Surgical Management of Rheumatoid Extensor Mechanism Deformities: Lateral Band Mobilization and Boutonnière Correction
Key Takeaway
The surgical correction of rheumatoid hand deformities requires a profound understanding of extensor mechanism biomechanics. This guide details the Nalebuff and Millender technique for lateral band mobilization in swan-neck deformities, emphasizing strategic skin release and joint positioning. Furthermore, it provides a comprehensive classification and stage-based surgical approach to boutonnière deformities, ranging from soft-tissue reconstruction to proximal interphalangeal joint arthrodesis in severe, fixed contractures.
Introduction to Rheumatoid Extensor Mechanism Deformities
The rheumatoid hand presents a complex array of biomechanical challenges, primarily driven by chronic synovial hypertrophy, capsular distension, and subsequent attenuation of the delicate tendinous and ligamentous structures. Among the most debilitating manifestations are deformities of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints, specifically the swan-neck and boutonnière deformities.
Successful surgical intervention requires a masterful understanding of the digital extensor mechanism—a highly sophisticated, interconnected network comprising the central slip, lateral bands, transverse retinacular ligaments, and the oblique retinacular ligament (ORL). This comprehensive guide details the precise surgical techniques for addressing these imbalances, focusing on the Nalebuff and Millender lateral band mobilization for swan-neck deformities and the stage-based management of the boutonnière deformity.
Lateral Band Mobilization and Skin Release (Nalebuff and Millender)
The swan-neck deformity is characterized by PIP joint hyperextension and DIP joint flexion. In the rheumatoid patient, this is frequently initiated by terminal tendon rupture or stretching, PIP joint synovitis, or intrinsic tightness. As the deformity progresses, the transverse retinacular ligaments attenuate, allowing the lateral bands to subluxate dorsally. They become fixed dorsal to the axis of rotation of the PIP joint, acting as powerful PIP hyperextensors.
The Nalebuff and Millender technique is a highly effective soft-tissue procedure designed to mobilize these dorsally fixed lateral bands, allowing them to return to their anatomical position volar to the PIP joint axis during flexion, while simultaneously addressing the contracted dorsal skin.
Preoperative Evaluation
Before embarking on lateral band mobilization, the surgeon must meticulously evaluate the integrity and function of the flexor apparatus.
Clinical Pearl: Flexor Tendon Assessment
Ensure in the preoperative evaluation that active motion can be established by evaluating active flexion of the joint by the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) tendons. If active flexor function is not confirmed clinically, intraoperative assessment is mandatory. Make an incision in the palm and apply traction to the flexor tendons to confirm they are not adherent or tethered by rheumatoid nodules within the flexor sheath.
Surgical Technique: Step-by-Step
1. Incision and Exposure
The surgical approach is critical, as the dorsal skin in a chronic swan-neck deformity is often severely contracted.
* Begin with a slightly curved dorsal incision at the midportion of the proximal phalanx.
* Continue the incision distally over the dorsolateral aspect of the PIP joint.
* Extend it over the middle of the middle phalanx, traversing obliquely and dorsally to form the "tail of a J".
Figure 1: Nalebuff and Millender technique for correction of swan-neck deformity. The skin incision is shown curved to permit the release of contracted skin.
2. Flap Elevation
* Elevate the skin flaps with extreme care. In the rheumatoid patient, the skin is often thin and fragile.
* Ensure that the dorsal venous drainage is preserved by taking the veins with the elevated skin flaps. This minimizes postoperative edema and prevents flap necrosis.
3. Lateral Band Release
The core of the procedure is the release of the lateral bands from their abnormal dorsal position.
* Identify the central tendon and the dorsally displaced lateral bands.
* Make a longitudinal incision between each lateral band and the central tendon.
* This precise tenotomy releases the lateral bands from their fixed dorsal position, freeing them from the attenuated triangular ligament and dorsal capsular adhesions.
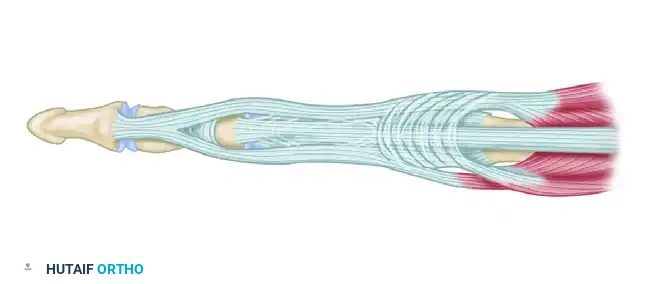
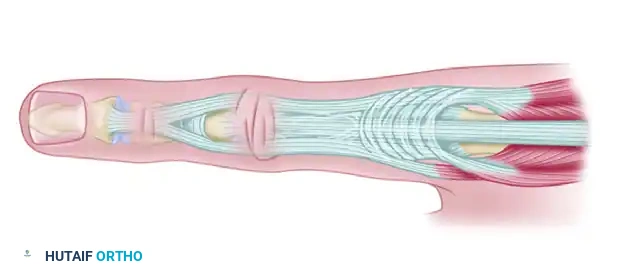
Figure 2: Longitudinal releasing incisions are made between the lateral bands and the central slip.
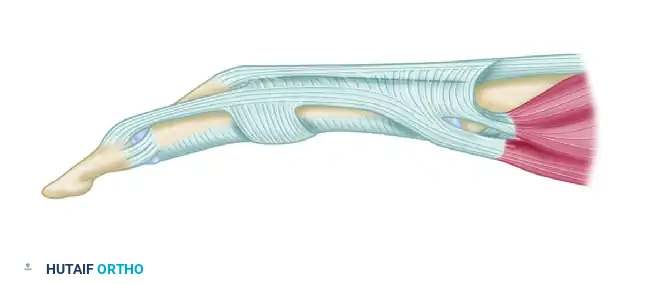
Figure 3: The lateral tendons are fully mobilized from their fixed dorsal position.
4. Dynamic Intraoperative Assessment
* Passively flex the PIP joint.
* Observe the biomechanical shift: the lateral bands should now slip volarward, sliding smoothly over the condyles of the PIP joint.
* If the bands do not subluxate volarward, further release of the dorsal adhesions or the triangular ligament may be required.
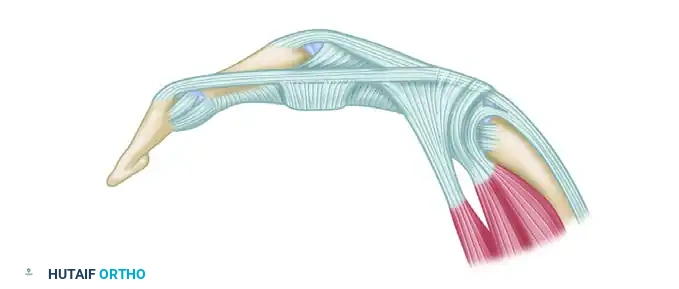
Figure 4: The joint is flexed, demonstrating the volar translation of the mobilized lateral bands across the condylar axis.
5. Synovectomy
* With the extensor mechanism mobilized, excellent exposure of the PIP joint is achieved.
* Perform a meticulous PIP joint synovectomy. Good passive motion is usually established at this stage unless there is a bulging, obstructive synovitis of the flexor tendons within the sheath, which would necessitate a separate volar approach for flexor tenosynovectomy.
6. Strategic Skin Closure
* Suture the skin incision proximally using non-absorbable monofilament (e.g., 5-0 nylon).
* Crucial Step: Distally, suturing may not be possible, nor is it desirable. The distal incision, being placed obliquely across the middle phalanx, will gape open when the finger is flexed. This gaping accomplishes a necessary skin release.
Surgical Warning: Avoid Routine Closure
If the distal portion of the skin incision is sutured routinely under tension, it will act as a dorsal tether and directly contribute to the recurrence of the PIP joint hyperextension deformity. The open portion of the incision usually heals by secondary intention without a skin graft in approximately 2 weeks.
7. Postoperative Fixation
* Pass a smooth 0.035-inch or 0.045-inch Kirschner wire (K-wire) obliquely across the PIP joint to maintain the joint in approximately 20 to 30 degrees of flexion.
* This pin is left in place postoperatively for approximately 3 weeks. During this immobilization period, the open portion of the skin wound will granulate and close, and the lateral bands will scar into their new, biomechanically advantageous position.
Buttonhole, or Boutonnière, Deformity
In stark contrast to the swan-neck deformity, a finger with a buttonhole (boutonnière) deformity presents with a flexed PIP joint and a hyperextended DIP joint. While it can result from acute trauma (e.g., central slip avulsion), it is most commonly seen in patients with rheumatoid arthritis as a progressive, insidious collapse of the extensor mechanism.
Pathoanatomy and Biomechanics
In the rheumatoid patient, the boutonnière deformity is initiated by primary synovitis of the PIP joint.
1. Capsular Distension: The hypertrophic synovium distends the dorsal capsule, stretching and attenuating the overlying central slip of the extensor tendon.
2. Lateral Band Subluxation: As the central slip loses its mechanical integrity, the lateral bands are no longer held dorsally. They begin subluxating volarward, slipping below the axis of rotation of the PIP joint.
3. Biomechanical Reversal: Once the lateral bands cross the mid-axial line, they cease to be PIP joint extensors and become paradoxical PIP joint flexors.
4. Secondary Contractures: As the deformity progresses, the lateral bands become tightened by their new shortened course and by pressure from the underlying swollen joint. The transverse retinacular ligaments contract, fixing the bands in this volar position.
5. DIP Hyperextension: The increased tension on the lateral bands and the contraction of the oblique retinacular ligament (ORL)—which originates from the flexor sheath and inserts into the dorsal base of the distal phalanx—lead to a secondary, rigid hyperextension deformity of the DIP joint.
6. MCP Joint Compensation: The flexion deformity of the PIP joint is often compensated for by an extension posture of the metacarpophalangeal (MCP) joint. Unlike the distal two joints, this MCP joint deformity usually does not become fixed.
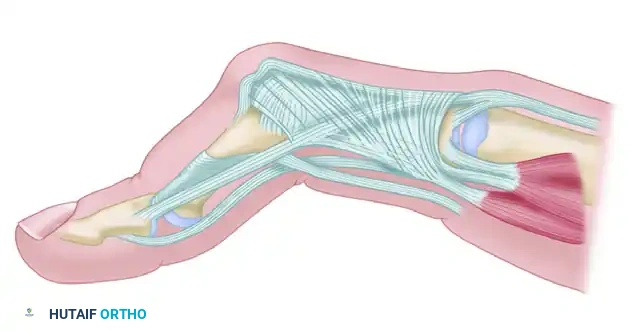
Figure 5: Pathoanatomy of the Boutonnière deformity. Primary synovitis of the PIP joint leads to attenuation of the central slip. The lateral bands subluxate volar to the axis of rotation, and contraction of the oblique retinacular ligament leads to DIP hyperextension.
Clinical Presentation
Patients present with the classic posture: PIP flexion and DIP hyperextension. Functionally, this severely impairs the ability to grasp large objects and perform fine pinch maneuvers, as the fingertip cannot be brought into flexion.
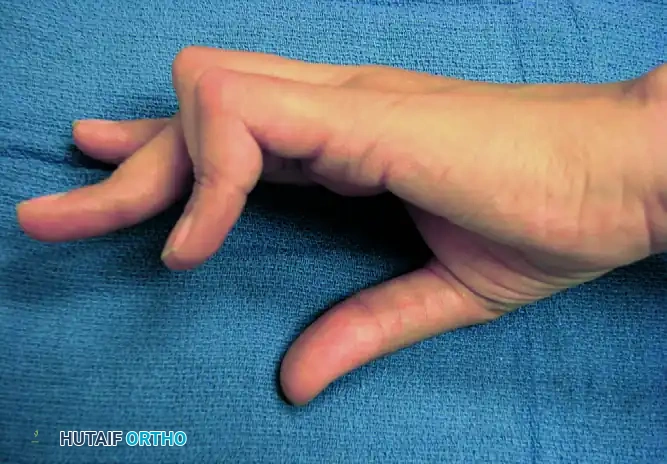
Figure 6: Clinical photograph illustrating the severe flexion posture of the PIP joints and hyperextension of the DIP joints in a rheumatoid patient.
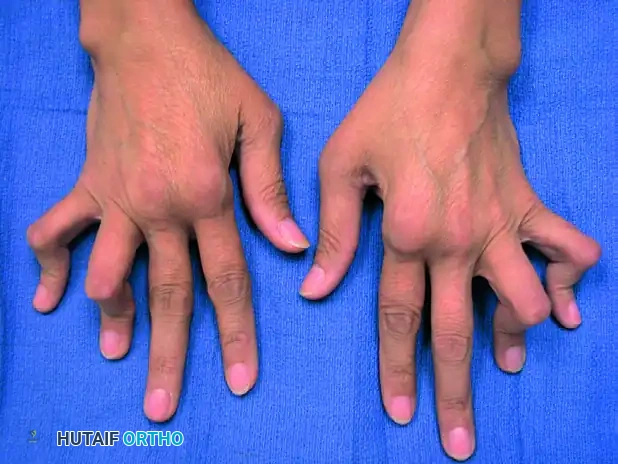
Figure 7: Lateral clinical view demonstrating the classic boutonnière cascade, highlighting the compensatory MCP extension.
Classification and Stage-Based Management
Nalebuff and Millender categorized boutonnière deformities based on three critical factors:
1. The radiographic appearance of the joint surface (cartilage preservation vs. destruction).
2. The amount of active and passive PIP joint motion.
3. The degree of fixed contracture.
1. Mild Boutonnière Deformity
- Characteristics: There is a mild flexion deformity at the PIP joint (approximately 10 to 15 degrees) with a lessened ability to fully flex the DIP joint. The DIP joint is not yet fixed in hyperextension. Crucially, the PIP flexion deformity is passively correctable to neutral. Radiographs show preserved joint spaces.
- Treatment: Management is primarily soft-tissue balancing. Treatment consists of releasing the lateral tendons near their insertion into the distal phalanx to correct the DIP hyperextension. A PIP joint synovectomy is performed. An extensor tenotomy over the middle phalanx (the Dolphin-Fowler procedure) can be utilized to redirect extensor force to the PIP joint while allowing the DIP joint to flex.
2. Moderate Boutonnière Deformity
- Characteristics: The finger presents with an approximately 40-degree PIP joint flexion contracture. Most of this contracture remains passively correctable. The distal joint is hyperextended, and the MCP joint is correctable to full flexion passively. The lateral bands are fixed in their subluxated volar position due to the contracted transverse retinacular ligament. Radiographs show no severe joint destruction.
- Treatment: To correct this deformity, the surgeon must achieve functional restoration of the central slip and correction of the lateral band subluxation.
- A dorsal approach is used.
- The contracted transverse retinacular ligaments are released longitudinally to allow the lateral bands to be mobilized dorsally.
- Central slip reconstruction is performed. This can be achieved by mobilizing and suturing the lateral bands together over the dorsum of the PIP joint, or by utilizing a free tendon graft (e.g., palmaris longus) to bridge the central slip defect.
- Postoperatively, the PIP joint is pinned in extension for 3 to 4 weeks.
3. Severe Boutonnière Deformity
- Characteristics: The PIP joint is stiff, and the flexion contracture is no longer passively correctable. Radiographs demonstrate significant joint space narrowing, cartilage destruction, and erosive changes typical of advanced rheumatoid arthritis.
- Treatment: Soft-tissue reconstruction alone will fail in the presence of a destroyed, stiff joint.
- Long, Ring, and Little Fingers: These digits require a functional arc of motion for grip strength. Therefore, treatment typically involves extensor mechanism reconstruction combined with PIP joint implant arthroplasty (e.g., silicone elastomer implants).
- Index Finger: The index finger PIP joint is subjected to significant lateral pinch forces. Implant arthroplasty in the index finger has a high rate of failure and instability. Therefore, arthrodesis of the PIP joint in a functional position (approximately 25 to 30 degrees of flexion) is a more durable and reliable procedure.
4. Fixed Boutonnière Deformity
- Characteristics: A fixed buttonhole deformity exhibits severe joint changes on radiographs and a passively uncorrectable PIP joint flexion contracture that cannot be mobilized even under anesthesia.
- Treatment: Kiefhaber and Strickland extensively evaluated outcomes in these advanced stages. They found that central extensor tendon reconstruction for severe, fixed rheumatoid boutonnière deformities is highly unpredictable and prone to recurrence. Consequently, they strongly recommended PIP joint arthrodesis as the definitive treatment for severe, fixed boutonnière deformities across all digits, ensuring a stable, pain-free finger, albeit at the cost of PIP motion.
Postoperative Rehabilitation Protocol
Regardless of the stage, postoperative rehabilitation is paramount to the success of boutonnière correction.
* Immobilization Phase: Following soft-tissue reconstruction, the PIP joint is typically immobilized in full extension (often with a transarticular K-wire) for 3 to 4 weeks to protect the central slip repair. During this time, active and passive DIP joint flexion exercises are encouraged to stretch the ORL and prevent recurrent DIP hyperextension.
* Mobilization Phase: Once the K-wire is removed, a dynamic extension splint (e.g., a Capener splint) is utilized during the day to support the PIP joint while allowing active flexion. Night splinting in full extension is continued for an additional 6 to 8 weeks to prevent flexion contracture recurrence.
Clinical Pearl: Managing Patient Expectations
Rheumatoid extensor mechanism reconstructions are salvage procedures. The primary goals are to relieve pain, improve the functional cascade of the hand, and prevent further deformity progression. Patients must be counseled preoperatively that achieving a completely "normal" finger with full, unrestricted range of motion is highly unlikely, and that rigorous adherence to postoperative hand therapy is non-negotiable.
📚 Medical References
- boutonnière deformity, J Bone Joint Surg 49A:1267, 1967.
- Lucas GL: Fowler central slip tenotomy for old mallet deformity, Plast Reconstr Surg 80:92, 1987.
- McCoy FJ, Winsky AJ: Lumbrical loop operation for luxation of the extensor tendons of the hand, Plast Reconstr Surg 44:142, 1969.
- Minamikawa Y, Peimer CA, Yamaguchi T, et al: Wrist position and extensor tendon amplitude following repair, J Hand Surg 17A:268, 1992.
- Mowlavi A, Burns M, Brown RE: Dynamic versus static splinting of simple zone V and zone VI extensor tendon repairs: a prospective, randomized, controlled study, Plast Reconstr Surg 115:482, 2005.
- Nakamura S, Katsuki M: Tendon grafting for multiple extensor tendon ruptures of fi ngers in rheumatoid hands, J Hand Surg 27B:326, 2002.
- Newport ML, Pollack GR, Williams CD: Biomechanical characteristics of suture techniques in extensor zone IV, J Hand Surg 20A:650, 1995.
- Newport ML, Shukla A: Electrophysiologic basis of dynamic extensor splinting, J Hand Surg 17A:272, 1992.
- Newport ML, Williams CD: Biomechanical characteristics of extensor tendon suture techniques, J Hand Surg 17A:1117, 1992.
- Noorda RJ, Hage JJ, de Groot PJ, et al:
You Might Also Like