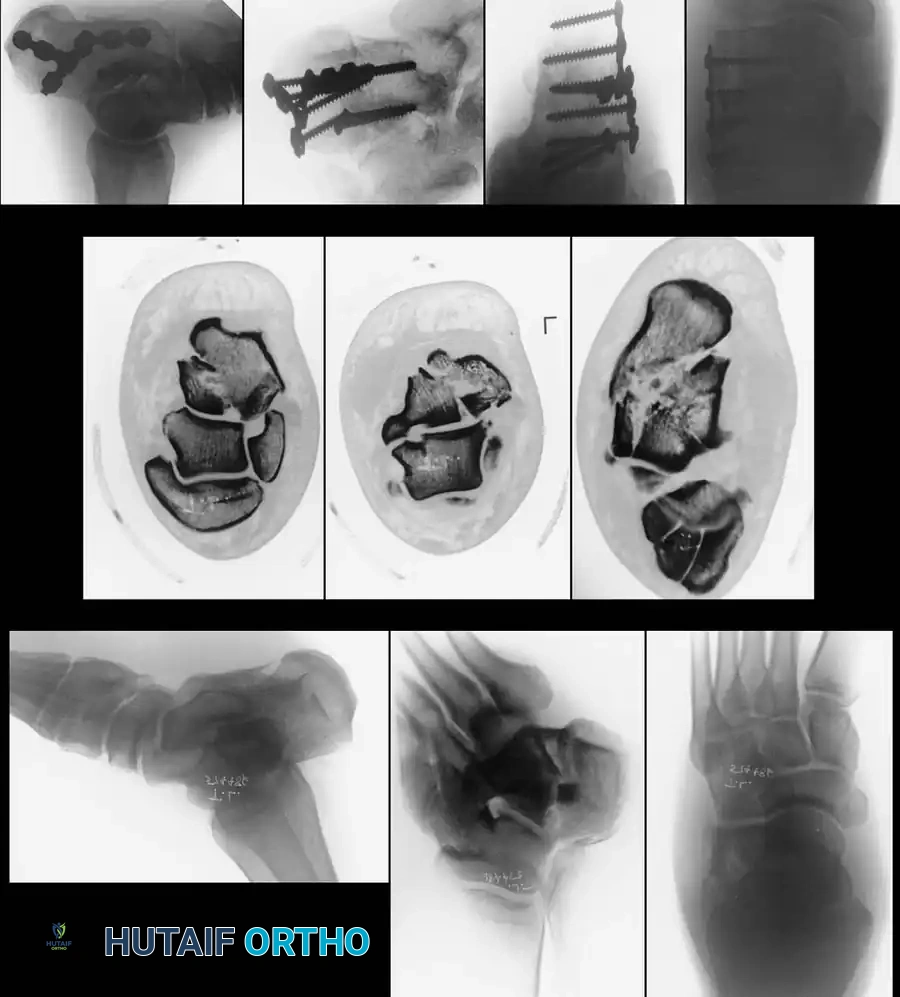
While plain films are essential, CT scanning is the gold standard for evaluating intraarticular calcaneal fractures. Scans must be ordered in two specific planes:
* Semicoronal Plane: Oriented perpendicular to the normal position of the posterior facet. This is the most critical view for assessing articular comminution and classifying the fracture.
* Axial Plane: Oriented parallel to the sole of the foot, excellent for evaluating the calcaneocuboid joint and the sustentaculum tali.
Modern Classification Systems
While the Essex-Lopresti system is excellent for understanding the secondary fracture line, it fails to quantify the energy absorbed by the posterior facet or the degree of comminution.
The Sanders Classification
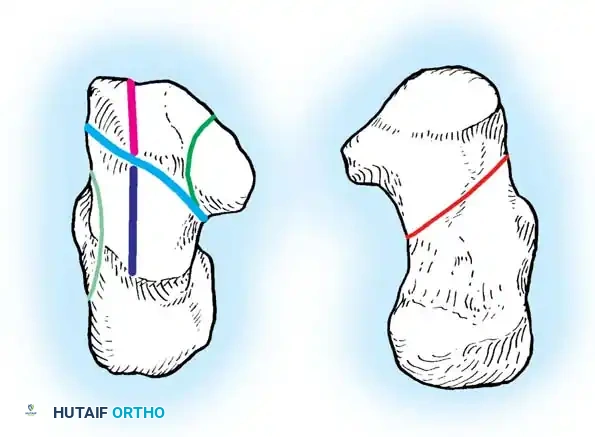
The Sanders classification has become the universally accepted system for intraarticular calcaneal fractures. It is based on the number and location of articular fracture lines seen on the semicoronal CT image showing the widest portion of the posterior facet.
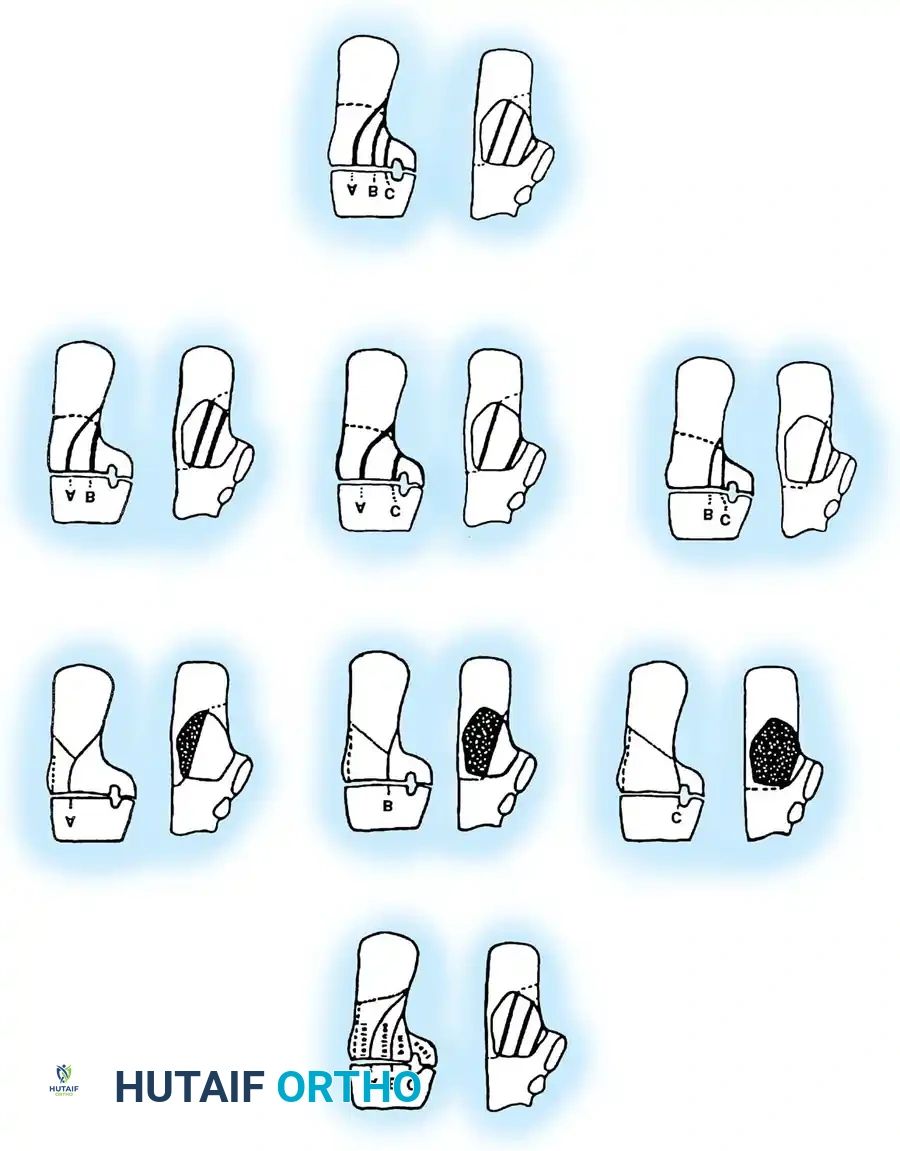
The posterior facet is divided into three potential fracture lines (A, B, and C), creating four potential fragments (lateral, central, medial, and sustentacular).
* Type I: All nondisplaced fractures (regardless of the number of fracture lines).
* Type II: Two-part fractures of the posterior facet (one fracture line). Subdivided into IIA, IIB, or IIC based on the location of the line.
* Type III: Three-part fractures (two fracture lines), featuring a centrally depressed fragment. Subdivided into IIIAB, IIIAC, or IIIBC.
* Type IV: Four-part (or more) highly comminuted fractures.
Clinical Pearl: Ebraheim et al. demonstrated that CT scans may occasionally underestimate the sagittal plane rotation of a depressed fragment. Therefore, plain lateral radiographs must always be correlated with CT findings to fully appreciate the three-dimensional deformity.
Decision Making and Indications for Treatment
The decision to proceed with operative versus nonoperative management is highly nuanced.
Nonoperative Management
Closed treatment (casting, compression dressings, early mobilization) is generally reserved for:
* Sanders Type I (nondisplaced) fractures.
* Patients with severe peripheral vascular disease (PVD) or poorly controlled diabetes.
* Heavy smokers (due to unacceptably high rates of wound necrosis).
* Non-ambulatory patients or those with severe medical comorbidities.
Operative Management
Kundel et al. compared operative and nonoperative treatments, noting that the primary statistically significant advantage of surgery was the ability of patients to return to their previous occupation. However, they emphasized that ORIF only benefits patients if a near-anatomical reconstruction of the joint and restoration of the Böhler angle is achieved.
Crosby and Fitzgibbons demonstrated that Type II and III fractures treated with ORIF yielded superior functional outcomes compared to closed methods, provided the soft tissue envelope was respected.
Surgical Approaches and Techniques
Timing is critical. Surgery must be delayed until the "wrinkle sign" is present, indicating that soft-tissue swelling has subsided (typically 10 to 21 days post-injury). Operating through edematous, blistered skin guarantees catastrophic wound complications.
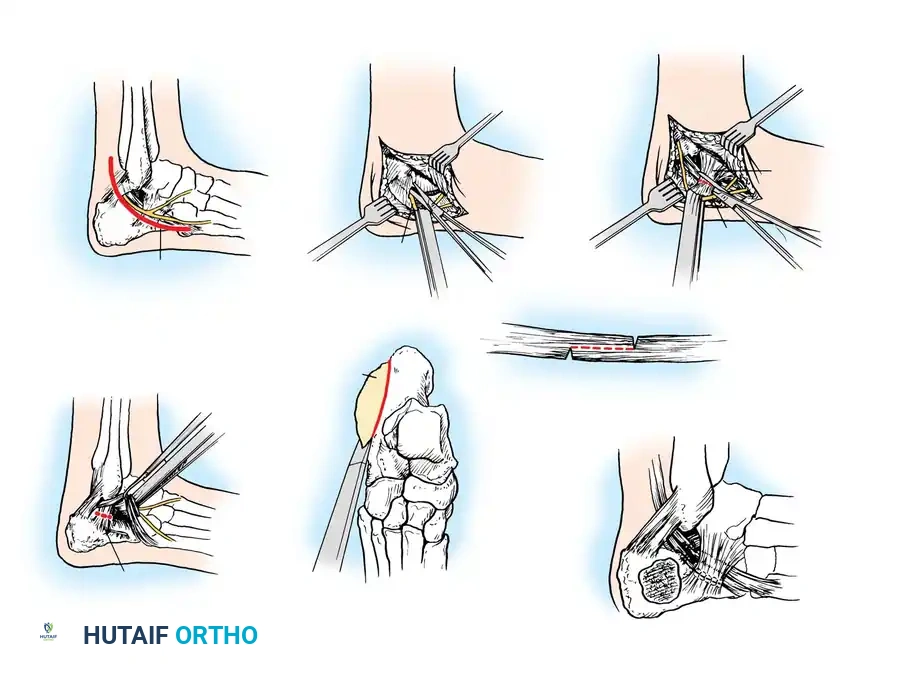
The Extensile Lateral Approach
The workhorse for calcaneal ORIF is the extensile lateral approach.
- Positioning: The patient is placed in the lateral decubitus position. A thigh tourniquet is applied.
- Incision: An L-shaped incision is made. The vertical limb is placed just anterior to the Achilles tendon, and the horizontal limb is placed in line with the base of the fifth metatarsal, transitioning between the glabrous (plantar) and non-glabrous (lateral) skin.
- Flap Creation: A full-thickness subperiosteal flap is elevated. It is imperative to use a "no-touch" technique. Retraction is achieved by placing stout Kirschner wires (K-wires) into the fibula, talar neck, and cuboid, bending them to hold the flap out of the surgical field without using self-retaining retractors that crush the skin edges.
Reduction Sequence
The reduction follows a strict, logical sequence:
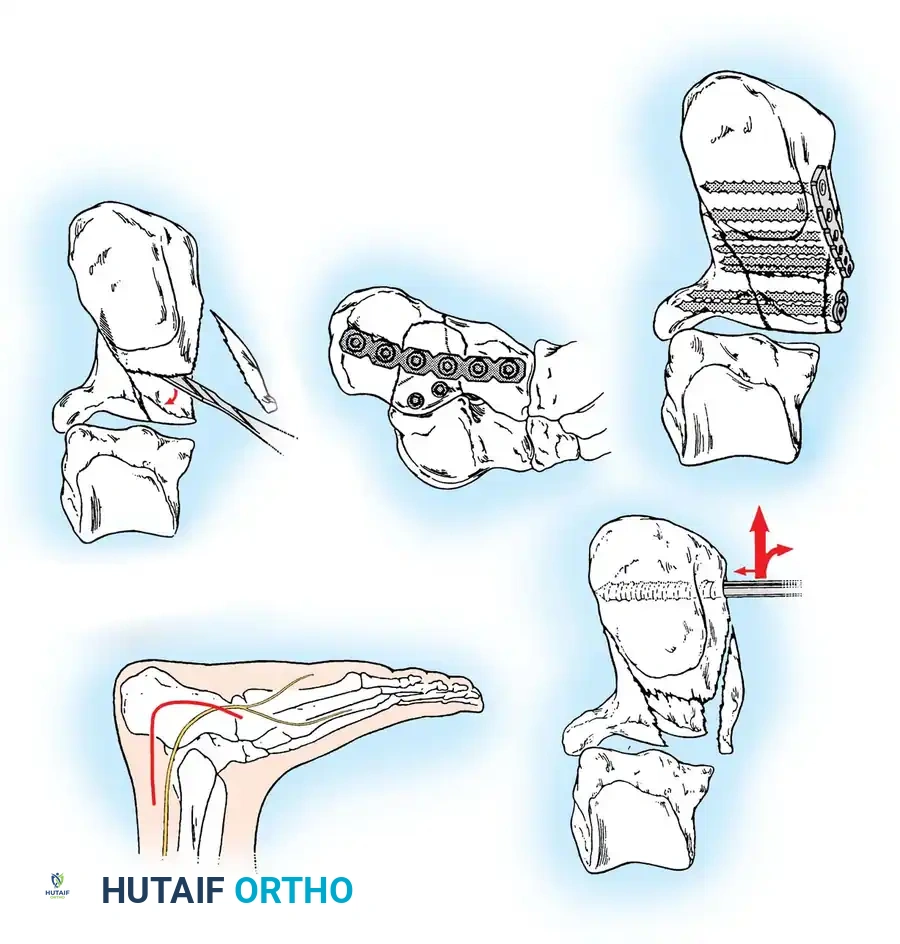
- Decompression: The lateral wall blowout is reflected inferiorly to expose the depressed posterior facet and the subtalar joint.
- Tuberosity to Sustentaculum: A Schanz pin is placed into the posteroinferior tuberosity. Using the pin as a joystick, the tuberosity is pulled out of varus, translated medially, and pulled plantarly to restore length, height, and alignment. It is temporarily pinned to the constant sustentacular fragment.
- Posterior Facet Reduction: The depressed articular fragments are elevated to match the intact articular surface of the talus.

- Anterior Process: If the calcaneocuboid joint is involved, it is reduced and pinned.
- Lateral Wall: The lateral wall is reduced to decompress the subfibular space, ensuring the peroneal tendons have adequate excursion.
Internal Fixation
Once anatomical reduction is confirmed via fluoroscopy (including Brodén views), definitive fixation is applied. A low-profile, anatomically contoured calcaneal locking plate is typically utilized.
Screws must be directed from lateral to medial, specifically targeting the dense bone of the sustentaculum tali to anchor the construct.
Percutaneous and Minimally Invasive Techniques
For specific fracture patterns, particularly the Essex-Lopresti Tongue-Type fractures, percutaneous reduction and screw fixation can yield excellent results with minimal soft-tissue risk.
Using the classic Essex-Lopresti maneuver, a heavy Schanz pin or Steinmann pin is introduced percutaneously into the posterior aspect of the tongue fragment. The knee is flexed to relax the Achilles tendon, and the pin is used to lever the fragment plantarly, restoring the posterior facet congruity.
Once reduced, the fragment is secured with percutaneous cannulated screws directed from the posterior tuberosity into the anterior calcaneus.
Postoperative Protocol
Meticulous postoperative care is as critical as the surgery itself.
* Wound Care: The foot is placed in a bulky, non-compressive Jones dressing with a posterior splint in neutral dorsiflexion. The drain (if used) is removed at 24-48 hours.
* Weight-Bearing: Patients are kept strictly non-weight-bearing for 10 to 12 weeks to prevent late collapse of the posterior facet.
* Rehabilitation: Early active range of motion (ROM) of the ankle and subtalar joints is initiated at 2 to 3 weeks once the surgical incision has completely healed.
Complications and Prevention
Calcaneal fractures are fraught with complications, demanding immense respect from the operating surgeon.
- Wound Dehiscence and Infection: The most feared acute complication, occurring in up to 25% of cases. Prevention relies on delaying surgery until swelling resolves, utilizing the "no-touch" flap technique, and avoiding surgery in high-risk patients (smokers, diabetics).
- Subtalar Arthritis: Post-traumatic arthritis is common, especially in Sanders Type III and IV fractures. If conservative measures (bracing, injections) fail, a subtalar arthrodesis is required.
3.
You Might Also Like

