Rheumatoid Finger Deformities: Pathomechanics & Surgery

Key Takeaway
Rheumatoid arthritis frequently produces complex finger deformities, including intrinsic plus and swan-neck presentations. These result from a combination of synovial hypertrophy, capsular attenuation, and altered biomechanical forces. Successful surgical management requires a systematic approach, prioritizing proximal joint stability before addressing digital deformities. Treatment ranges from soft tissue rebalancing, such as intrinsic release and flexor digitorum superficialis tenodesis, to salvage procedures like proximal interphalangeal joint arthrodesis or arthroplasty, depending on joint flexibility and articular destruction.
PATHOMECHANICS OF RHEUMATOID FINGER DEFORMITIES
Deformities of the fingers in rheumatoid arthritis (RA) are the culmination of destructive synovitis interacting with the complex biomechanical forces of the hand. These deformities are driven by normal forces applied to joints that have been structurally compromised by the disease process. The extrinsic flexors and extensors, combined with the tightness of the intrinsic muscles, exert deforming forces on attenuated capsuloligamentous structures.
Specific anatomical failures include the displacement of the lateral bands of the extensor hood, rupture of the central slip, or attritional rupture of the long extensor or flexor tendons. Furthermore, abnormal forces act on joints already weakened by erosive pannus. Flexor tenosynovitis frequently produces a mechanical limitation of interphalangeal (IP) joint motion; consequently, the range of active flexion in these joints is significantly less than passive flexion.
Fig. 70-10 Rheumatoid nodules in the olecranon bursa and on the subcutaneous surface of the ulna, indicative of severe systemic rheumatoid disease.
Surgical Priorities in the Rheumatoid Patient
When managing the rheumatoid hand, the surgeon must view the upper extremity as a single functional unit. Souter advocated for a strict hierarchy of surgical interventions, emphasizing the correction of significant disease and deformity in the elbow and shoulder before addressing hand deformities.
According to Ferlic, Smyth, and Clayton, surgical priorities follow a descending order of importance:
1. Spine (Cervical instability is life-threatening)
2. Foot and Hip (Weight-bearing and ambulation)
3. Knee
4. Wrist (The foundation of hand function)
5. Shoulder and Thumb
6. Elbow
7. Fingers
Clinical Pearl: When multiple operations are indicated on a single hand, order of priority is paramount. Persistent tenosynovitis, impending tendon rupture, and nerve compression are high-priority problems. Generally, if wrist arthroplasty or arthrodesis is indicated, it must be performed first, as a stable wrist is a prerequisite for balanced digital function.
Radiographic evaluation demonstrating periarticular osteopenia, joint space narrowing, and early erosive changes typical of rheumatoid arthritis.
INTRINSIC PLUS DEFORMITY
The intrinsic plus deformity is characterized by flexion of the metacarpophalangeal (MCP) joints and extension of the proximal interphalangeal (PIP) joints. It is caused by the tightness, spasm, and eventual ischemic contracture of the intrinsic muscles (lumbricals and interossei) secondary to rheumatoid inflammation.
In hands with a fixed intrinsic plus deformity, the PIP joint cannot be flexed while the MCP joint is fully extended. This deformity frequently develops in combination with volar subluxation of the MCP joints and ulnar deviation of the fingers.
Clinical Evaluation of Intrinsic Tightness
Accurate clinical testing is essential to differentiate intrinsic tightness from capsular contracture or extrinsic tendon adhesions.
The Bunnell Test for Intrinsic Tightness:
To perform this test, the MCP joint is passively held in maximum extension. This maneuver places the intrinsic muscles on stretch. If the intrinsics are tight, passive flexion of the PIP joint is prevented or significantly limited. Conversely, when the MCP joint is passively flexed (relaxing the intrinsics), passive flexion of the PIP joint increases.

Fig. 70-11 The Bunnell test for intrinsic tightness. Extension of the MCP joint exacerbates PIP extension forces if the intrinsics are contracted.
Surgical Warning: With ulnar drift of the fingers, intrinsic tightness may be present only on the ulnar side. To test this accurately, axial alignment of the finger with the metacarpal must be maintained. Any ulnar deviation at the MCP joint during the test slackens the intrinsics on the ulnar side and will yield a false-negative result.
A tight first volar interosseous muscle pulls the extended index finger ulnarward. If the finger is held in line with the second metacarpal during the test, tightness of this specific muscle can be isolated. The first volar interosseous is a flexor and adductor of the second MCP joint, whereas the first dorsal interosseous is typically an abductor only.
Oblique Retinacular Ligament (ORL) Test:
Tightness in the oblique retinacular ligament is demonstrated by maintaining the PIP joint in extension while testing the distal interphalangeal (DIP) joint's resistance to passive flexion. This is particularly helpful when evaluating a digit with an evolving boutonnière or swan-neck deformity.

Fig. 70-12 Test for tightness of the oblique retinacular ligament. The PIP joint is held in maximal extension by the examiner while resistance to passive flexion of the DIP joint is evaluated.
Management of Intrinsic Tightness
Release of the volar intrinsics, especially the abductor digiti quinti, was previously thought to reduce ulnar drift when performed early. However, it is usually ineffective in isolation because factors other than tight intrinsics (e.g., radial deviation of the wrist, volar plate attenuation) contribute heavily to the deformity.
When indicated, intrinsic tightness may be released in conjunction with MCP synovectomy by mobilization of the lateral bands. If severe degeneration of the MCP joints requires arthroplasty, the resection of the metacarpal head often shortens the skeletal framework sufficiently to relax the intrinsic mechanism without requiring a formal release.

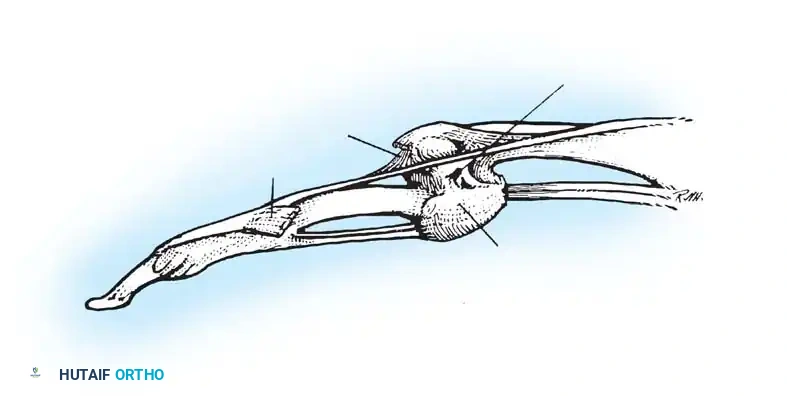
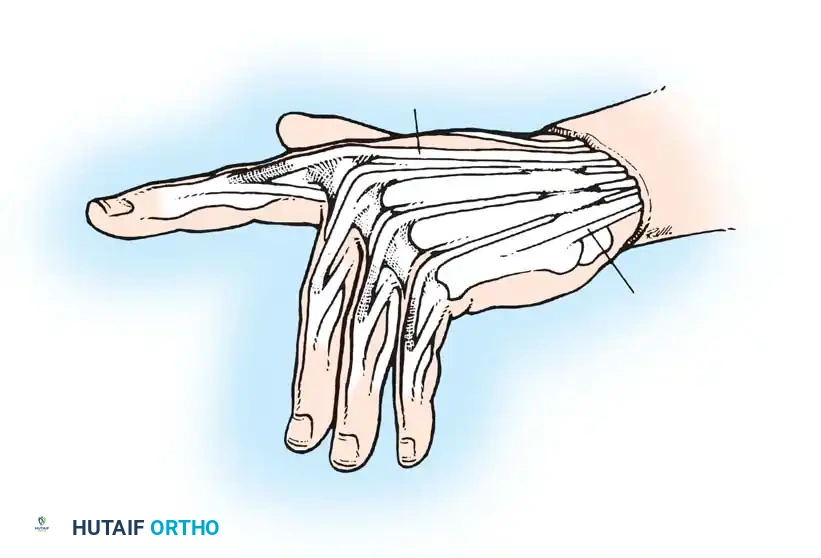
Anatomical illustration of the intrinsic musculature and its relationship to the extensor hood mechanism.
SWAN-NECK DEFORMITY
The swan-neck deformity is defined by a primary hyperextension posture of the PIP joint and a flexion posture of the DIP joint, often accompanied by flexion of the MCP joint. It is driven by profound muscle imbalance and capsular attenuation.
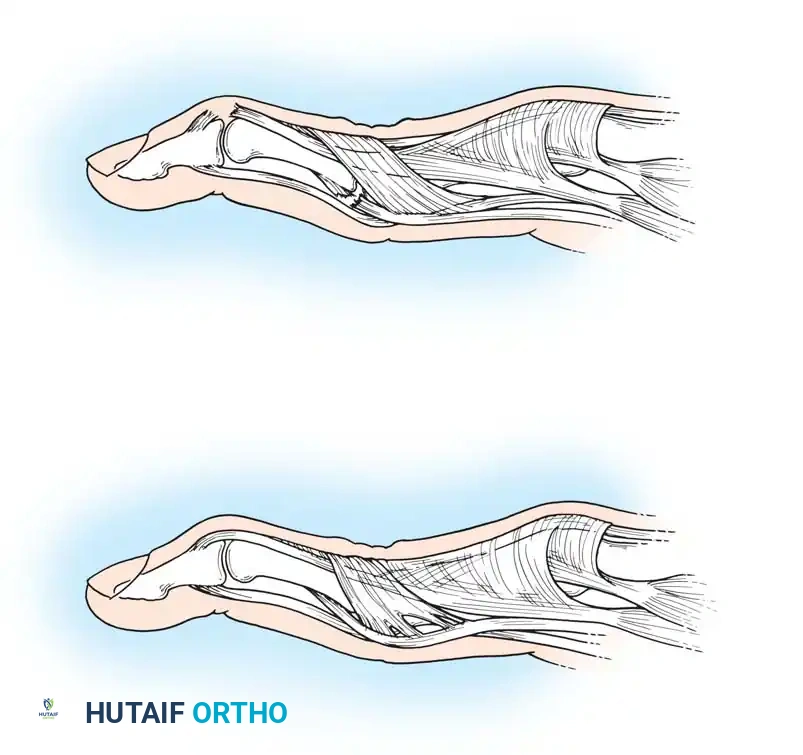
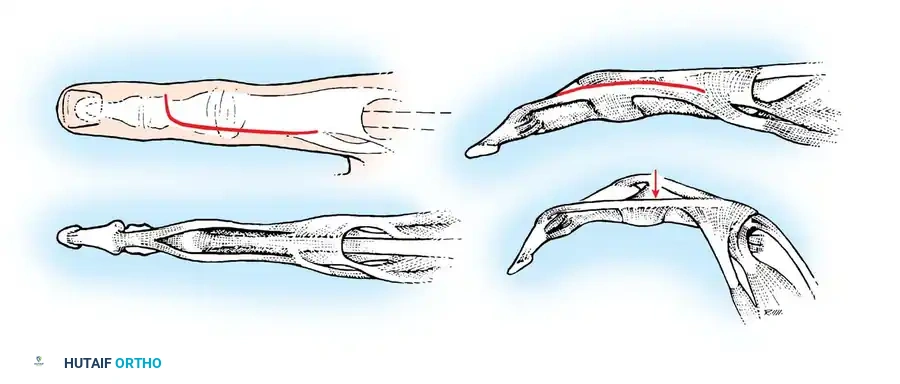
Fig. 70-13 Swan-neck deformity pathomechanics. (A) Terminal tendon rupture leading to DIP flexion and secondary PIP hyperextension. (B) Lateral-band subluxation dorsal to the axis of rotation of the PIP joint.
Pathogenesis
Although classically associated with rheumatoid arthritis, swan-neck deformities also occur in patients with generalized ligamentous laxity (e.g., Ehlers-Danlos syndrome) or post-traumatic conditions. In the rheumatoid hand, the deformity can originate at either the DIP or PIP joint:
- DIP Joint Origin: The deformity may begin as a mallet finger due to attenuation or disruption of the terminal extensor tendon at the DIP joint. This leads to secondary overpull of the central slip, causing hyperextension of a lax PIP joint.
- PIP Joint Origin: Synovitis of the PIP joint causes herniation of the volar capsule and attenuation of the volar plate. This allows the lateral bands and central tendon to subluxate dorsally. Eventually, the lateral bands adhere in a fixed dorsal position, preventing them from sliding volarly over the condyles during PIP flexion.

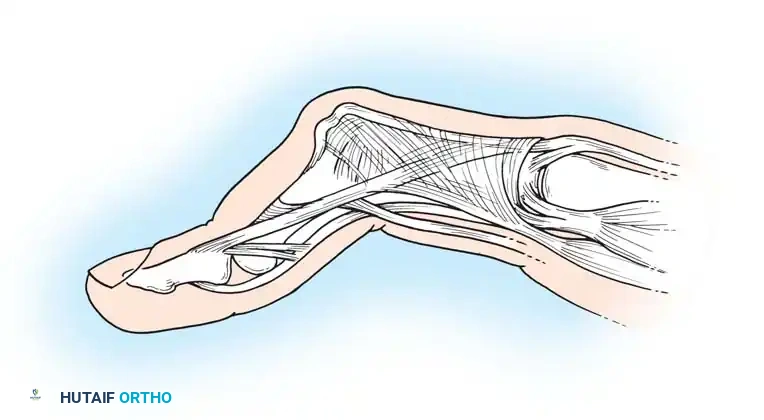
Fig. 70-14 Fixed rheumatoid swan-neck deformity, demonstrating severe PIP joint hyperextension and DIP joint flexion.
Nalebuff Classification and Treatment Algorithm
Nalebuff, Feldon, and Millender categorized rheumatoid swan-neck deformities into four distinct types, guiding the surgical approach:
- Type I: Deformities are flexible in all positions.
- Treatment: Dermodesis, flexor tenodesis of the PIP joint, fusion of the DIP joint, or reconstruction of the retinacular ligament.
- Type II: Deformities are characterized by intrinsic muscle tightness (PIP flexion is limited when the MCP is extended).
- Treatment: Intrinsic release combined with Type I procedures.
- Type III: Deformities are stiff and do not allow satisfactory passive PIP flexion, but lack significant radiographic joint destruction.
- Treatment: Joint manipulation, mobilization of the lateral bands, and dorsal skin release.
- Type IV: Deformities exhibit severe stiffness with radiographic evidence of intra-articular destruction.
- Treatment: Arthrodesis of the PIP joint or, in the ring and small fingers, Swanson implant arthroplasty.
Radiographic evidence of Type IV joint destruction requiring salvage procedures such as arthrodesis or arthroplasty.
The Role of Flexor Tenosynovitis
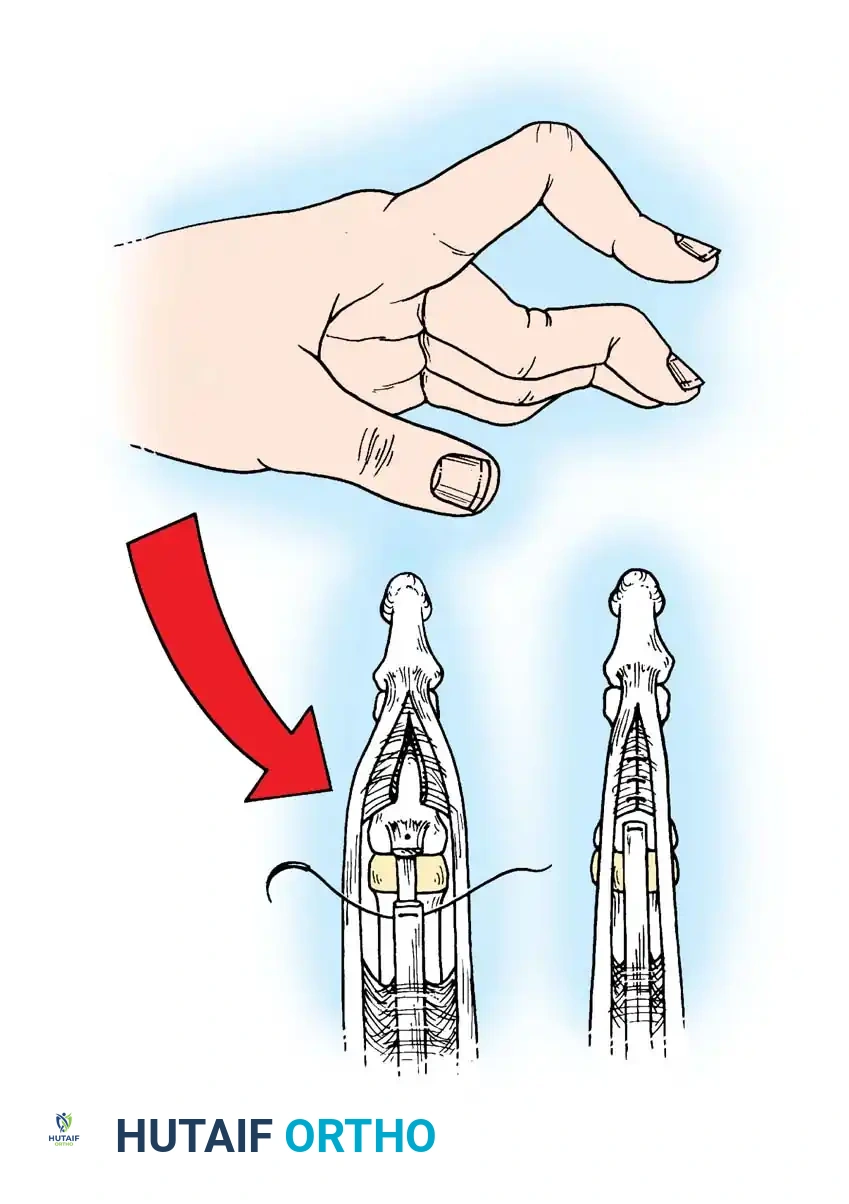
Beckenbaugh observed that flexor tenosynovitis results in ineffective volar support by the flexor digitorum superficialis (FDS) tendon, acting as a primary catalyst for swan-neck deformity. Adherence of the FDS tendon prevents it from stabilizing the PIP joint against hyperextension. The unopposed overpull of the central tendon, combined with PIP synovitis, stretches the volar plate, locking the joint in hyperextension.
To counteract this, Beckenbaugh advocated creating a volar tenodesis across the PIP joint using one slip of the FDS tendon.
Intraoperative exposure demonstrating the dorsal subluxation of the lateral bands contributing to the swan-neck posture.
SURGICAL TECHNIQUES
Correction of PIP Hyperextension Deformity (Beckenbaugh FDS Tenodesis)
This technique utilizes a slip of the FDS to create a volar tether, preventing PIP hyperextension while allowing active flexion.
TECHNIQUE 70-1: Beckenbaugh
-
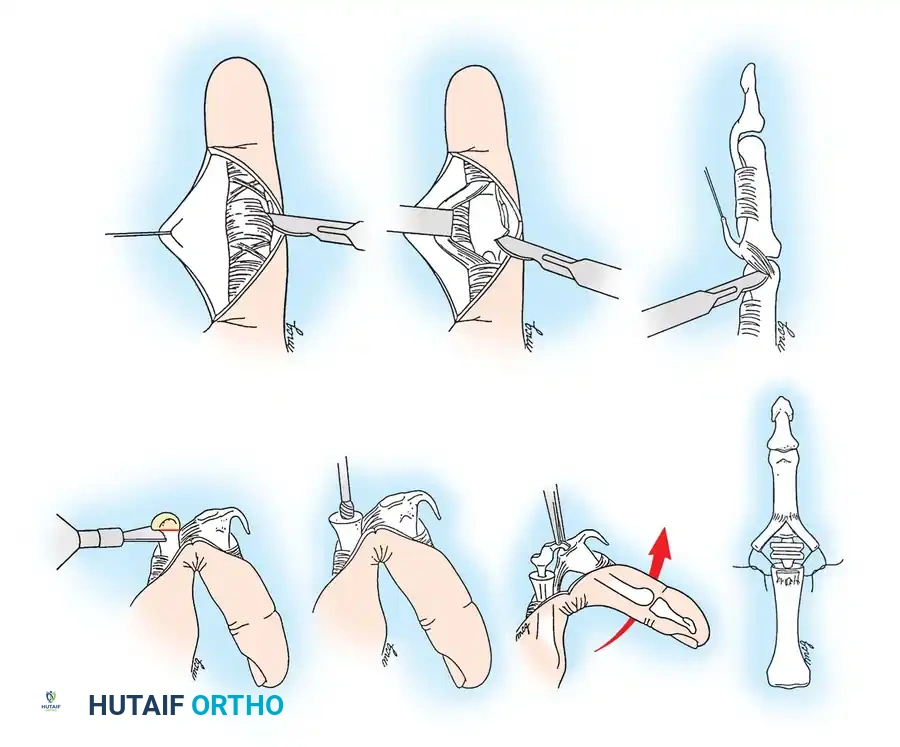
Incision and Exposure: Make a volar zigzag (Bruner) incision over the middle and proximal phalanges. Meticulously avoid damaging the digital neurovascular bundles, which may be displaced or adherent to the cruciate pulley system anterior to the hyperextended PIP joint.
Volar zigzag incision providing wide exposure of the flexor tendon sheath. -
Pulley Identification: Expose the cruciate pulleys by elevating the neurovascular bundles medially and laterally. Clearly identify and expose the A2 pulley.

Exposure of the A2 pulley, a critical structure that must be preserved for the tenodesis. -
Tendon Sheath Incision: Incise the central pulley system (C1/A3) centrally to expose the underlying flexor tendons.

Retraction of the profundus tendon and exposure of the sublimis (FDS) tendon for synovectomy. -
Synovectomy: Retract the flexor digitorum profundus (FDP) tendon and release any adhesions. Expose the FDS tendon, release its adhesions, and perform a thorough flexor tenosynovectomy.
-
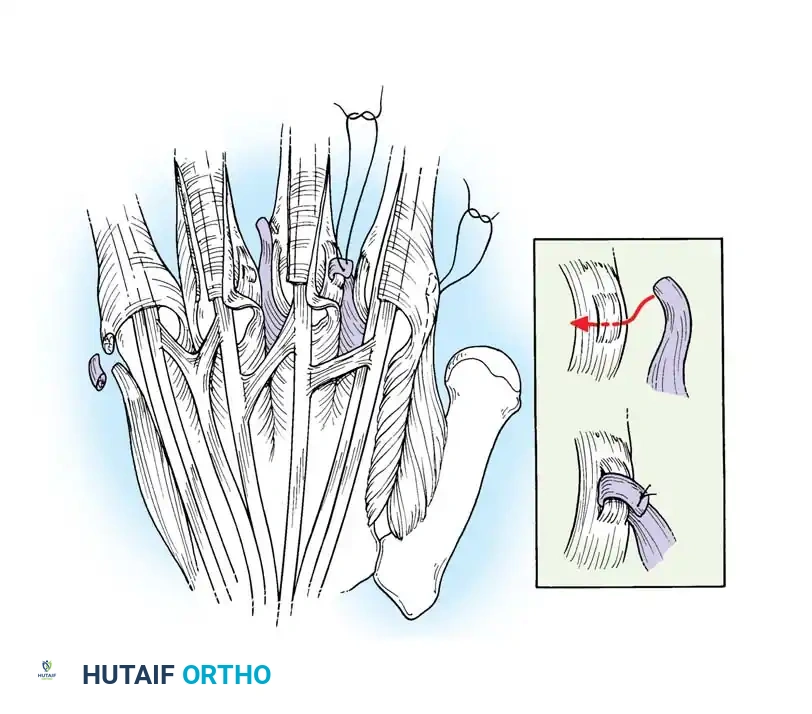
Tendon Preparation: Pull the FDS tendon distally and incise the decussation (Camper's chiasm), splitting the tendon into its two constituent slips. If necessary, extend the incision proximally and release adhesions at the A1 pulley level to allow adequate distal translocation of the tendon.

Splitting the FDS tendon into two slips at the level of the decussation. -
Slip Harvesting: Pull the divided FDS tendon distally and incise the ulnar slip proximally, leaving a 5-cm slip of tendon attached to its insertion on the ulnar side of the middle phalanx. Pull the slip firmly to ensure its insertion has not been compromised by erosive synovitis. (Note: In the little finger, both slips are often incised and used together because a single slip is usually too diminutive).
-
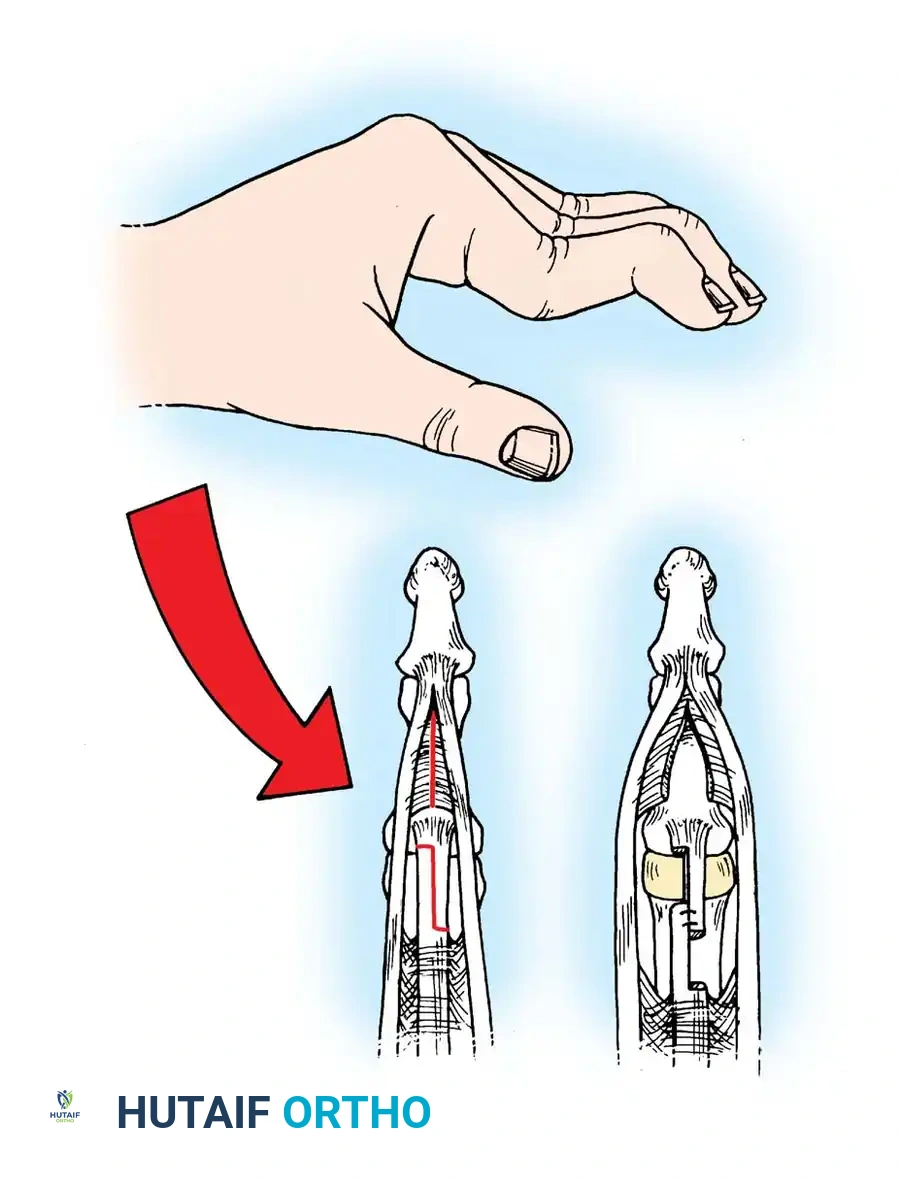
Pulley Fenestration: Puncture the A2 pulley 3 to 4 mm from its distal border using a scalpel or fine tenotomy scissors.

Creating a small fenestration in the distal aspect of the A2 pulley. -
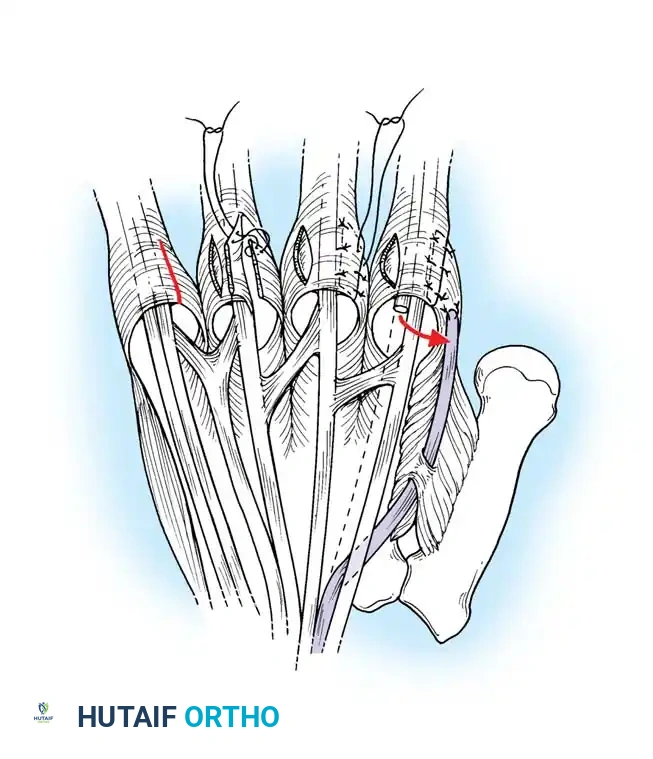
Tendon Routing: Pass a small curved hemostat through the hole distally into the sheath. Clamp the tip of the harvested FDS tendon slip and pull it proximally through the fenestration in the A2 pulley.
Routing the FDS slip proximally through the A2 pulley to create the tenodesis effect. -
Tensioning and Suturing: Bring the slip of tendon distally, folding it back on itself. Adjust the tension so that the digit is held at exactly 5 to 10 degrees of flexion at the PIP joint. Suture the tendon to itself using nonabsorbable 4-0 braided sutures.

Securing the tendon slip to itself under appropriate tension.

The completed FDS tenodesis, preventing PIP hyperextension while permitting active flexion.
- Closure: Repair the cruciate pulley if feasible. Close the skin over a small drain. Apply a sterile compressive dressing supported by a dorsal blocking splint to prevent hyperextension of the PIP joints.
Pitfall: Over-tensioning the tenodesis can result in a severe, iatrogenic PIP flexion contracture exceeding 30 degrees. Ensure the joint rests at no more than 10 degrees of flexion before final suture placement.
Lateral Band Mobilization and Skin Release (Nalebuff and Millender)
For Type III swan
Associated Surgical & Radiographic Imaging

You Might Also Like

