Operative Management of the Rheumatoid Forefoot: A Comprehensive Guide
Key Takeaway
Rheumatoid arthritis of the forefoot presents with progressive metatarsophalangeal joint synovitis, leading to capsular distention, ligamentous failure, and severe dorsal subluxation. This comprehensive guide details the biomechanical collapse, nonoperative management, and step-by-step surgical reconstruction techniques. Emphasizing meticulous preoperative vascular assessment and precise osteotomies, it provides orthopaedic surgeons with evidence-based protocols to restore plantigrade alignment, alleviate intractable pain, and manage complex multi-planar deformities effectively.
Introduction to Rheumatoid Forefoot Deformities
The forefoot is frequently the initial site of clinical manifestation in rheumatoid arthritis (RA). The earliest pathologic hallmark is aggressive synovitis of the metatarsophalangeal (MTP) joints. Concomitant with this synovial hypertrophy is the localized release of destructive enzymes—specifically matrix metalloproteinases (MMPs), proteases, and collagenases—from the diseased synovium. These enzymes systematically degrade articular cartilage and disrupt critical ligament-bone interphases, leading to profound biomechanical instability.
As the joint capsule undergoes fluid distention and the capsular ligaments weaken, the delicate balance of the forefoot is lost. During the propulsive phase of weight-bearing, the proximal phalanges begin to subluxate dorsally on the metatarsal heads. This initiates a cascade of progressive, multi-planar deformities that severely compromise patient mobility and quality of life.
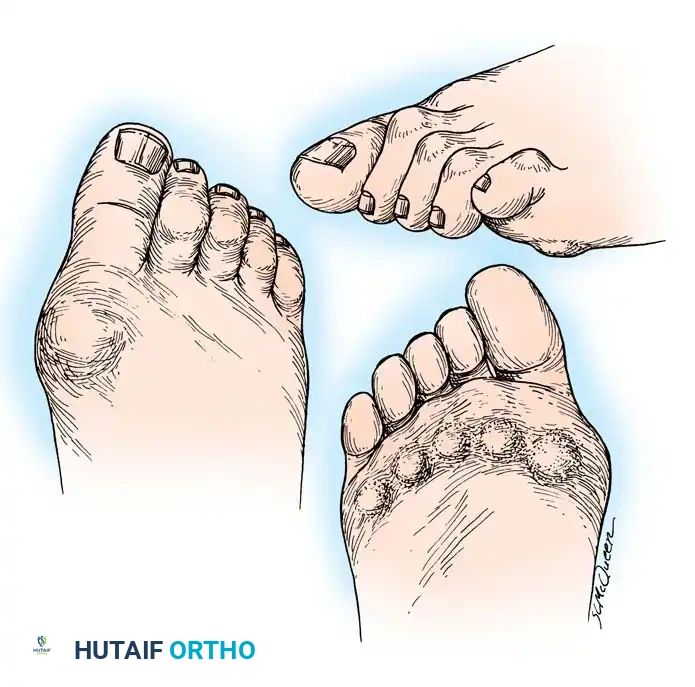
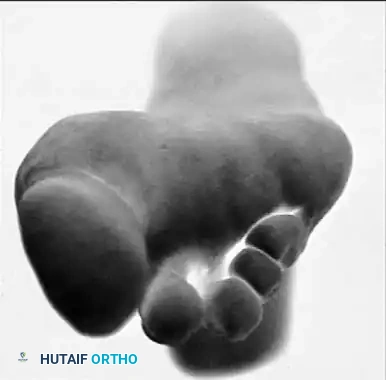
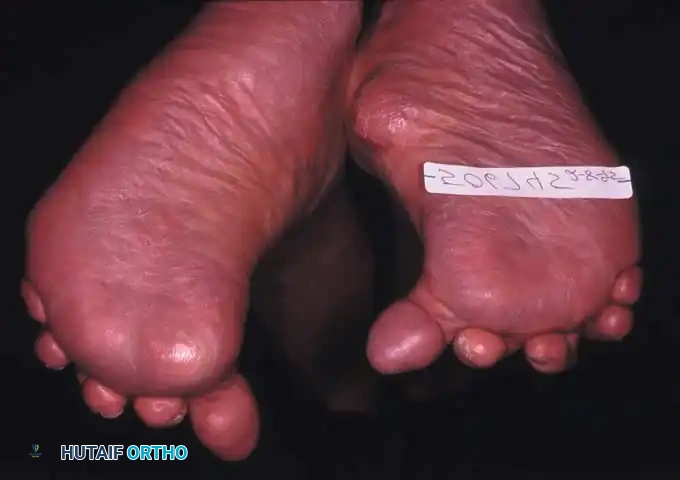
Fig. 81-1 Rheumatoid foot. Note the multiple severe deformities characteristic of rheumatoid arthritis of the forefoot, including advanced hallux valgus, subluxed and dislocated lesser metatarsophalangeal joints, claw toes, hammer toes, and prominent bursal formation.
Biomechanics of Forefoot Collapse
Understanding the biomechanical collapse of the rheumatoid forefoot is essential for effective surgical reconstruction. The deformity is driven by a predictable sequence of intrinsic and extrinsic muscle imbalances:
- Intrinsic Muscle Dysfunction: As the MTP joints subluxate dorsally, the intrinsic muscles (lumbricals and interossei) shift dorsal to the flexion-extension axis of the MTP joints. Consequently, they lose their primary ability to flex the MTP joint. Furthermore, their secondary function—extending the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints—is severely weakened.
- Extrinsic Overpowering (Tenodesis Effect): With the intrinsics mechanically disadvantaged, the extrinsic long toe flexors (flexor hallucis longus and flexor digitorum longus) exert an unopposed pull, drawing the PIP and DIP joints into rigid flexion.
- Extensor Mechanism Concentration: The inability of the extensor digitorum brevis (EDB) and extensor digitorum longus (EDL) to extend the middle and distal joints compounds the deformity. Because of reduced tendon excursion secondary to MTP joint hyperextension, all the extension moment of the extensor hallucis longus (EHL), extensor hallucis brevis (EHB), EDL, and EDB is concentrated entirely at the MTP joints.
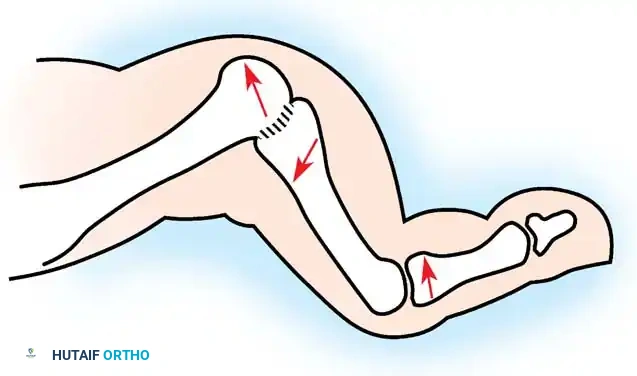
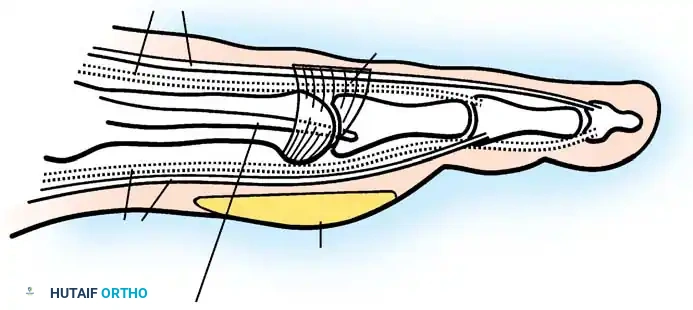
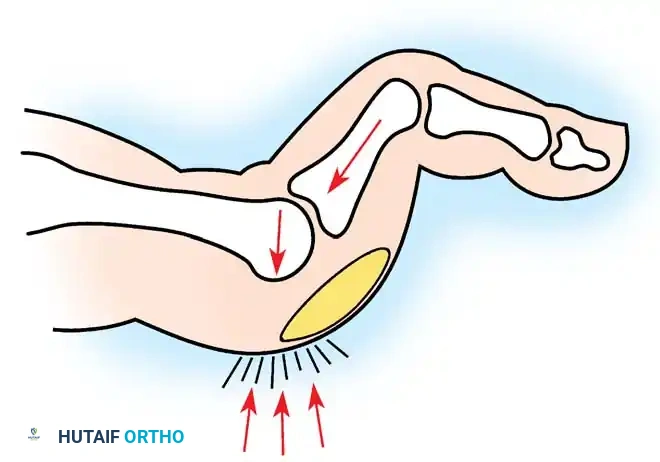
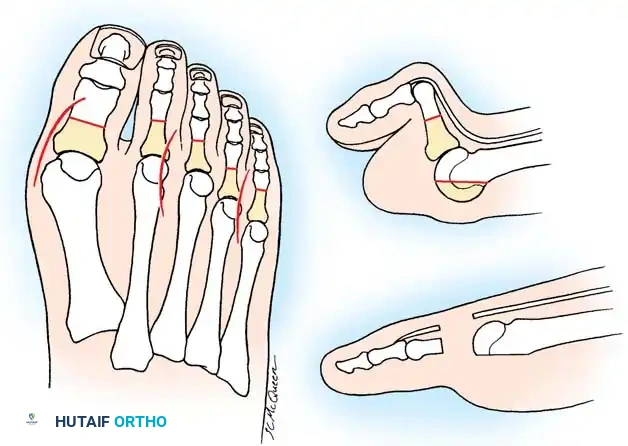
Fig. 81-7 Biomechanical progression. (A) Normal alignment and balance of the MTP joints and extensor sling. (B) Progressive dorsal subluxation and lesser toe deformity. (C) End-stage deformity with complete MTP dislocation; the proximal phalanx is ankylosed to the dorsal aspect of the metatarsal head, and the plantar fat pad has migrated distally.
Gradually, this concentrated extension force completely dislocates the MTP joints. At end-stage disease, the proximal phalanx rests entirely on the dorsal aspect of the metatarsal neck.
Clinical Evaluation and Deformity Progression
The hyperextension and eventual dislocation of the MTP joints yield several clinically significant and highly symptomatic deformities:
- Distal Migration of the Plantar Fat Pad: As the proximal phalanx dislocates dorsally, it drags the plantar aponeurosis and the protective plantar fat pad distally.
- Intractable Plantar Keratoses (IPKs): The metatarsal heads are left completely uncovered and prominent against the plantar skin, leading to painful callosities and a high risk of skin ulceration.
- Digital Contractures: Fixed flexion contractures of the PIP and DIP joints (claw toes) and the interphalangeal joint of the hallux develop.
- Dorsal Prominences: Painful hard corns form over the dorsum of the PIP joints, and end corns develop at the nail-pulp junction due to abnormal weight-bearing on the toe tips.


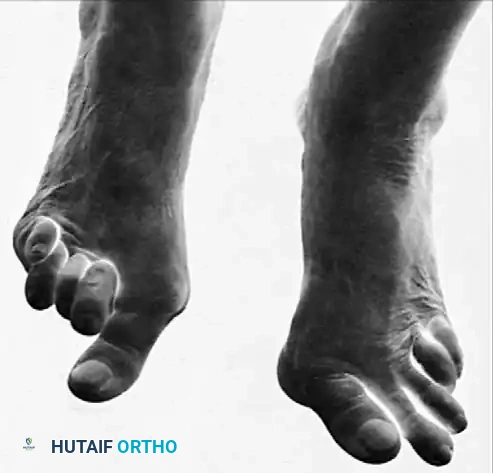
Fig. 81-4 Multiple deformities of rheumatoid arthritis. Note the prominent bursa directly over the medial eminence and the severe dorsal posturing of the lesser digits.
Clinical Pearl: While isolated hammer toes can occur without MTP joint synovitis, their isolated occurrence is exceedingly rare in rheumatoid arthritis. Conversely, in seronegative spondyloarthropathies (e.g., psoriatic arthritis), destructive arthritic deformity of the PIP joints resulting in isolated hammer toes is common and may present without significant MTP joint involvement.
Epidemiological data strongly supports the prevalence of these deformities. Vidigal et al. evaluated 104 patients with RA and noted that 77% exhibited lesser MTP joint subluxation, with 30% developing pressure lesions secondary to hammer toes. Furthermore, hallux valgus deformity was present in 70% of these patients, often accompanied by a varus deformity of the fifth digit.


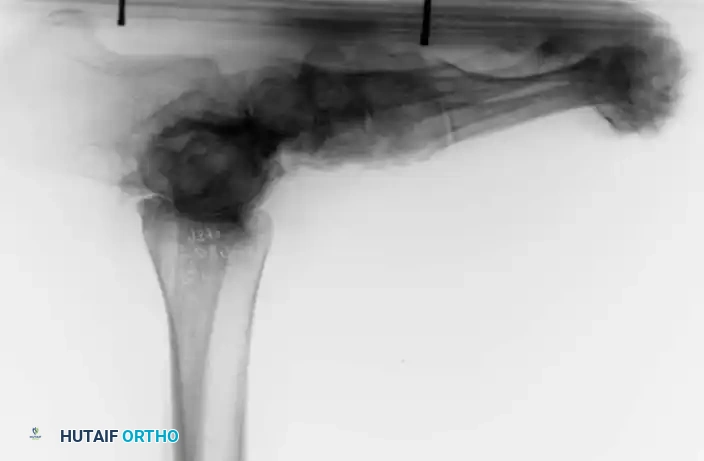
Fig. 81-6 (A) Heel valgus and foot pronation secondary to RA. If the subtalar and midtarsal joints are surgically reduced, the forefoot may be in pronounced supination relative to the hindfoot, complicating first ray plantarflexion. (B) Radiographic evidence of multiple severe dislocations of the MTP joints.
Nonoperative Management Strategies
Initial management of the rheumatoid forefoot is strictly nonoperative, focusing on accommodating the deformity, reducing pressure over bony prominences, and alleviating pain.
- Footwear Modifications: Patients should be fitted with extra-deep shoes featuring a wide, high toe box to accommodate dorsal digital deformities.
- Orthoses: A custom-molded insert with relief for prominent metatarsal heads is essential. Chalmers et al. demonstrated that semirigid orthoses are significantly more effective than soft orthoses in providing symptomatic relief. Early implementation is highly recommended.
- Shoe Alterations: Rocker-bottom soles and rigid steel shanks can effectively relieve midfoot pain by reducing the bending moment across the forefoot during the terminal stance phase of gait.
- Ancillary Care: Toe sleeves, silicone spacers, corn pads, and routine podiatric debridement of plantar callosities provide valuable symptomatic relief.
- Bracing: If concomitant tibiotalar or hindfoot involvement is present, a double upright brace with a limited-motion or locked ankle joint and an inside (valgus-correcting) T-strap may aid in comprehensive nonoperative management.
While these conservative measures can be utilized indefinitely, surgical intervention is frequently required due to progressive pain, worsening deformity, recurrent ulcerations, and patient dissatisfaction with increasingly cumbersome footwear modifications.
Preoperative Planning and Optimization
Before recommending forefoot arthroplasty, the surgeon must engage in thorough patient counseling. The patient must explicitly understand that rheumatoid arthritis is a progressive systemic disease; therefore, surgical correction is primarily palliative, aiming to restore a plantigrade, braceable foot rather than offering a definitive "cure."
Systemic and Local Evaluation
Complications in rheumatoid forefoot surgery can be catastrophic but are largely preventable if strict preoperative protocols are followed:
- Vascular Assessment: Meticulous evaluation of pedal pulses is mandatory. If asymmetry or diminution is noted, a peripheral vascular consultation is required. In nondiabetic RA patients, an absolute ankle pressure of $\ge 90$ mm Hg or an Ankle-Brachial Index (ABI) of $\ge 0.7$ generally predicts successful forefoot wound healing in 90% of cases.
- Rheumatoid Vasculitis: Carefully inspect the skin of the foot and distal leg. Rheumatoid vasculitis presents as slightly raised macules and papules (often over the anterolateral distal tibia or dorsolateral foot) that do not blanch with pressure and may feature a necrotic preulcerative center.
- Neurologic Evaluation: Mononeuritis multiplex, resulting from immune complex–mediated vasculitis of the vasa nervorum, can cause hyperesthesia or impaired sensation. If vasculitis is suspected, rheumatology consultation or skin biopsy is warranted prior to any elective reconstruction.
- Medication Management: Historically, disease-modifying antirheumatic drugs (DMARDs) were stopped perioperatively. However, contemporary evidence (Bibbo et al.) indicates that the perioperative continuation of methotrexate, gold therapy, NSAIDs, low-dose corticosteroids, or hydroxychloroquine does not significantly increase postoperative healing complications or infection rates.
Surgical Warning: Patients on chronic corticosteroid therapy possess fragile, atrophic skin. Sutures should be left in place for a minimum of 3 to 4 weeks, rather than the customary 12 to 14 days, to prevent wound dehiscence.
Operative Techniques: Forefoot Reconstruction
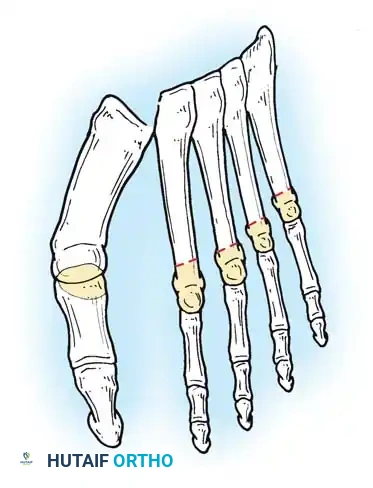
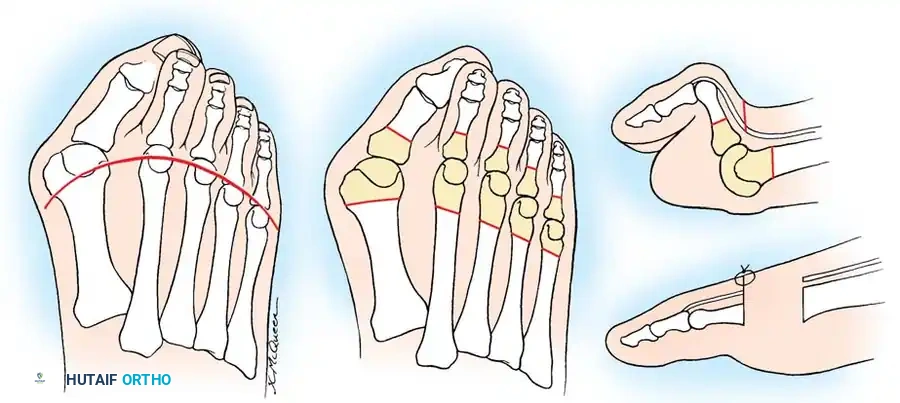
The gold standard for the severely deformed rheumatoid forefoot is Arthrodesis of the First MTP Joint combined with Resection Arthroplasty of the Lesser Metatarsal Heads (often referred to as the modified Hoffman-Clayton procedure).



Surgical Diagrams demonstrating the principles of first MTP arthrodesis and lesser metatarsal head resection to restore a functional, plantigrade forefoot cascade.
Step 1: Preparation and Positioning
- Skin Prep: Meticulous skin preparation is critical. The foot, especially the interdigital web spaces and periungual folds, should be scrubbed for 10 to 15 minutes preoperatively and wrapped in a sterile towel. This is repeated in the operating suite.
- Antibiotics: Prophylactic broad-spectrum intravenous antibiotics must be administered 30 minutes prior to tourniquet inflation and continued for 24 to 48 hours postoperatively.
- Positioning: The patient is placed supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position. A calf or thigh tourniquet is applied.
Step 2: First MTP Joint Arthrodesis
Arthrodesis of the first ray provides a stable medial column, which is essential for offloading the lesser metatarsals and preventing recurrent lateral deformity.
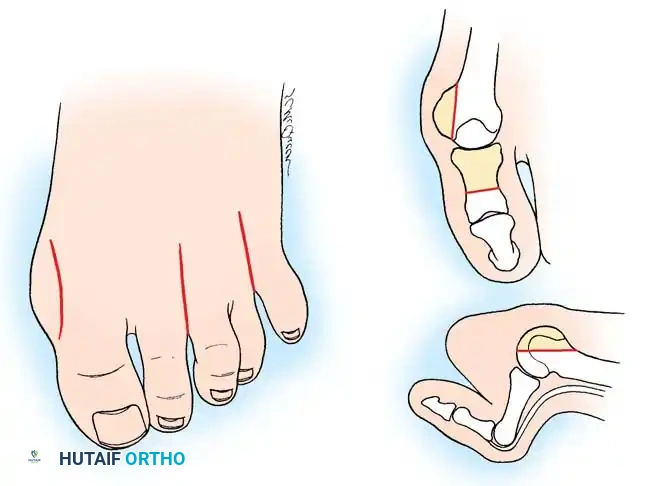
1. Approach: A dorsal longitudinal incision is made medial to the EHL tendon, extending from the mid-shaft of the first metatarsal to the interphalangeal joint.
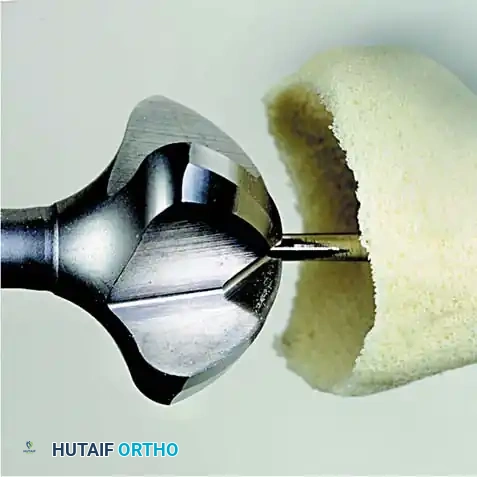
2. Joint Preparation: The capsule is incised, and the collateral ligaments are released. The severely eroded articular surfaces of the first metatarsal head and the base of the proximal phalanx are resected. Cup-and-cone reamers are highly recommended to preserve length while allowing multi-planar adjustment.
3. Positioning: The hallux is positioned in 10 to 15 degrees of valgus and 15 to 20 degrees of dorsiflexion relative to the first metatarsal shaft. Neutral rotation must be confirmed to ensure the toenail faces directly dorsal.
4. Fixation: Rigid internal fixation is achieved using a dorsal contoured titanium plate and a lag screw across the arthrodesis site.


Fig. 81-2 (A, B) Preoperative clinical views showing severe dorsal subluxation-dislocation of lesser toes. (C) Plantar view post-resection of metatarsal heads. (D) Excellent postoperative clinical alignment following first MTP arthrodesis and lesser metatarsal head excision.
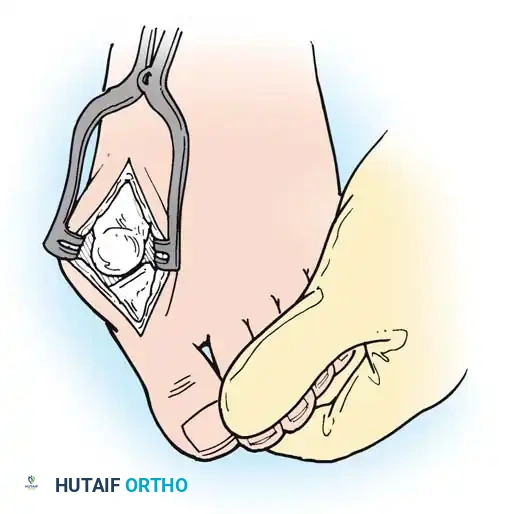
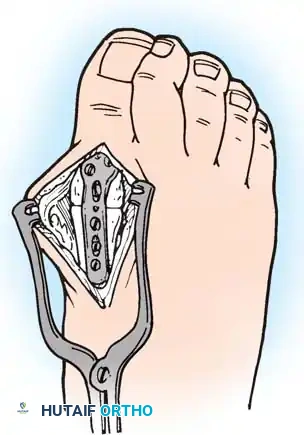
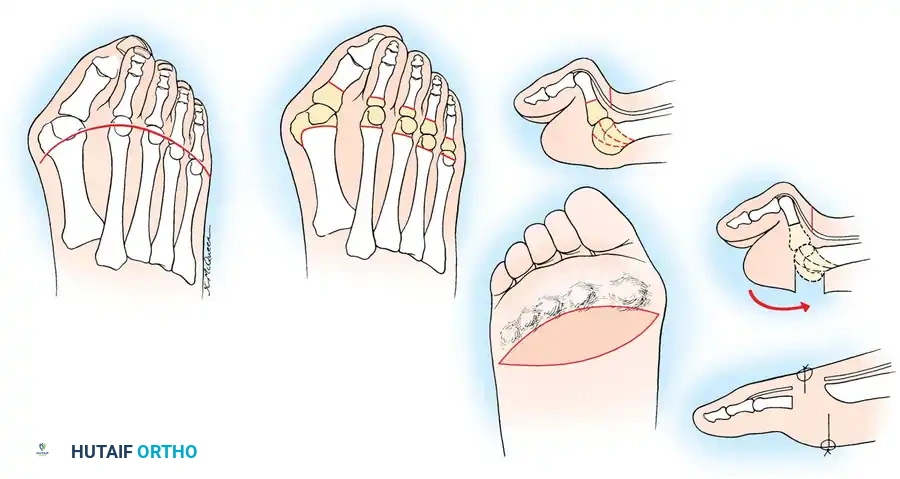
Step 3: Lesser Metatarsal Head Resection
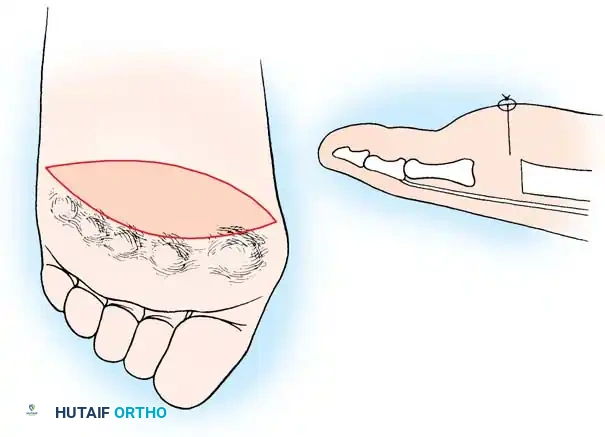
- Approach: Two dorsal longitudinal incisions are typically utilized (one centered between the 2nd and 3rd rays, and one between the 4th and 5th rays) to access all lesser MTP joints while preserving dorsal skin bridges. Alternatively, a transverse plantar approach can be used if severe plantar callosities require excision.
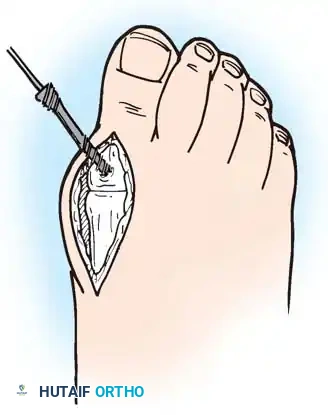
- Resection: The extensor tendons are retracted or lengthened (Z-plasty). The dorsal capsule is opened, and the collateral ligaments are sharply divided to allow plantarflexion of the metatarsal.
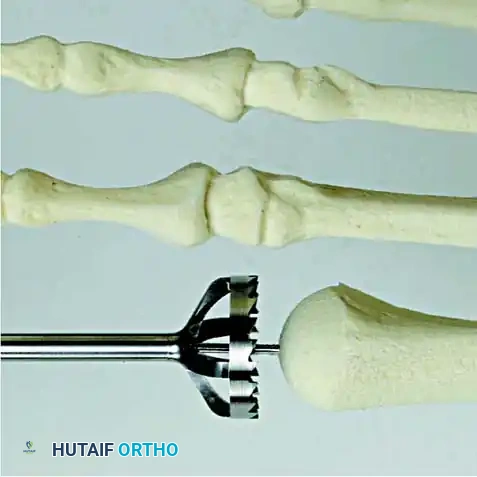
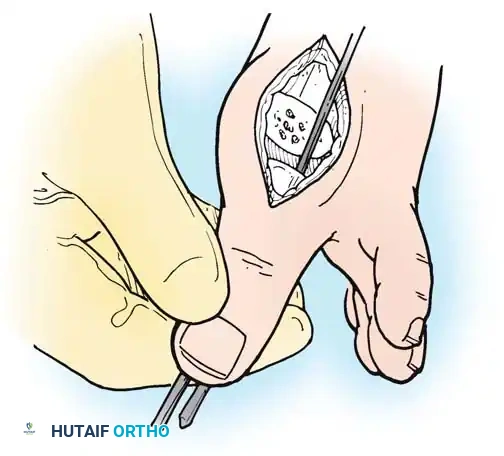
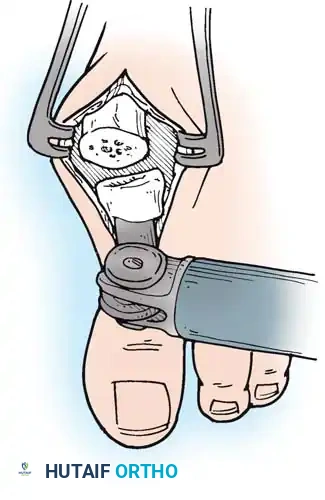
- Osteotomy: An oscillating saw is used to resect the metatarsal heads at the anatomical neck. It is imperative to create a smooth, parabolic cascade (the 2nd metatarsal should be the longest, tapering down to the 5th).
- Soft Tissue Balancing: The plantar plate and fat pad, which have migrated distally, are mobilized and pulled proximally under the remaining metatarsal stumps. If the toes remain contracted, closed osteoclasis or PIP joint resection arthroplasties may be performed.
- Pinning: Smooth Kirschner wires (K-wires) are driven antegrade through the toes and retrograde into the metatarsal shafts to hold the toes in neutral alignment.

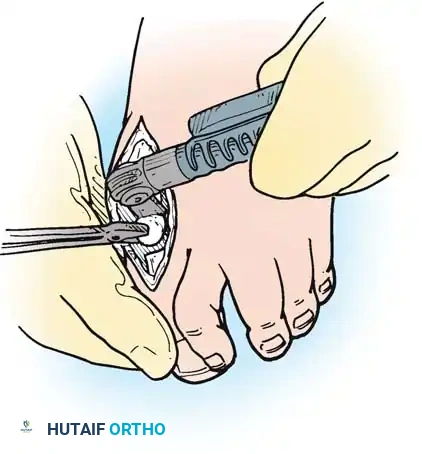
Intraoperative view demonstrating the exposure and resection of the lesser metatarsal heads to decompress the forefoot and allow reduction of the dislocated digits.
Postoperative Protocol and Outcomes
Immediate Postoperative Care
- Elevation: Strict elevation of the feet above heart level is mandatory for the first 48 to 72 hours to minimize edema and prevent wound sloughing.
- Weight-Bearing: Patients are placed in a rigid postoperative shoe or a short-leg cast. Heel-touch weight-bearing is permitted immediately, but forefoot loading is restricted until clinical and radiographic union of the first MTP joint is achieved (typically 6 to 8 weeks).
- Pin Management: Lesser toe K-wires are generally removed in the clinic at 3 to 4 weeks postoperatively.
- Suture Removal: As previously noted, sutures are left in place for 3 to 4 weeks, particularly in patients on chronic corticosteroids or biologic agents.
Long-Term Outcomes and Complications
Provided that adequate bone resection is performed and a smooth metatarsal cascade is achieved, the clinical results of forefoot arthroplasty are highly rewarding.
- Short-Term Success: Reduced pain, increased ambulatory function, improved cosmesis, and the ability to wear standard commercial footwear are achieved in 80% to 90% of patients initially.
- Long-Term Deterioration: After 3 to 5 years, objective success rates begin to decline. Vahvanen et al. observed 100 patients (179 feet) at a mean of 5 years. While 93% of patients considered the procedure a subjective success (51% completely satisfied, 42% satisfied with minor reservations), objective evaluation revealed that over 50% had recurrent deformities.

Fig. 81-9 (A, B) Radiographic evidence of bony proliferation at the distal end of the resected metatarsals. This remodeling can lead to recurrent plantar pressure and necessitates adequate initial resection.
Common long-term objective recurrences include:
1. Recurrence of hallux valgus (if arthrodesis was not performed or failed).
2. Dorsal posturing of the lesser phalanges on the metatarsal remnants.
3. Bony proliferation (osteophyte formation) on the distal ends of the resected metatarsals, leading to recurrent plantar keratoses.
Despite these objective radiographic recurrences, many patients maintain a high level of subjective satisfaction, largely because their overall activity level naturally decreases due to the systemic progression of rheumatoid arthritis. Nonetheless, meticulous surgical technique, aggressive preoperative optimization, and lifelong use of accommodative orthoses remain the cornerstones of successfully managing the rheumatoid forefoot.
Associated Surgical & Radiographic Imaging














📚 Medical References
- [Rheumatoid forefoot reconstruction. In Johnson KA, ed: Master techniques in orthopaedic surgery: the foot and ankle, New York, 1994, Raven.
Saltzman CL, Johnson KA, Donnelly RE: Surgical treatment for mild deformities of the rheumatoid forefoot by partial phalangectomy and syndactylization, Foot Ankle 14:325, 1993.](https://pubmed.ncbi.nlm.nih.gov/?term=Rheumatoid%20forefoot%20reconstruction.%20In%20Johnson%20KA%2C%20ed%3A%20Master%20techniques%20in%20orthopaedic%20surgery%3A%20the%20foot%20and%20ankle%2C%20New%20York%2C%201994%2C%20Raven.%0A%0ASaltzman%20CL%2C%20Johnson%20KA%2C%20Donnelly%20RE%3A%20Surgical%20treatment%20for%20mild%20deformities%20of%20the%20rheumatoid%20forefoot%20by%20partial%20phalangectomy%20and%20syndactylization%2C%20Foot%20Ankle%2014%3A325%2C%201993.)
- Sbarbaro JL Jr: Surgery of the rheumatoid foot and ankle. In Evarts MC, ed: Surgery of the musculoskeletal system, New York, 1983, Churchill Livingstone. Schwartzmann JR: The surgical management of foot deformities in rheumatoid arthritis, Clin Orthop Relat Res 36:86, 1964.
- Sebold EJ, Cracchiolo A 3rd: Use of titanium grommets in silicone implant arthroplasty of the hallux metatarsophalangeal joint, Foot Ankle Int 17:145, 1996.
- Sethu A, D’Netto DC, Ramakrishna B: Swanson’s Silastic implants in great toes, J Bone Joint Surg 62B:83, 1980.
- Shapiro JS: Forefoot resection in rheumatoid arthritis: evolution and results of a technique. Paper presented at the Tenth Annual Meeting of the American Orthopaedic Foot Society, Atlanta, Ga, Feb 6, 1980.
- Shereff MJ: Talocalcaneal (subtalar) arthrodesis. In Johnson KA, ed: Master techniques in orthopaedic surgery: the foot and ankle, New York, 1994, Raven. Sledge CB: Rheumatoid arthritis, Instr Course Lect 28:246, 1979.
- Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: a user-friendly technique, Foot Ankle 13:367, 1992.
- Smith RW, Shen W, Dewitt S, et al: Triple arthrodesis in adults with non-paralytic disease: a minimum ten-year follow-up study, J Bone Joint Surg 86A:2707, 2004.
- Spiegel TM, Spiegel JS: Rheumatoid arthritis in the foot and ankle: diagnosis, pathology, and treatment, Foot Ankle 2:318, 1982.
- Stockley I, Betts RP, Getty CJM, et al: A prospective study of forefoot arthroplasty, Clin Orthop Relat Res 248:213, 1989.
- Swanson AB: Implant arthroplasty for the great toe, Clin Orthop Relat Res 85:75, 1972.
- Swanson AB, Lumsden RM, Swanson GD: Silicone implant arthroplasty of the great toe, Clin Orthop Relat Res 142:30, 1979.
- Thomas S, Kinninmonth AW, Kumar CS: Long-term results of the modifi ed Hoffman procedure in the rheumatoid forefoot, J Bone Joint Surg 87A:748, 2005.
- Thomas S, Kinninmonth AW, Kumar CS: Long-term results of the modifi ed Hoffman procedure in the rheumatoid forefoot, J Bone Joint Surg 88A(suppl 1):149, 2006.
- Thompson FM, Mann RA: Arthritides. In Mann RA, Coughlin MJ, eds: Surgery of the foot and ankle, 6th ed, St Louis, 1993, Mosby. Thordarson DB, Aval S, Krieger L: Failure of hallux MP preservation surgery for rheumatoid arthritis, Foot Ankle Int 23:486, 2002.
- Tillmann K: Surgery of the rheumatoid forefoot with special reference to the plantar approach, Clin Orthop Relat Res 340:39, 1997.
- Trentham DE: Strategies for medical treatment based on current understanding of the pathogenesis of rheumatoid arthritis, Clin Orthop Relat Res 182:31, 1984.
- Trieb K: Management of the foot in rheumatoid arthritis, J Bone Joint Surg 87B:1171, 2005.
- Trnka HJ: Arthrodesis procedures for salvage of the hallux metatarsophalangeal joint, Foot Ankle Clin 5:673, 2000.
- Turan I, Lindgren U: Compression-screw arthrodesis of the fi rst metatarsophalangeal joint of the foot, Clin Orthop 221:292, 1987.
- Urquhart MW, Mont MA, Michelson JD, et al:
You Might Also Like

