Comprehensive Management of Femoral Malunions: Supracondylar and Diaphyseal Strategies
Key Takeaway
Femoral malunions present complex biomechanical challenges, often resulting in gait disturbances and abnormal joint stresses. Significant malunions—defined by shortening greater than 2.5 cm, angulation exceeding 10 degrees, or severe rotational deformity—require meticulous surgical correction. Treatment strategies range from single-stage intramedullary nailing to complex two-stage osteotomies with external fixation. Successful management demands precise preoperative planning, rigid internal fixation, and an understanding of multi-planar deformity correction to restore lower extremity alignment and function.
INTRODUCTION TO FEMORAL MALUNIONS
The management of femoral malunions represents a formidable challenge in reconstructive orthopedic surgery. While the advent and widespread adoption of interlocking intramedullary (IM) nailing have drastically reduced the incidence of diaphyseal malunions, complex deformities still arise following nonoperative management, unlocked nailing, or the failure of initial fixation constructs. Malunions of the femur alter the mechanical axis of the lower extremity, leading to profound disturbances in gait, posture, and energy expenditure. Consequently, these deformities can impart abnormal, asymmetric stresses across the adjacent knee and hip joints, as well as the lumbar spine.
Surgical correction of a femoral malunion is a technically demanding endeavor that requires a comprehensive understanding of lower extremity biomechanics, multi-planar deformity analysis, and advanced osteosynthesis techniques. This guide delineates the evidence-based protocols for addressing both supracondylar and femoral shaft malunions, providing a masterclass in preoperative planning, surgical execution, and postoperative rehabilitation.
SUPRACONDYLAR FEMORAL MALUNIONS
Pathoanatomy and Biomechanics
Supracondylar femoral malunions are relatively infrequently reported in contemporary literature, largely due to the success of modern locking plate technology and retrograde intramedullary nailing for acute distal femur fractures. However, when they do occur, they present a complex reconstructive dilemma. The most common and challenging deformity pattern involves an angular varus collapse of the medial condyle coupled with significant limb shortening. This is primarily driven by the unopposed pull of the adductor magnus on the medial femoral condyle and the gastrocnemius on the distal fragment, leading to apex-lateral (varus) and apex-posterior (extension) angulation.
Clinical Evaluation and Indications
Patients typically present with a noticeable limb-length discrepancy (LLD), a varus thrust during the stance phase of gait, and medial compartment knee pain. Surgical intervention is indicated when the mechanical axis deviation causes symptomatic joint overload or when the LLD exceeds 2.0 to 2.5 cm, significantly impairing gait efficiency.
CLINICAL PEARL: All patients presenting with a supracondylar malunion and at least 10 degrees of varus angulation will predictably develop medial knee pain due to the exponential increase in medial compartment contact pressures. Early corrective osteotomy is paramount to preserving the articular cartilage.
Surgical Techniques for Supracondylar Correction
One-Stage Intramedullary Nailing
Wu described a highly effective one-stage surgical technique utilizing antegrade intramedullary nailing for supracondylar femoral fracture malunions associated with medial condyle varus deformity and shortening. In a cohort of 19 patients, the technique demonstrated excellent reliability. The procedure involves a corrective osteotomy at the apex of the deformity, followed by aggressive soft tissue release and distraction over the intramedullary nail.
Sixteen of the fractures healed without the need for additional surgery at a median period of 4.5 months. The amount of lengthening obtained intraoperatively ranged from 2.0 to 3.5 cm. Complications were minimal but included nonunion in one patient and deep infection in another. Notably, no recurrent malunions or neurovascular injuries occurred, highlighting the safety profile of this approach when executed meticulously.
External Fixation and Plating (Two-Stage or Hybrid Approach)
For severe, multi-planar deformities where acute correction may compromise the neurovascular bundle, a staged approach is often necessary.

FIGURE 58-23 A: Distal femoral fracture presenting with a severe 30-degree varus malunion.

FIGURE 58-23 B: Application of a circular external fixator to gradually correct the deformity and restore length prior to definitive internal fixation.

FIGURE 58-23 C: Final radiographic appearance after external fixator removal, corrective osteotomy, and rigid plate osteosynthesis.
In cases of profound articular destruction or end-stage post-traumatic osteoarthritis secondary to a long-standing malunion, salvage procedures such as compression arthrodesis may be indicated to provide a stable, painless limb.

FIGURE 58-21: Radiograph 3.5 months after compression arthrodesis for a severe distal femoral malunion with articular collapse. The knee is stable and painless.
FEMORAL SHAFT MALUNIONS
Epidemiology and Biomechanical Consequences
Malunions of femoral shaft fractures have become much less common with the increased popularity and refinement of interlocking intramedullary nail procedures. Historically, malunions after closed treatment (e.g., traction and casting) were the rule rather than the exception. Today, diaphyseal malunions become clinically significant and warrant surgical intervention only if they meet specific criteria:
* Shortening: Greater than 2.5 cm.
* Angulation: Greater than 10 degrees in the coronal or sagittal plane.
* Rotation: Internal or external rotation to the point that the knee cannot be aligned with forward motion during the stance phase of gait.
Although many authors define a rotational malunion as 10 degrees or more of axial malalignment, clinical symptoms vary widely. Studies indicate that 0% of patients are symptomatic with less than 10 degrees of rotational deformity; 12% are symptomatic with 10 to 15 degrees; and up to 38% experience significant symptoms with greater than 15 degrees of malrotation.
Interestingly, whether a femoral shaft fracture malunion directly leads to the development of knee osteoarthritis remains a subject of academic debate. Phillips et al., in a long-term study of 62 patients with femoral shaft fractures, found no significant association between the presence of a malunion, WOMAC scores, and the development of clinical or radiographic osteoarthritis at a 22-year follow-up. However, corrective surgery is still heavily planned based on the patient’s overall medical condition, functional demands, and the severity of the gait disturbance.
Rotational Deformity Correction
Rotational malunions frequently occurred in the era of unlocked intramedullary nailing or when comminuted fractures were fixed without adequate attention to cortical step-signs or linea aspera alignment.

FIGURE 58-22 A: Rotational malunion of the femur following unlocked intramedullary nailing.

FIGURE 58-22 B: Intraoperative correction of the malunion utilizing a proximal femoral derotational osteotomy and subsequent locked intramedullary nailing.

FIGURE 58-22 C: Radiographic evidence of a fully healed osteotomy with restored axial alignment.
Similarly, subtrochanteric fractures are highly susceptible to rotational and angular malunions due to the deforming forces of the iliopsoas (flexion and external rotation) and the gluteus medius/minimus (abduction).

FIGURE 58-24 A: Anteroposterior radiograph demonstrating a malunion of a subtrochanteric fracture.

FIGURE 58-24 B: Lateral radiograph of the same subtrochanteric malunion highlighting severe internal rotational deformity.

FIGURE 58-24 C: Postoperative AP radiograph following corrective osteotomy, removal of the previous implant, and rigid fixation with a proximal interlocking Grosse-Kempf medullary nail.

FIGURE 58-24 D: Postoperative lateral radiograph confirming restoration of sagittal alignment and rotation.
PREOPERATIVE PLANNING AND PATIENT SELECTION
When corrective surgery is planned, the surgeon must meticulously evaluate the patient's physiologic age, bone quality, and soft tissue envelope.
Contraindications
Extensive scarring, a history of deep infection, severe nerve injury, or multiple previous failed bone grafting procedures are considered relative or absolute contraindications to acute, single-stage corrective osteotomy. In such scenarios, the risk of catastrophic complications (e.g., infected nonunion, amputation) outweighs the functional benefits of realignment.
Pediatric Considerations
Angular deformity has been reported to occur in up to 40% of children with femoral shaft fractures treated nonoperatively. However, due to the immense remodeling potential of the pediatric physis, these deformities usually correct spontaneously over time, provided the child has at least 2 years of growth remaining. Surgical intervention in young children is generally reserved for overlapping that results in a final, projected limb shortening of more than 3.8 cm.
Adult Limb-Length Discrepancy Guidelines
In young adults, surgery is usually indicated when the overlap or shortening is more than 3.8 cm. However, the operation is technically demanding. Union may be delayed after surgery, and there is a significant risk of postoperative knee stiffness and impairment of the vascular and nerve supplies to the extremity due to acute stretching.
SURGICAL WARNING: When marked osteoporosis is present, the patient should be encouraged to bear weight before surgery until the osteopenia has at least partially resolved and localized pain and swelling have ceased. Operating on severely osteoporotic bone drastically increases the risk of hardware failure and iatrogenic fracture during deformity correction.
SURGICAL APPROACHES AND OPERATIVE TECHNIQUES
Patient Positioning and Setup
Any operation for a malunited femoral fracture in an adult is significantly easier with the patient positioned on a fracture table. This allows for controlled traction, precise rotational adjustments, and unhindered fluoroscopic access. The affected extremity should be meticulously draped into the sterile field, and the footpiece must be covered with sterile drapes to allow intraoperative manipulation if necessary.
Identifying the Fracture Plane
Although the old fracture line can be seen clearly on preoperative radiographs, the ends of the bone fragments may be encased in a massive volume of mature callus. Even after extensive subperiosteal stripping of the soft tissues, the exact plane of the original fracture can be exceedingly difficult to recognize at the time of surgery.
CLINICAL PEARL: To aid in identifying the fracture and in placing the osteotomy properly, drill a Kirschner wire (K-wire) or a small Steinmann pin through the bone in what appears to be the plane of the fracture. The relative positions of the wire and the fracture are then verified using an image intensifier.
Alternatively, if the original fracture plane is obliterated, the thickened part of the bone can be divided by a long oblique osteotomy. This technique produces a much larger surface area for the apposition of the fragments after length and alignment have been restored, thereby enhancing the biological environment for union.
Osteotomy and Fixation Strategies
Plate Osteosynthesis vs. Intramedullary Nailing
The successful use of oblique osteotomy combined with intramedullary nailing and autogenous bone grafting is well documented. However, oblique osteotomy using plate osteosynthesis and autogenous bone grafting remains a highly viable alternative. Plate fixation of femoral osteotomies is often preferred in cases where the femoral canal is severely distorted, obliterated by dense sclerotic bone, or when the fracture is located in the extreme distal part of the femur.
Chiodo et al. utilized an oblique osteotomy combined with closing wedges to correct complex coronal, transverse, and sagittal plane deformities in six femoral malunions. All six femurs presented with varus (average 22 degrees) and antecurvatum (average 23 degrees) deformities, and two had internal rotation deformities (10 degrees and 15 degrees). Fixation was performed with 4.5-mm lag screws and broad 4.5-mm compression plates in five malunions, and a 95-degree blade plate in one. All patients improved clinically, and all osteotomies healed. The average postoperative limb-length discrepancy was within 0.5 cm, and axial limb alignment was restored to within 10 degrees of the contralateral side.
One-Stage Z-Lengthening
For significant shortening without severe angular deformity, a Z-shaped step-cut osteotomy allows for controlled lengthening while maintaining rotational stability and a broad surface area for healing.
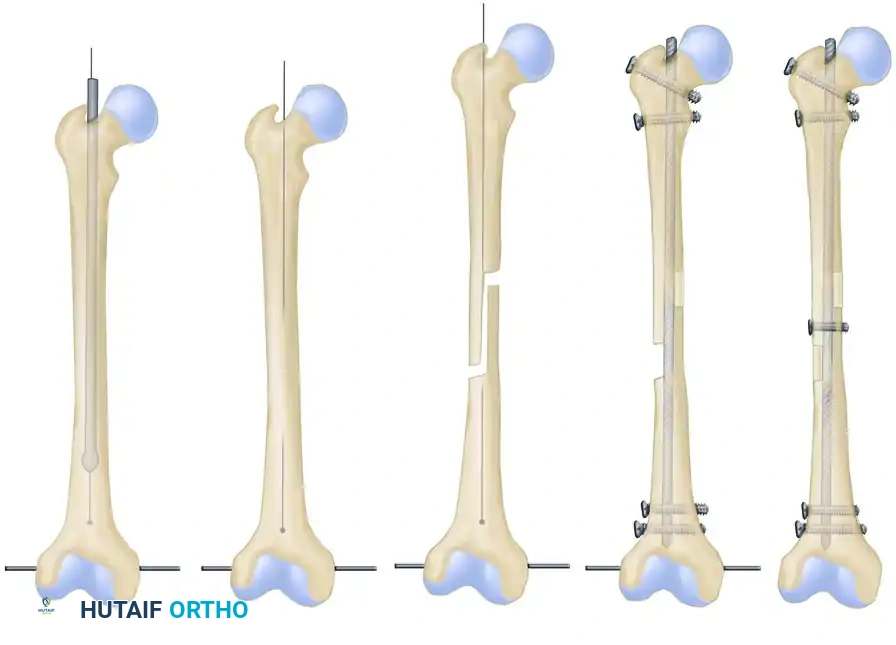
FIGURE 58-25: Schematic representation of a one-stage femoral lengthening procedure: Initial reaming, creation of a Z-shaped osteotomy, controlled lengthening, insertion of a static locked medullary nail, transverse locking screws, and application of autogenous bone grafts.
Two-Stage Corrections for Severe Deformity
For a severe deformity of long duration, an operation in two stages may be necessary to prevent neurovascular compromise.
1. Stage One: The malunion is broken up in an oblique plane via osteotomy. Length is gradually restored postoperatively using skeletal traction or, more commonly in modern practice, by external fixation distraction (Ilizarov or Taylor Spatial Frame).
2. Stage Two: Once satisfactory apposition, length, and alignment are obtained, the external fixator is removed. The fragments are then fixed internally with a rigid intramedullary nail or a large-fragment compression plate. Copious autogenous bone grafts (often harvested from the iliac crest or via Reamer-Irrigator-Aspirator) are placed around the osteotomy site, particularly medially and posteriorly, to stimulate osteogenesis.
COMPLICATIONS AND HARDWARE MANAGEMENT
Reported complications following the surgical correction of femoral malunions include femoral nerve palsies (typically from excessive or rapid traction), deep infection, nonunion, and loss of length due to hardware failure. When plates are utilized, complications can include plate avulsion, screw loosening, implant fracture, and persistent deformity.
Hardware Removal Challenges
Occasionally, internal fixation devices from the index surgery are fractured and deformed when the patient experiences a new injury or due to fatigue failure over a nonunion. This situation is frequently difficult because the deformed internal fixation device must be removed entirely before the new fracture or osteotomy can be definitively fixed. Broken intramedullary nails may require the use of specialized extraction hooks, over-reaming, or even a cortical window for retrieval. If not corrected acutely, retained hardware and persistent malalignments will inevitably cause intractable pain and progressive joint deformity.
CONCLUSION
The operative management of supracondylar and femoral shaft malunions requires a masterful blend of biomechanical knowledge, meticulous preoperative planning, and precise surgical execution. Whether employing a single-stage derotational intramedullary nail, a complex closing-wedge osteotomy with plate fixation, or a staged external-to-internal fixation protocol, the ultimate goal remains the same: restoration of the mechanical axis, equalization of limb length, and the return of pain-free, functional ambulation. Strict adherence to evidence-based indications and a deep respect for the soft tissue envelope will minimize complications and optimize patient outcomes in these challenging reconstructive cases.
You Might Also Like

