Femoral Shaft Fractures with Hip Dislocation: Comprehensive Surgical Guide
Key Takeaway
The combination of a femoral shaft fracture and hip dislocation is a high-energy orthopaedic emergency. Because the shaft fracture masks the clinical signs of dislocation, up to 50% of these injuries are initially missed. Prompt recognition via mandatory pelvic radiography and emergent hip reduction are critical to prevent femoral head osteonecrosis, followed by definitive intramedullary stabilization of the femoral shaft.
FRACTURE OF THE FEMORAL SHAFT WITH DISLOCATION OF THE HIP
The simultaneous occurrence of a femoral shaft fracture and an ipsilateral dislocation of the hip represents a complex, high-energy orthopaedic emergency. This combined injury pattern presents a profound diagnostic and therapeutic challenge. The discontinuity of the femoral diaphysis effectively eliminates the lever arm of the lower extremity, thereby masking the classic clinical presentation of a dislocated hip (shortening, internal rotation, and adduction). Consequently, a high index of suspicion and strict adherence to advanced trauma life support (ATLS) radiographic protocols are mandatory to prevent catastrophic delays in diagnosis.
Biomechanics and Mechanism of Injury
Historically, it was postulated that a single continuous force vector was responsible for producing both a fracture of the femoral neck or shaft and a concomitant hip dislocation. However, rigorous biomechanical investigations by Helal and Skevis have elucidated that this complex injury pattern is almost exclusively the result of two distinct, sequential forces acting upon the lower extremity.
In their cadaveric studies, Helal and Skevis demonstrated that the combination of a hip dislocation and a femoral shaft fracture could only be reliably reproduced under specific kinematic conditions:
* Force 1 (The Dislocating Vector): The hip is dislocated by a massive axial load applied directly in line with the femoral shaft while the knee and hip are flexed to 90 degrees and the hip is in a position of adduction (the classic "dashboard injury" mechanism).
* Force 2 (The Fracturing Vector): The femoral shaft is subsequently fractured by a secondary, independent force applied directly to the lateral aspect of the thigh.
The biomechanical reality of this two-force mechanism is strongly supported by the fracture morphology typically observed in these patients; the femoral shaft fracture is usually transverse, indicative of a direct, high-energy bending moment rather than a torsional force.
Clinical Evaluation and Radiographic Diagnosis
The most critical pitfall in the management of this combined injury is the failure to recognize the hip dislocation. Literature indicates that in up to 50% of all reported cases, the dislocation of the hip was unrecognized upon initial presentation. The fractured femoral shaft absorbs the deforming forces and prevents the distal limb from assuming the classic posture of a posterior hip dislocation.
CLINICAL PEARL: We maintain an absolute, unbreakable rule in trauma evaluation: In all fractures of the femoral shaft, an anteroposterior (AP) radiograph of the pelvis must be obtained. Since the universal institution of this protocol, the incidence of missed or delayed diagnosis of hip dislocations has plummeted.
Thorough systematic radiographic evaluation in the setting of high-energy trauma must include, at a minimum, orthogonal imaging of the joints adjacent to the anatomical area of primary injury. When evaluating the radiographs of a femoral shaft fracture, the position of the proximal fragment offers a critical diagnostic clue:
- The "Adduction Sign": Adduction of the proximal femoral fragment on the AP radiograph is strong evidence that the hip is dislocated. Because the femoral head is displaced posteriorly and medially out of the acetabulum, it tethers the proximal fragment in adduction.
- The Normal Abduction Vector: Helal and Skevis noted that in 85% of femoral shaft fractures without a dislocation of the hip, the proximal fragment is abducted due to the unopposed pull of the gluteus medius and minimus muscles inserting on the greater trochanter.
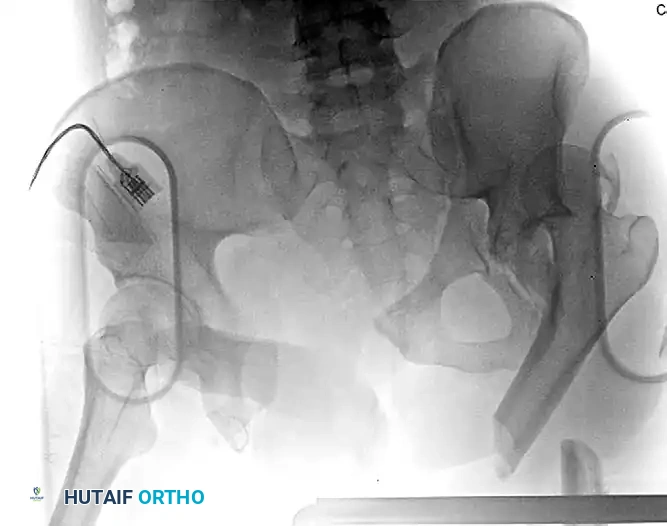
Figure 54-93 A: Polytraumatized patient with a left femoral diaphyseal fracture and an associated femoroacetabular dislocation. Note the concomitant complex pelvic ring and left-sided acetabular injury. The proximal femoral fragment is tethered in adduction, a hallmark radiographic sign of this combined injury.
Surgical Management and Reduction Techniques
In this combined injury, the dislocation of the hip is an absolute orthopaedic emergency. It must be reduced promptly to restore the vascular supply to the femoral head and mitigate the risk of osteonecrosis (avascular necrosis). The overarching goal is to achieve a concentric reduction of the hip joint as rapidly as possible, followed by definitive stabilization of the femoral shaft.
If the patient’s overall physiological condition permits early total care, we prefer to treat the femoral shaft fracture definitively in the same surgical setting immediately following hip reduction. However, the lack of a distal lever arm makes closed reduction of the hip exceptionally difficult. Several techniques have been described to overcome this mechanical disadvantage:
Technique 1: Percutaneous Pin-Assisted Reduction (Preferred)
To recreate a lever arm for hip reduction, a heavy Steinmann pin or a 5.0 mm Schanz pin is inserted percutaneously from anterior to posterior (or laterally) through the greater trochanter of the proximal fragment.
1. A large traction bow or T-handle is applied to the pin.
2. The surgeon uses the pin to apply direct longitudinal traction, flexion, and internal rotation to the proximal fragment.
3. Once the hip is concentrically reduced, the femoral shaft fracture can be treated definitively with antegrade or retrograde intramedullary fixation.

Figure 54-93 B: The proximal femur was reduced using a percutaneously positioned Schanz pin at the time of the patient’s exploratory laparotomy. The pin was subsequently incorporated into a uniplanar external fixator for temporary stabilization of the femoral fracture, dictated by the patient’s overall critical condition on presentation (Damage Control Orthopaedics).
Technique 2: Provisional Intramedullary Fixation
In this method, the patient is taken promptly to the operating room, and the femoral shaft fracture is rapidly stabilized using an intramedullary nail. The dislocation of the hip is momentarily disregarded until the diaphyseal fixation is complete.
1. Once the femur is rigidly nailed, the intact femur now serves as a robust lever arm.
2. Standard closed reduction maneuvers (e.g., Allis or Captain Morgan techniques) are then performed to reduce the hip.
SURGICAL WARNING: While this technique provides an excellent lever arm, it inherently delays the time to hip reduction by the duration of the nailing procedure. Therefore, this method should only be utilized if percutaneous pin-assisted closed reduction methods have been exhausted or if the nailing can be performed with extreme rapidity.
SUBTROCHANTERIC FRACTURES AND METASTATIC LESIONS
The subtrochanteric region of the femur is subjected to the highest biomechanical stresses in the human body. During normal weight-bearing, massive compressive forces are generated along the medial cortex, while significant tensile forces are exerted along the lateral cortex. This unique biomechanical environment makes the management of fractures in this region—whether traumatic or pathological—particularly demanding.
Pathological Fractures and Metastatic Disease
Metastatic lesions frequently localize in the highly vascularized subtrochanteric region and are often multicentric. These pathological fractures are notoriously slow to heal due to a combination of factors:
* Severe local bone loss secondary to osteolysis.
* Active tumor extension disrupting the osteogenic environment.
* The inhibitory effects of neoadjuvant or adjuvant radiation therapy on osteoblast function.
Because biological healing is compromised and delayed, the chosen orthopaedic implant must be capable of withstanding prolonged cyclical loading without fatigue failure. Intramedullary implants are exceptionally well-suited for the treatment of pathological processes because of their load-sharing biomechanics, which allow patients to tolerate immediate postoperative weight-bearing.
Modern cephalomedullary nails provide rigid, durable fixation of the entire femur, extending from the femoral neck down to the intercondylar notch. Rotation and length are meticulously maintained by the proximal reconstruction screws (into the femoral head) and distal interlocking screws.
Evidence-Based Outcomes:
In a landmark multicenter prospective study evaluating the efficacy of cephalomedullary fixation for metastatic disease, 25 metastatic femoral lesions in 22 patients were treated with the Russell-Taylor reconstruction nail.
* Pathological fractures had already occurred in 15 femurs, while 10 presented with impending pathological fractures (high Mirels' score).
* Twenty-four of the 25 lesions produced incapacitating preoperative pain. Following cephalomedullary nailing, profound pain relief was evident immediately after surgery in all patients.
* At an average 1-year follow-up, fixation had not been lost in any patient, and 16 of the 22 patients were still alive, demonstrating the implant's durability and its role in preserving quality of life in oncologic patients.
Subtrochanteric Fracture of the Femoral Shaft
Continuous improvements in interlocking intramedullary nail metallurgy and design have elevated cephalomedullary nailing to our treatment of choice for nearly all femoral shaft fractures extending from the lesser trochanter to the supracondylar region.
Implant Selection and Indications
- Standard Interlocking Nails: Suitable for mid-diaphyseal fractures.
- Cephalomedullary Nails: Mandatory for proximal fractures involving the lesser trochanter or subtrochanteric extension. These nails utilize proximal interlocking screws directed into the femoral head and neck, neutralizing the powerful deforming forces of the iliopsoas (flexion/external rotation) and abductors (abduction).
Managing Comminution and the Piriformis Fossa
Comminution involving the piriformis fossa presents a significant technical challenge for standard antegrade intramedullary nailing. If the starting point is compromised, the nail can propagate the fracture into the femoral neck or result in a catastrophic varus malreduction.
These challenges can be overcome if anatomical reduction of the major proximal head and neck fragment is strictly maintained with respect to the shaft during reaming and nail insertion. Alternatively, a trochanteric entry nail can be utilized to bypass a comminuted piriformis fossa.
While intramedullary nailing is the gold standard, Open Reduction and Internal Fixation (ORIF) utilizing fixed-angle plate and screw constructs (such as the 95-degree angled blade plate or proximal femoral locking plates) remains a viable primary treatment option, particularly in cases of severe proximal comminution where an intramedullary starting point cannot be safely established.
Step-by-Step Surgical Approach: Cephalomedullary Nailing
1. Patient Positioning and Preparation:
The patient is placed supine on a radiolucent fracture table. The operative leg is placed in traction with the hip flexed approximately 15 degrees and adducted to facilitate access to the proximal femur. The uninjured leg is scissored posteriorly or placed in a well-leg holder (hemilithotomy position) to allow unobstructed access for the C-arm fluoroscope.
2. Closed Reduction:
Prior to prepping, closed reduction is attempted using longitudinal traction and internal rotation. The reduction is confirmed via orthogonal fluoroscopic views. If the proximal fragment is flexed and abducted, percutaneous joysticks (Schanz pins) or a collinear reduction clamp may be required to neutralize the deforming muscle forces.
3. Incision and Entry Point:
A 3 to 5 cm longitudinal incision is made proximal to the greater trochanter. The fascia lata is split in line with its fibers.
* Piriformis Entry: The starting awl or guide pin is placed exactly in the piriformis fossa on the AP view and in line with the center of the femoral canal on the lateral view.
* Trochanteric Entry: The starting point is on the medial aspect of the greater trochanter tip.
4. Canal Preparation and Reaming:
A ball-tipped guide wire is passed across the fracture site and centered in the distal metaphysis. The canal is sequentially reamed over the guide wire. Reaming should be performed in 0.5 mm increments until cortical chatter is achieved, typically over-reaming by 1.0 to 1.5 mm larger than the selected nail diameter.
5. Nail Insertion and Proximal Locking:
The selected cephalomedullary nail is attached to the targeting jig and advanced manually into the canal. Aggressive hammering must be avoided to prevent iatrogenic comminution. Once the nail is seated at the correct depth (confirmed fluoroscopically), the proximal reconstruction guide pins are advanced into the femoral head. The pins should be positioned centrally in the femoral head on both AP and lateral views (Tip-Apex Distance < 25mm). The proximal screws are then drilled and inserted.
6. Distal Locking:
Distal locking is performed using a perfect circle technique under fluoroscopy. At least two distal locking screws are placed to control rotation and maintain length.
Postoperative Protocols and Rehabilitation
Postoperative management is dictated by the fracture pattern, the presence of concomitant injuries, and the rigidity of the fixation achieved.
- Weight-Bearing: For traumatic subtrochanteric fractures treated with a statically locked cephalomedullary nail, patients are typically allowed toe-touch or partial weight-bearing (up to 20 kg) for the first 6 weeks. Full weight-bearing is advanced once radiographic evidence of bridging callus is observed. For pathological fractures, immediate weight-bearing as tolerated is often permitted, as the implant is designed to load-share indefinitely.
- Physical Therapy: Early mobilization is critical. Active and active-assisted range of motion exercises for the hip and knee are initiated on postoperative day one. Strengthening of the hip abductors and quadriceps is emphasized to restore normal gait mechanics.
- Thromboembolic Prophylaxis: Due to the high-energy nature of the trauma and the proximity to the pelvic venous plexus, strict deep vein thrombosis (DVT) prophylaxis (e.g., low-molecular-weight heparin) is mandatory, typically continued for 28 to 35 days postoperatively.
- Follow-Up: Clinical and radiographic evaluations are conducted at 2 weeks, 6 weeks, 3 months, and 6 months to monitor fracture consolidation and implant integrity.
You Might Also Like


