Arthroscopic Treatment of Elbow Osteochondritis Dissecans: A Comprehensive Surgical Guide
Key Takeaway
Arthroscopic management of capitellar osteochondritis dissecans (OCD) requires meticulous preoperative planning and precise surgical execution. Treatment algorithms are dictated by lesion stability, ICRS grading, and articular congruity. Techniques range from retrograde drilling for stable lesions to microfracture, fragment fixation, or osteochondral autograft transfer for unstable variants. Proper patient positioning and strategic portal placement are critical for optimal visualization and successful restoration of the radiocapitellar joint.
INTRODUCTION TO CAPITELLAR OSTEOCHONDRITIS DISSECANS
Osteochondritis dissecans (OCD) of the elbow primarily affects the capitellum and is a focal idiopathic alteration of subchondral bone with risk for secondary compromise of the overlying articular cartilage. It is most frequently observed in adolescent athletes engaged in repetitive overhead or upper-extremity weight-bearing activities, such as baseball pitchers and gymnasts. The pathophysiology is driven by repetitive valgus extension overload, which induces excessive radiocapitellar compressive forces. Combined with the tenuous, end-arterial blood supply of the capitellum, this microtrauma leads to focal ischemia, subchondral bone necrosis, and eventual fragmentation.
The arthroscopic management of capitellar OCD represents the gold standard for operative intervention. It offers superior visualization of the articular surface, allows for dynamic assessment of lesion stability, and facilitates a wide array of therapeutic interventions with minimal soft-tissue morbidity compared to open arthrotomy.
Clinical Pearl: Do not confuse capitellar OCD with Panner's disease. Panner's disease is an osteochondrosis of the entire capitellum occurring in younger children (typically under 10 years of age), is self-limiting, and rarely requires surgical intervention. OCD occurs in adolescents (11–17 years) and frequently leads to unstable osteochondral fragments requiring arthroscopic management.
PREOPERATIVE EVALUATION AND IMAGING
A thorough clinical examination typically reveals lateral-sided elbow pain, localized swelling, and a loss of terminal extension. Mechanical symptoms such as catching, locking, or crepitus strongly suggest an unstable lesion or the presence of loose bodies.
Radiographic Assessment
Standard anteroposterior (AP), lateral, and oblique radiographs of the elbow are mandatory. The AP view in 45 degrees of flexion is particularly useful for profiling the capitellum and identifying radiolucencies, flattening, or loose bodies.
Magnetic Resonance Imaging (MRI)
MRI is the imaging modality of choice for assessing the size, depth, and stability of the OCD lesion. The DeSmet and Takahara criteria are widely utilized to determine lesion stability on MRI.
MRI Criteria for Instability (DeSmet):
* A high-signal-intensity line (T2-weighted) surrounding the OCD lesion, indicating fluid interposition between the fragment and the crater.
* A focal osteochondral defect or empty crater.
* The presence of intra-articular loose bodies.
* Multiple subchondral cysts (>5 mm) adjacent to the lesion.
TREATMENT ALGORITHM AND PROTOCOL
The decision-making process for capitellar OCD is dictated by the stability of the lesion, the integrity of the overlying articular cartilage, and the International Cartilage Repair Society (ICRS) grading system.
Non-Operative Management (Stable Lesions)
For lesions deemed stable (based on Takahara criteria and DeSmet MRI criteria), conservative management is the first line of treatment.
* Protocol: Strict rest from the offending activity, utilization of a control motion brace, and close clinical follow-up to monitor healing at 6 weeks.
* Imaging Follow-up: A repeat MRI is obtained at 3 months to assess subchondral bone healing.
* Return to Play: The athlete may return to activity only when the lesion is radiographically healed and the patient is entirely asymptomatic.
Operative Management (Unstable Lesions - ICRS Grades 1-4)
When conservative measures fail, or if the lesion is acutely unstable, arthroscopic intervention is indicated. The surgical strategy is tailored to the specific ICRS grade and the morphological characteristics of the lesion.
- Grade 1 (Stable, continuous but softened cartilage): Arthroscopic transarticular or retroarticular drilling using a 0.062-inch Kirschner wire to stimulate angiogenesis and subchondral healing.
- Grade 2-4 (Contained lesion, stable articulation): Arthroscopic debridement of the necrotic bone and marrow stimulation via microfracture.
- Grade 2-4 (Unstable articulation, excellent quality cartilage and bone): In situ fragment fixation using bioabsorbable pins or headless compression screws. Note: Healing in this scenario remains somewhat guarded due to the avascular nature of the fragment.
- Grade 2-4 (Unstable articulation, unipolar lesion): Osteochondral autograft transfer system (OATS) to restore the articular contour with viable hyaline cartilage.
- Grade 2-4 (Unstable articulation, bipolar lesion): In cases where both the capitellum and the radial head are involved (bipolar "kissing" lesions), complex reconstruction is often unfeasible. The treatment of choice is arthroscopic debridement, microfracture, and strict postoperative activity modification.
SURGICAL TECHNIQUE: PATIENT POSITIONING AND SETUP
Meticulous patient positioning is paramount for safe portal placement and comprehensive visualization of the radiocapitellar joint.
- Anesthesia: General anesthesia is typically preferred, often supplemented with a regional block (e.g., supraclavicular or axillary nerve block) for postoperative pain control.
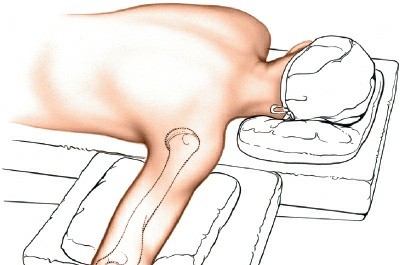
- Positioning: Place the patient in the supine position.
- Suspension and Traction: The operative arm is held in balanced suspension. Apply 5 to 6 lb of longitudinal traction to the forearm.
- Joint Orientation: The shoulder is positioned in 90 degrees of abduction, and the elbow is maintained in 90 degrees of flexion.
Surgical Warning: Maintaining the elbow at 90 degrees of flexion during portal placement is critical. This position allows the neurovascular structures (specifically the radial and median nerves) to fall anteriorly, maximizing the safe zone for anterior portal establishment.
ARTHROSCOPIC PORTAL PLACEMENT
Diagnostic arthroscopy of the elbow requires a systematic approach. Generally, five portals are necessary to fully visualize the anterior and posterior compartments, address loose bodies, and treat the capitellar OCD lesion.
Joint Distension
Before making any incisions, the elbow joint must be maximally distended to push the neurovascular structures away from the capsule.
* Identify the "soft spot" in the center of the triangle formed by the lateral epicondyle, the radial head, and the tip of the olecranon.
* Insert an 18-gauge spinal needle through the soft spot and inject 20 to 30 mL of sterile normal saline until backflow is achieved and the capsule is palpably tense.
The Mid-Anterolateral Portal
The mid-anterolateral portal is the primary viewing portal for the anterior compartment and provides an excellent trajectory for visualizing the capitellum.
* Landmarks: The portal is located approximately 1 cm proximal and 1 cm anterior to the lateral epicondyle.
* Technique: Use a spinal needle to confirm the trajectory into the radiocapitellar joint. Once confirmed, use a No. 11 blade to incise the skin only.
* Blunt Dissection: Use a mosquito hemostat to bluntly dissect down to the capsule to protect the radial nerve.
* Instrumentation: Insert the arthroscopic cannula with a blunt trocar. A standard 4-mm, 30-degree arthroscope is typically used to visualize the anterior portion of the joint, assess for loose bodies, and evaluate the extent of the OCD lesion. In smaller pediatric patients, a 2.7-mm arthroscope may be utilized to prevent iatrogenic scuffing of the articular cartilage.
Additional Portals
Depending on the location of the lesion and the required intervention, additional portals are established under direct intra-articular visualization:
* Proximal Anteromedial Portal: Used as the primary working portal for anterior compartment pathology.
* Direct Lateral / Soft Spot Portal: Excellent for viewing the radiocapitellar articulation directly.
* Posterolateral and Direct Posterior Portals: Necessary for evaluating the olecranon fossa, removing posterior loose bodies, and addressing concurrent valgus extension overload osteophytes.
SURGICAL PROCEDURES FOR CAPITELLAR OCD
Once the diagnostic sweep is complete and the lesion is identified, the specific surgical intervention is executed based on the preoperative plan and intraoperative findings.
1. Drilling of Intact Lesions (ICRS Grade 1)
For lesions with intact but softened cartilage, the goal is to decompress the subchondral bone and stimulate revascularization without violating the articular surface if possible.
* Retroarticular Drilling: Under fluoroscopic guidance, a 0.062-inch K-wire is advanced from the posterior aspect of the lateral epicondyle into the OCD lesion, stopping just short of the articular cartilage.
* Transarticular Drilling: If retroarticular access is challenging, transarticular drilling can be performed directly through the cartilage using a smooth K-wire, creating multiple small channels to allow marrow elements to access the ischemic bone.
2. Debridement and Microfracture (ICRS Grades 2-4, Contained)
For lesions with fragmented or detached cartilage but a contained crater (intact peripheral rim), microfracture is the workhorse procedure.
- Preparation: The unstable osteochondral fragment is excised using arthroscopic graspers.
- Debridement: An arthroscopic curette and motorized shaver are used to debride the base of the crater down to stable, bleeding subchondral bone. The margins of the lesion must be sharply debrided to create vertical walls, which helps contain the marrow superclot.
- Microfracture: Arthroscopic awls (typically 45-degree and 90-degree angles) are used to penetrate the subchondral bone plate. The holes should be spaced 2 to 3 mm apart and depth should be approximately 3 to 4 mm to access the cancellous marrow.
- Verification: The arthroscopic pump pressure is temporarily lowered to verify the egress of fat droplets and marrow blood from the microfracture holes, confirming adequate depth.
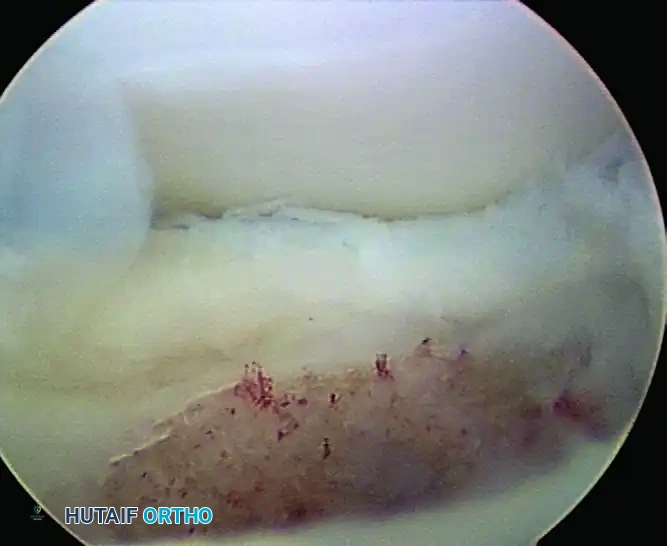
FIGURE 52-67: Microfracture of crater of osteochondritis dissecans lesion less than 1 cm in size with stable lateral rim. Note the punctate bleeding from the subchondral bone indicating adequate marrow stimulation.
3. Fragment Fixation (ICRS Grades 2-4, Unstable with Good Bone Quality)
If a large, unstable fragment is encountered that possesses excellent cartilage and a substantial piece of attached subchondral bone, fixation may be attempted.
* The crater is debrided of fibrous tissue and lightly burred to expose bleeding bone.
* The fragment is reduced into the crater.
* Fixation is achieved using bioabsorbable darts, pins, or headless titanium compression screws.
* Caveat: The surgeon must counsel the patient that healing is guarded, as the fragment has suffered an ischemic insult, and nonunion or subsequent fragmentation remains a significant risk.
4. Osteochondral Autograft Transfer (OATS) (ICRS Grades 2-4, Unipolar)
For large, uncontained lesions where microfracture is likely to fail (typically >1.5 cm or involving the lateral capitellar margin), OATS provides immediate structural restoration.
* Harvest: A cylindrical osteochondral plug is harvested from a non-weight-bearing portion of the ipsilateral knee (e.g., the lateral periphery of the lateral femoral condyle).
* Preparation: The capitellar defect is reamed to a precise depth and diameter matching the harvested plug. This often requires a mini-open arthrotomy if the lesion cannot be accessed perpendicularly via arthroscopic portals.
* Implantation: The graft is press-fit into the capitellar defect, ensuring the articular surface is perfectly flush with the surrounding native cartilage. Proud grafts will lead to rapid degeneration of the radial head.
5. Management of Bipolar Lesions
When both the capitellum and the radial head exhibit advanced chondral damage, the prognosis is poor. Extensive reconstructive procedures are generally contraindicated. The surgical approach is palliative: arthroscopic debridement of loose flaps, removal of loose bodies, and microfracture of exposed bone. Postoperatively, the patient must undergo strict activity modification, permanently retiring from heavy upper-extremity loading or throwing sports.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative rehabilitation protocol is highly dependent on the specific surgical intervention performed.
Following Debridement and Microfracture
- Phase 1 (Weeks 0-2): The elbow is placed in a posterior splint at 90 degrees of flexion for 3 to 5 days to allow the marrow clot to stabilize. Gentle, passive range of motion (ROM) is initiated thereafter.
- Phase 2 (Weeks 2-6): Active-assisted and active ROM exercises are progressed. A hinged elbow brace may be used to protect the joint from valgus stress. Weight-bearing through the arm is strictly prohibited.
- Phase 3 (Weeks 6-12): Progressive strengthening of the forearm, biceps, triceps, and rotator cuff begins.
- Phase 4 (Months 3-6): An interval throwing program or sport-specific training is initiated only after MRI confirms adequate filling of the defect with fibrocartilage and the patient has full, painless ROM.
Following OATS or Fragment Fixation
- The initial protection phase is extended. ROM is initiated early to nourish the cartilage, but any loading or valgus stress is delayed until radiographic evidence of bony incorporation is observed (typically 8 to 12 weeks).
- Return to competitive throwing or gymnastics may take 6 to 12 months and requires rigorous functional testing.
COMPLICATIONS AND PITFALLS
While arthroscopic management of capitellar OCD is highly effective, surgeons must be vigilant regarding potential complications:
1. Neurological Injury: The radial nerve is at highest risk during the establishment of the anterolateral portals. Strict adherence to the "soft spot" distension and blunt dissection techniques is mandatory.
2. Stiffness: The elbow is notoriously prone to arthrofibrosis. Prolonged immobilization must be avoided. Early, controlled ROM is the key to preventing capsular contracture.
3. Progression to Osteoarthritis: Despite optimal surgical management, large lesions, bipolar disease, or failure of graft incorporation can lead to early-onset radiocapitellar arthritis. Patients and parents must be counseled preoperatively regarding the long-term prognosis of the joint.
📚 Medical References
- elbow osteochondritis dissecans, Am J Orthop 5:237, 2003.
- Bauer M, Johnsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: a long-term follow-up study, Clin Orthop Relat Res 284:156, 1992.
- Bauer M, Johnsson K, Lindén B: Osteochondritis of the ankle: a 20-year follow-up study, J Bone Joint Surg 69B:93, 1987.
- Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classifi cation and treatment of osteochondritis dissecans of the capitellum, Am J Sports Med 26:520, 1998.
- Berlet GC, Mascia A, Miniaci A: Treatment of unstable osteochondritis dissecans lesions of the knee using auto-genous osteochondral grafts (mosaicplasty), Arthroscopy 15:312, 1999.
- Binek R, Levinsohn EM, Bersani F, et al: Freiberg disease complicating unrelated trauma, Orthopedics 11:753, 1988.
- Bosworth DM: Autogenous bone pegging for epiphysitis of the tibial tubercle, J Bone Joint Surg 16:829, 1934.
- Bradley J, Dandy DJ: Results of drilling osteochondritis dissecans before skeletal maturity, J Bone Joint Surg 71B:641, 1989.
- Byrd JWT, Jones KS:
You Might Also Like