Bioabsorbable Materials in Orthopaedic Surgery: Biomechanics, Biomaterials, and Clinical Application

Key Takeaway
Bioabsorbable materials, including polyglycolic acid (PGA) and polylactic acid (PLA), offer significant advantages in orthopaedic surgery by enabling gradual load transfer and eliminating hardware removal. However, their use requires a deep understanding of polymer biomechanics, degradation profiles, and potential complications such as aseptic osteolysis. This guide details the biochemical properties, surgical indications, and intraoperative handling techniques essential for optimizing clinical outcomes with bioabsorbable fixation devices.
BIOABSORBABLE MATERIALS IN ORTHOPAEDIC SURGERY
The evolution of orthopaedic fixation has increasingly embraced bioabsorbable materials, driven by the desire to eliminate secondary hardware removal surgeries, reduce stress shielding, and facilitate unhindered postoperative advanced imaging. Polyglycolic acid (PGA) was the first totally synthetic bioabsorbable suture developed, which paved the way for Vicryl—a copolymer consisting of 92% PGA and 8% polylactic acid (PLA)—and polydioxanone (PDS). PDS holds the historical distinction of being the first bioabsorbable material manufactured into orthopaedic screws.
Currently, the primary alpha polyesters utilized for bioabsorbable implants include PGA, PDS, polylevolactic acid (PLLA), and racemic poly(D, L)-lactic acid (PDLLA). While these materials offer the distinct advantage of gradual load transfer to healing tissue, their successful application demands a rigorous understanding of their degradation kinetics, biomechanical limitations, and potential for inciting adverse biological responses.
Biochemical Composition and Degradation Pathways
The degradation of bioabsorbable alpha polyesters occurs primarily through bulk hydrolysis, a process wherein water molecules cleave the ester bonds of the polymer backbone, leading to a progressive reduction in molecular weight, followed by a loss of mechanical strength, and ultimately, mass loss.
- Polyglycolic Acid (PGA): PGA is highly crystalline and hydrophilic, leading to rapid degradation. It is hydrolyzed primarily into pyruvic acid, which subsequently enters the tricarboxylic acid (TCA) cycle and is excreted physiologically as carbon dioxide (via respiration) and water.
- Polylactic Acid (PLA, PLLA, PDLLA): The addition of a methyl group makes PLA more hydrophobic than PGA, significantly slowing its degradation rate. PDLLA is hydrolyzed via the TCA cycle into carbon dioxide and water, excreted primarily by respiration. PLLA exhibits the slowest degradation profile of the alpha polyesters, maintaining its mechanical integrity for extended periods, which is highly advantageous for tissues requiring prolonged mechanical support.
- Polydioxanone (PDS): PDS is similarly hydrolyzed but is unique in that its degradation byproducts are primarily excreted in the urine rather than through respiration.
Clinical Pearl: The choice of bioabsorbable polymer must be meticulously matched to the expected healing time of the target tissue. Utilizing a rapidly degrading PGA implant for a slow-healing fracture may result in catastrophic fixation failure before clinical union is achieved.
Biomechanics and Material Properties
The biomechanical behavior of bioabsorbable polymers is fundamentally different from that of traditional metallic implants (e.g., titanium or stainless steel). Their properties are heavily influenced by chemical composition, manufacturing processes, physical dimensions, environmental factors, and time.
Glass Transition Temperature and Intraoperative Contouring
A critical limitation of biodegradable implants is their high glass transition temperature ($T_g$)—the specific temperature at which the amorphous regions of the polymer transition from a hard, glassy state to a softer, rubbery state. Because the $T_g$ of these polymers is well above human body temperature and standard operating room temperatures, biodegradable implants cannot be contoured or bent intraoperatively. Attempting to forcefully bend a bioabsorbable plate or pin at room temperature will result in brittle failure.
Self-Reinforcement Technology
To overcome the inherent mechanical weakness of raw polymers, manufacturers employ "self-reinforcement" techniques. By drawing the polymer through a die under specific thermal conditions, the internal polymer chains and fibers are oriented parallel to the longitudinal axis of the implant. This self-reinforcement (e.g., SR-PGA, SR-PLLA) dramatically increases the tensile and flexural strength of the device, making it suitable for load-bearing applications in orthopaedics.
Viscoelasticity: Creep and Stress Relaxation
Absorbable polymers are highly viscoelastic, making them subject to creep (progressive deformation under a constant load) and stress relaxation (decrease in stress under a constant strain).
Claes demonstrated that self-reinforced PLA (SR-PLA) and PDLLA-PLLA screws lost 20% of their compressive force within just 20 minutes of insertion. In a more natural, warm saline environment mimicking the human body, this loss of compressive force was even more rapid. Consequently, surgeons must be aware that the initial compression achieved across a fracture or osteotomy site will diminish rapidly in the immediate postoperative period.
Degradation Kinetics and Strength Loss
Because these implants are absorbable, they lose mechanical strength relatively rapidly compared to their mass loss.
* SR-PGA rods: Retain only 50% of their initial strength at 2 weeks, and a mere 13% at 4 weeks.
* PLLA: Exhibits the slowest degradation and loss of strength, making it the preferred material for interference screws in ligament reconstruction and anchors requiring prolonged pull-out strength.
Loading Modes and Stress-Strain Characteristics
Understanding how bioabsorbable implants respond to various physiological loading modes is essential for preventing premature mechanical failure. Implants may be subjected to tension, compression, bending, shear, torsion, or a combination of these forces.
When evaluating the material properties of these polymers, a single-cycle stress-strain curve is utilized. Testing is usually performed in a fixed sample with stress applied under tension. The curve delineates the elastic region (where deformation is reversible), the yield stress (the point of permanent plastic deformation), the ultimate stress (maximum load capacity), and the breaking stress (point of catastrophic failure). The modulus of elasticity (stiffness) of bioabsorbables is significantly closer to that of cortical and cancellous bone than metallic implants, which theoretically reduces stress shielding and promotes secondary bone healing.
Clinical Indications for Bioabsorbable Fixation
The most common orthopaedic application of bioabsorbable implants is for the attachment of soft tissue to bone, predominantly in shoulder (rotator cuff repair, labral repair) and knee surgeries (ACL/PCL reconstruction interference screws). However, their use in fracture fixation is expanding, particularly in scenarios where minimal load is applied until healing is evident.
Established Indications for Absorbable Fixation Devices:
* Foot and Ankle: Metatarsal osteotomies (e.g., hallux valgus correction), metacarpal and metatarsal fusions, malleolar fractures.
* Sports Medicine: Arthroscopic fixation of meniscus lesions, osteochondritis dissecans (OCD) fragment fixation, ruptures of the ulnar collateral ligament (UCL) of the thumb.
* Trauma and Pediatrics: Fractures of the radial head and olecranon, epiphyseal (physeal) fractures in children (where avoiding a second operation for hardware removal is highly desirable).
* Arthroplasty and Adjuncts: Femoral canal occlusion for cement restriction during total hip arthroplasty.
* Advanced Biologics: Drug delivery systems, cell transplantation matrices (e.g., Dermagraft), nerve reconstruction conduits (e.g., Neurotube), and adhesion prevention barriers.
Surgical Pitfall: Bioabsorbable bone implants currently should be strictly limited to applications where there is minimal load applied until healing is evident, such as periarticular fractures that are subsequently protected with rigid immobilization (cast or boot). They are contraindicated in diaphyseal fractures of major load-bearing long bones.
Surgical Technique and Intraoperative Handling
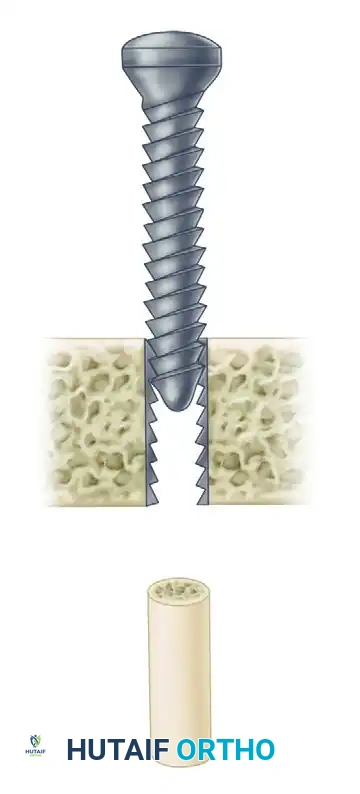
The surgical application of bioabsorbable screws and pins requires a meticulous technique that differs significantly from metallic hardware insertion. Failure to adhere to these principles often results in intraoperative implant breakage.
Step-by-Step Surgical Approach
- Anatomical Reduction: Achieve and provisionally hold absolute anatomical reduction using metallic K-wires or reduction forceps. Bioabsorbable implants cannot be used to "lag" or pull a poorly reduced fracture together with the same force as a metallic screw.
- Drilling: Drill the pilot hole using the exact drill bit specified by the manufacturer. Because bioabsorbables do not possess the cutting flutes of self-tapping metallic screws, the hole must be perfectly sized.
- Tapping (Crucial Step): The drill tract must be tapped through the entire depth of the planned screw insertion. Bioabsorbable screws cannot cut their own thread path in cortical bone; attempting to force them will result in the screw head shearing off.
- Insertion: Insert the screw using a specialized driver. Apply steady, axial pressure and turn slowly. Avoid high-torque, rapid insertion, which can cause frictional melting of the polymer or torsional failure of the screw shaft.
- Countersinking and Trimming: The head of the implant must be countersunk beneath the articular cartilage or flush with the cortical bone. Prominent bioabsorbable hardware is a primary catalyst for severe localized synovitis. If using pins, cut them flush with the bone surface using a hot wire or specialized cutting forceps to avoid leaving sharp, prominent edges.
Complications and Biological Responses
While bioabsorbable implants eliminate the need for hardware removal, their degradation process is not entirely benign. The body's response to the hydrolytic byproducts can lead to several well-documented complications.
Aseptic Inflammation and Osteolysis
PGA has been heavily implicated in aseptic inflammation and sterile sinus track formation. As the polymer rapidly degrades, the local clearance mechanisms (macrophages) can become overwhelmed by the acidic byproducts, leading to a localized drop in pH. This acidic environment can trigger a nonspecific foreign body reaction, resulting in osteolysis around the implant site.
Synovitis in Intra-articular Applications
Severe synovitis has been reported with the use of both PGA and PLLA bioabsorbable implants used to fix osteochondral lesions. This is believed to be a direct result of the volume of biodegradation debris shed into the joint space. Slower resorption of high-strength PLLA may mitigate, but does not entirely eliminate, this problem. If an implant breaks off into a joint space, the resulting loose body can cause rapid, severe arthropathy, often necessitating arthroscopic retrieval.
Infection and Fixation Failure Rates
Despite concerns regarding foreign body reactions, large-scale studies show favorable overall complication profiles. In a review of more than 2,500 fractures fixed with bioabsorbable implants:
* Bacterial wound infections: 3.6%
* Nonspecific foreign body reactions: 2.3%
* Failures of fixation: 3.7%
In a comparative study of 3,111 ankle fractures, infection was slightly less frequent with bioabsorbable fixation (3.2%) than with metallic fixation (4.1%). Furthermore, a prospective, randomized comparison of PLA screws versus stainless steel screws for displaced medial malleolar fractures found no statistically significant differences in operative or postoperative complications.
However, caution is warranted in specific anatomical regions. A report on absorbable plate-and-screw fixation for metacarpal fractures noted foreign body reactions in 4 out of 12 patients, all of whom required subsequent surgical débridement.
Postoperative Protocols and Radiographic Evaluation
Postoperative rehabilitation must account for the rapid loss of mechanical strength inherent to bioabsorbable polymers.
- Immobilization: Joints fixed with bioabsorbable implants typically require a longer period of rigid external immobilization (e.g., casting or bracing) compared to those fixed with metallic implants, protecting the construct during the critical 2-to-6-week window when polymer strength drops precipitously.
- Radiographic Evaluation: A major advantage of these implants is their radiolucency, which facilitates unobstructed postoperative radiographic, CT, and MRI evaluation of fracture healing and joint congruity.
- Bony Ingrowth: Surgeons must be aware that while bioabsorbable implants do dissolve, most are not replaced by bone. Postoperative CT scans of bones previously fixed with bioabsorbable implants frequently show empty, sclerotic tracts at the screw site long after the fractures have healed.
Future Horizons: Biologics and Drug Delivery
The future of bioabsorbable materials in orthopaedics extends far beyond simple mechanical fixation. Because these polymers can be engineered with specific degradation profiles, they are ideal candidates for use as delivery vehicles.
Currently, bioabsorbable implants are being heavily researched and utilized as carriers for Bone Morphogenetic Protein 2 (BMP-2) and other osteoinductive biochemicals. By embedding these proteins within the polymer matrix, the implant can provide a sustained, localized release of growth factors directly to the fracture site as it degrades. Additionally, their use in localized antibiotic delivery, cell transplantation, and nerve reconstruction conduits represents the cutting edge of orthopaedic biomaterial science, potentially making biochemical delivery the ultimate and most impactful application for this technology.
You Might Also Like