Web Space Infections of the Hand: Epidemiology, Surgical Anatomy, & Management
Key Takeaway
Web space infections are deep palmar abscesses in the hand's intermetacarpal compartments, typically caused by trauma. Key signs include pronounced dorsal hand edema and "splaying" of adjacent fingers. Diagnosis relies on clinical findings and understanding their critical surgical anatomy, especially lumbrical canal communications, demanding prompt management to prevent extensive morbidity.
Introduction & Epidemiology
Web space infections, or interdigital space infections, represent a common yet potentially debilitating form of deep palmar space infection. These abscesses occur within one of the four intermetacarpal compartments of the palm, typically distal to the superficial palmar arch and proximal to the common digital nerves bifurcation. While seemingly localized, the unique anatomical communications of these spaces necessitate prompt and accurate diagnosis followed by aggressive management to prevent extensive morbidities.
Epidemiologically, hand infections remain a significant cause of emergency department visits and operative interventions. Web space infections are frequently observed following minor penetrating trauma, such as splinters, thorns, or animal/human bites, which can introduce bacteria directly into the deep tissues. They can also arise from neglected or inadequately treated superficial infections (e.g., paronychia, felon) or represent a progression from tenosynovitis. Predisposing factors include diabetes mellitus, immunocompromised states (e.g., HIV, organ transplant recipients), intravenous drug use, poor hygiene, and occupations involving frequent hand trauma or exposure to contaminants.
The predominant causative organism is Staphylococcus aureus , including Methicillin-resistant S. aureus (MRSA), followed by streptococcal species. Polymicrobial infections are common, particularly in cases stemming from human or animal bites, contaminated wounds, or in immunocompromised patients, often involving Gram-negative bacilli and anaerobes. Early identification of the microbiological profile is critical for targeted antibiotic therapy.
Clinical presentation is often characterized by pronounced dorsal hand edema, which is a hallmark feature, as the dorsal skin of the web space is thinner and less restrictive than the palmar skin, allowing pus to point dorsally. This edema can be disproportionately large compared to the actual abscess size. Another classic sign is the abduction, or "splaying," of the two fingers adjacent to the affected web space, caused by the inflammatory swelling and pressure within the intermetacarpal compartment. Patients typically present with exquisite tenderness in the web space, warmth, erythema, and severe pain, often exacerbated by movement or pressure. Systemic symptoms such as fever, chills, and malaise may be present, indicating potential systemic involvement.
Differential diagnoses include cellulitis (without abscess), flexor tenosynovitis (Kanavel's signs), deep palmar space infections (midpalmar or thenar space), septic arthritis of the metacarpophalangeal (MCP) joint, foreign body reaction, gout, or a severe soft tissue contusion. Distinguishing web space infection from these entities is paramount for appropriate management.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate surgical anatomy of the web spaces is foundational to the successful management of these infections and the prevention of iatrogenic injury. There are four web spaces located between the metacarpal heads, housing critical structures and featuring unique communication pathways.
Web Space Boundaries
Each web space is an inverted pyramid-shaped compartment with distinct boundaries:
*
Proximal:
The level of the transverse metacarpal ligament and the septa originating from the palmar aponeurosis that bind the digital slips. These septa divide the palm into superficial and deep compartments.
*
Distal:
The level of the distal palmar crease, where the skin becomes thicker and more fibrous.
*
Palmar (Volar):
Formed by the volar skin, subcutaneous tissue, and the distal edge of the palmar aponeurosis. The palmar skin is notably thick and densely adherent, making palmar pointing of abscesses less common and challenging to palpate.
*
Dorsal:
Consists of the dorsal skin, subcutaneous tissue, dorsal aponeurosis, and the extensor tendons. The dorsal skin is significantly thinner and more pliable, explaining why pus often points dorsally and why dorsal incisions are typically preferred for drainage.
*
Medial/Lateral:
The sides of each web space are defined by the fibrous septa that extend from the palmar aponeurosis to the metacarpals, effectively compartmentalizing the palm.
Contents of the Web Spaces
The web spaces are densely packed with vital structures:
*
Lumbrical Muscles:
Each web space contains the lumbrical muscle associated with the radial side of the respective finger. These muscles originate from the flexor digitorum profundus (FDP) tendons in the palm and insert into the extensor expansions dorsally.
*
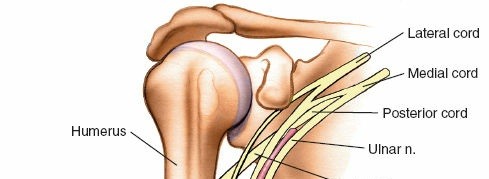
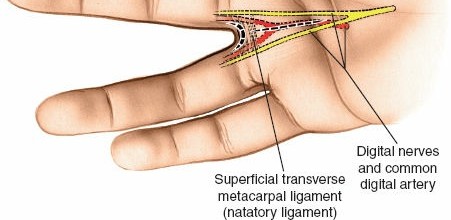
Neurovascular Bundles:
The common palmar digital nerves and arteries, which branch into proper digital nerves and arteries, traverse the web spaces distally. These structures are critical for sensation and vascular supply to the digits and are highly vulnerable during surgical dissection. The nerves are typically volar to the arteries.
*
Interosseous Muscles:
While the interossei lie deeper, between the metacarpals, their tendons contribute to the dorsal aponeurosis and are adjacent to the deep aspects of the web space.
*
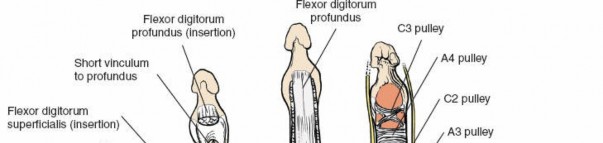
Flexor Tendon Sheaths:
The flexor digitorum superficialis (FDS) and profundus (FDP) tendons, encased in their synovial sheaths, lie immediately volar to the web spaces proper, separated by a thin fibrous septum.
Anatomical Communications
A critical anatomical consideration is the communication of the web spaces, particularly the lumbrical canals:
*
Lumbrical Canals:
The lumbrical muscles, as they pass from the palm into the web spaces, create fascial tunnels, or canals. These canals provide a direct conduit for infection to spread proximally from the web space into the deep midpalmar space. This pathway for spread underscores the urgency of intervention.
*
Adjacency to Flexor Tendon Sheaths:
The proximity of the web spaces to the flexor tendon sheaths creates a risk of tenosynovitis if an infection is left untreated or inadequately drained.
Biomechanics of Presentation
The characteristic finger abduction or "splaying" observed in web space infections is a direct biomechanical consequence of the anatomical confines and inflammatory response:
* Inflammatory edema and pus accumulation within the relatively unyielding web space compartment exert pressure on the adjacent flexor tendon sheaths and the intrinsic muscles (lumbricals and interossei).
* This pressure, combined with the inflammatory changes, can lead to mechanical separation and displacement of the fingers, particularly away from the affected web. The second and fourth web spaces are most commonly affected, leading to index-middle or ring-small finger splaying, respectively. The first web space (thumb-index) has a different anatomical configuration, making infection here more prone to thumb-index adduction contracture if not properly managed.
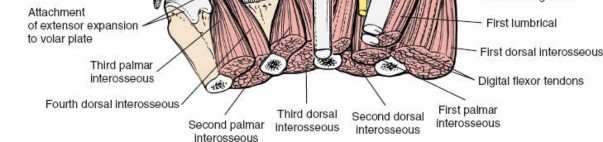
The image provided illustrates the characteristic dorsal edema and finger splaying indicative of a web space infection:
Indications & Contraindications
The decision-making process for the management of web space infections hinges on the clinical presentation, the presence and extent of purulence, and the patient's overall health status. The fundamental principle of treating any abscess is surgical incision and drainage (I&D).
Operative Indications
Surgical intervention is indicated in the following scenarios:
*
Presence of a true abscess:
Confirmed clinically by fluctuance, or by imaging (ultrasound, MRI) demonstrating a well-defined fluid collection consistent with pus. This is the primary indication for I&D.
*
Failure of conservative management:
If initial non-operative treatment for cellulitis (e.g., intravenous antibiotics, elevation, splinting) does not lead to clinical improvement within 24-48 hours, or if symptoms worsen, suggesting progression to abscess formation.
*
Progressive infection:
Rapidly worsening pain, swelling, erythema, or the development of systemic signs of infection (fever, chills, tachycardia, leukocytosis) despite antibiotic therapy.
*
Threat to vital structures:
Signs of impending spread to adjacent structures such as flexor tendon sheaths (flexor tenosynovitis), midpalmar space, thenar space, or suspicion of osteomyelitis or septic arthritis.
*
Retained foreign body:
If there is a high suspicion or confirmed presence of a foreign body (e.g., splinter, glass, metal fragment) that cannot be removed safely by non-surgical means, surgical exploration and removal are indicated, often concomitantly with drainage if infection is present.
*
Necrotic tissue:
Presence of devitalized tissue within the web space.
Non-Operative Indications
Non-operative management is appropriate for:
*
Early cellulitis without abscess formation:
Patients presenting with signs of localized inflammation (erythema, warmth, tenderness, swelling) but no demonstrable fluctuance or imaging evidence of a pus collection.
*
Mild, localized infection:
Where systemic signs are absent, and the patient is otherwise healthy.
*
Initial management prior to surgical drainage:
In some cases, a brief course of empirical intravenous antibiotics may be initiated to control spreading cellulitis before definitive I&D, especially if operative facilities are not immediately available or to stabilize a septic patient. However, this should not delay surgical drainage of an established abscess.
Contraindications
Absolute contraindications to incision and drainage of a true web space abscess are rare, as untreated deep space infections can lead to severe morbidity and mortality.
*
Misdiagnosis:
The most significant contraindication is the absence of an actual abscess. Draining cellulitis alone is ineffective and can be harmful.
*
Severe coagulopathy:
While a relative contraindication, this must be corrected preoperatively if possible. If not, the risks of bleeding must be weighed against the risks of leaving an abscess undrained.
*
Patient instability:
In an unstable patient with multiple comorbidities, operative drainage may need to be performed under local anesthesia or deferred until the patient is medically optimized, though this carries the risk of infection progression.
Table: Operative vs. Non-Operative Indications for Web Space Infection
| Parameter | Operative Management (I&D) | Non-Operative Management |
|---|---|---|
| Clinical Presentation | - Palpable fluctuance | - Diffuse erythema, warmth, tenderness without fluctuance |
| - Characteristic "splaying" of fingers with severe pain | - Early stages of inflammation, often post-trauma | |
| - Rapidly worsening localized symptoms | - Improving symptoms on antibiotics after 24-48 hours | |
| Imaging Findings | - Ultrasound demonstrating a well-defined anechoic or hypoechoic fluid collection (abscess) | - Ultrasound showing diffuse soft tissue edema and hyperemia without discrete fluid collection (cellulitis) |
| - MRI confirming abscess formation, often with surrounding inflammatory changes | - MRI showing diffuse inflammatory changes without a drainable collection | |
| Response to Treatment | - Failure of initial broad-spectrum antibiotic therapy to improve symptoms within 24-48 hours | - Prompt resolution or significant improvement of symptoms with intravenous antibiotics and conservative measures within 24-48 hours |
| Systemic Symptoms | - Persistent or worsening fever, chills, leukocytosis, elevated inflammatory markers (CRP, ESR) despite antibiotics | - Absence of or improving systemic signs of infection |
| Associated Factors | - Suspected or confirmed foreign body | - No evidence of foreign body |
| - Signs of spread to adjacent deep spaces (midpalmar, thenar, flexor tendon sheaths) | - Infection contained to the web space without signs of deeper spread | |
| Microbiology | - Persistent purulent drainage post-aspiration or prior attempts at conservative management | - Early empiric antibiotics initiated while awaiting cultures, or infection responding well to empiric therapy |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for ensuring a safe and effective surgical outcome for web space infections. This involves thorough diagnostic workup, appropriate antibiotic selection, and precise patient positioning.
Diagnostic Workup
- Clinical Assessment: A comprehensive history detailing the onset, progression, predisposing factors, and any prior treatments is crucial. Physical examination focuses on the classic signs: dorsal edema, finger splaying, tenderness, fluctuance (if present), and assessment for signs of proximal spread (e.g., palmar tenderness, limited digital flexion, tenderness along flexor sheaths).
-
Laboratory Studies:
- Complete Blood Count (CBC) with differential: To assess for leukocytosis and left shift, indicative of bacterial infection.
- Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP): Inflammatory markers that are typically elevated and can be monitored for response to treatment.
- Blood Cultures: If systemic signs of sepsis are present.
- Gram Stain and Cultures: If purulent material can be aspirated pre-operatively, it should be sent for Gram stain, aerobic, and anaerobic cultures. Fungal cultures may be considered in immunocompromised patients or specific exposures.
-
Imaging:
- Plain Radiographs (X-rays): Routine anteroposterior, lateral, and oblique views of the hand are necessary to rule out retained foreign bodies (especially radiopaque ones), gas in soft tissues, osteomyelitis (a late complication), or septic arthritis of the adjacent MCP joint.
- Ultrasound: This is often the most valuable imaging modality for confirming an abscess. It is non-invasive, readily available, and can precisely localize fluid collections, differentiate abscess from cellulitis, identify foreign bodies, and guide aspiration. Dynamic ultrasound can assess compressibility.
- Magnetic Resonance Imaging (MRI): While not routinely required for uncomplicated web space infections, MRI offers superior soft tissue contrast and can delineate the exact extent of infection, identify osteomyelitis, tenosynovitis, or involvement of deeper fascial planes, particularly in complex or refractory cases.
- CT Scan: Less useful than MRI for soft tissue infections but can identify bony involvement and gas.
Antibiotic Selection
Empiric intravenous antibiotic therapy should be initiated as soon as an infection is suspected and certainly pre-operatively. The choice should cover the most likely pathogens:
*
Staphylococcus aureus (including MRSA):
Given the high prevalence, MRSA coverage is often prudent. Options include Vancomycin, Daptomycin, Linezolid, or Clindamycin (if local resistance patterns allow).
*
Streptococcal species:
Penicillin-based antibiotics or cephalosporins are effective.
*
Gram-negative bacteria and anaerobes:
Consider in specific scenarios (e.g., bite wounds, immunocompromised hosts, chronic infections, IV drug users). Agents like Piperacillin-tazobactam, Cefepime with Metronidazole, or Carbapenems may be necessary.
Once culture and sensitivity results are available, the antibiotic regimen should be narrowed or adjusted accordingly.
Anesthesia
The choice of anesthesia depends on the patient's comorbidities, the extent of the infection, and surgeon preference.
*
General Anesthesia:
Often preferred for patient comfort, especially for longer or more complex cases, or anxious patients.
*
Axillary or Brachial Plexus Block:
Provides excellent anesthesia and post-operative analgesia for the entire arm and hand, suitable for most web space I&D procedures.
*
Intravenous Regional Anesthesia (Bier Block):
May be used for simpler, more localized cases but requires specific setup and duration limitations.
*
Regional Block (e.g., wrist block):
Can be considered for very superficial or small abscesses, though less reliable for deep web space involvement.
Patient Positioning and Surgical Preparation
The patient is placed supine on the operating table. The affected arm is positioned on a specialized hand table or arm board, allowing for maximal exposure and ergonomic access for the surgical team. This setup facilitates proper draping and instrument manipulation.
A pneumatic tourniquet is applied to the upper arm. Prior to inflation, the arm is elevated for approximately 3 minutes (as indicated in the seed content, see illustration in Figure 5-15, which is not provided but conceptualized by the instruction) to exsanguinate the limb via gravity. This provides a bloodless field, which is critical for identifying subtle anatomical structures, localizing pus, and meticulously dissecting around neurovascular bundles. The tourniquet is then inflated to a pressure typically 250-300 mmHg, or 100 mmHg above systolic blood pressure.
Standard sterile surgical preparation and draping are then performed, ensuring a wide operative field that includes the entire hand and distal forearm.
Detailed Surgical Approach / Technique
Surgical incision and drainage (I&D) of a web space infection demand meticulous technique to adequately debride the infected tissue, allow for continuous drainage, and prevent iatrogenic injury to critical neurovascular structures. The goal is complete evacuation of pus, removal of any necrotic tissue, and creation of a pathway for ongoing drainage, while minimizing functional loss.
Incision Planning
The choice of incision site is critical. Due to the thinner dorsal skin and the tendency for pus to point dorsally, a dorsal approach is almost universally preferred for initial drainage.
1. Dorsal Incision:
*
Location:
A longitudinal or gently curved incision is made on the dorsal aspect of the affected web space. The incision should be centered over the area of maximal tenderness and swelling. It generally lies just dorsal to the neurovascular bundles of the digits.
*
Orientation:
The incision should run parallel to the long axis of the metacarpals and fingers, avoiding transverse cuts across flexion creases that could lead to contracture. A "zigzag" or curvilinear incision can be considered to further minimize scar contracture, particularly in the critical thumb-index web space.
*
Length:
The incision should be adequate to allow for thorough exploration and drainage but no longer than necessary. Typically 1.5-3 cm in length.
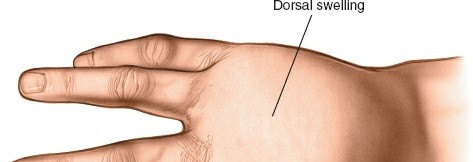
The following images illustrate the characteristic dorsal swelling and a dorsal incision for web space infection:
This illustration demonstrates the typical appearance of a web space infection, with significant dorsal edema and splaying of the adjacent digits, guiding the surgeon to the optimal location for a dorsal incision.
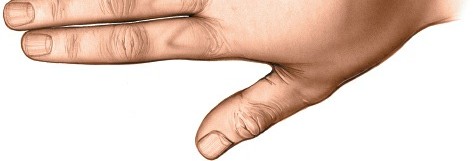
This image depicts a dorsal incision already made, showing the initial exposure of the underlying tissues during drainage of a web space infection.
2. Palmar Incision (Less Common, Counter-Incision):
* Direct palmar incisions are rarely used as the primary drainage route due to the thick palmar skin, dense fibrous septa, and the immediate proximity of vital neurovascular structures (common digital nerves and arteries) that are more superficially located volarly.
* However, a small palmar counter-incision may be used in conjunction with a dorsal incision (through-and-through drainage) for extensive, multiloculated abscesses or to facilitate drain placement. If used, it must be carefully placed longitudinally within the web, strictly avoiding the digital nerves and arteries, typically just volar to the metacarpal head.
Surgical Dissection and Drainage
The principle is to access the pus pocket, debride necrotic tissue, and ensure open drainage.
Step-by-step Dissection:
1.
Skin and Subcutaneous Tissue:
Incise the skin and subcutaneous tissue meticulously using a scalpel.
2.
Blunt Dissection:
Once through the skin, sharp dissection should be minimized. The use of a small, curved hemostat, scissors (e.g., Metzenbaum), or a blunt probe is preferred for spreading the tissues. This blunt technique helps to push away and protect neurovascular structures rather than transecting them.
3.
Identify and Protect Structures:
*
Dorsally:
Exercise caution to protect the dorsal sensory branches of the radial and ulnar nerves, and the dorsal digital arteries, which are relatively superficial.
*
Deep within the Web:
Bluntly spread the tissues deep into the web space. The web space abscess lies volar to the transverse metacarpal ligament and dorsal to the flexor tendon sheaths. The lumbrical muscle is typically found within this space.
*
Pus Localization:
Advance the blunt instrument cautiously until the pus pocket is entered. Pus will often egress under pressure.
4.
Abscess Exploration:
Once the abscess cavity is entered, use the hemostat or finger (if the incision allows) to gently explore the extent of the cavity, breaking down any loculations. This ensures complete drainage.
This image shows a surgical probe or hemostat carefully exploring the web space, indicating the depth of dissection required to adequately debride the abscess cavity and break down loculations.

*This illustration details blunt dissection using a hemostat, a critical technique to safely spread tissues and locate the abscess while protecting the delicate neurovascular bundles within the web space.*
*This intraoperative view likely depicts the identification and initial drainage of purulent material from within the web space.*

*This image may show a further stage of debridement or exploration, ensuring the entire infected compartment is addressed.*
- Pus Collection and Debridement: Collect a sample of the purulent material for Gram stain and aerobic/anaerobic cultures. Debride any obviously necrotic or devitalized tissue.
- Irrigation: Copiously irrigate the abscess cavity with sterile normal saline to flush out debris and reduce bacterial load.
-
Drainage Maintenance:
-
Packing: The wound should not be closed primarily. Loosely pack the entire cavity with sterile gauze (e.g., iodoform gauze or plain saline-moistened gauze). The packing serves to maintain an open wound for continuous drainage and to prevent premature skin closure. It also aids in wound healing by secondary intention.
This image shows the packing of the surgical wound with gauze after incision and drainage, a critical step to ensure continuous drainage and prevent premature closure of the abscess cavity. -
Penrose Drain: In larger or more complex cases, a small Penrose drain may be placed into the deep part of the cavity and brought out through one end of the incision (or a separate small counter-incision if a through-and-through approach is preferred, as seen in some practices). The drain should be secured with a single skin stitch.
This final image illustrates the appearance of the web space after surgical drainage and packing, showcasing the open wound management essential for resolution of the infection.
-
-
Dressing: Apply a sterile, bulky dressing over the packed wound.
After the tourniquet is deflated, assess for hemostasis. Any significant bleeding points should be addressed.
The hand is typically splinted in a functional position (intrinsic plus, see post-operative section) and elevated.
The image

is a general hand image, which might contextually represent the patient's hand post-surgery with dressings or splint, reinforcing the overall post-operative care.
Complications & Management
Despite meticulous surgical technique and appropriate post-operative care, complications can arise following the surgical management of web space infections. Early recognition and aggressive management are critical to mitigate long-term morbidity.
Common Complications
-
Spread of Infection:
- Incidence: Varies, but significant if initial drainage is incomplete or delayed. As noted, the lumbrical canals serve as direct conduits to the midpalmar space.
- Manifestations: Progression to midpalmar space infection, thenar space infection, flexor tenosynovitis (if it extends to a digital sheath), septic arthritis of the adjacent MCP joint, or osteomyelitis of the metacarpal head/phalangeal base. Systemic sepsis is the most severe systemic complication.
- Salvage Strategies: Immediate re-evaluation, including repeat clinical examination, inflammatory markers, and imaging (ultrasound, MRI). Requires aggressive re-exploration, wider debridement, repeat cultures, and adjustment of antibiotic regimen. Serial debridement may be necessary.
-
Neurovascular Injury:
- Incidence: Low with blunt dissection, but possible with sharp dissection or aggressive retraction.
-
Manifestations:
- Digital Nerves: Sensory deficit (anesthesia or paresthesia) in the adjacent fingers, formation of painful neuromas.
- Digital Arteries: Ischemia to the involved digit, non-healing wound, or even digital loss in severe cases (rare).
- Salvage Strategies: Meticulous surgical technique focusing on blunt dissection in deep layers. If a major digital nerve is transected, primary repair should be attempted if conditions allow (clean wound, minimal contamination). For arterial injury, microvascular repair may be necessary; otherwise, careful monitoring of digital viability is crucial. Neuroma excision with nerve grafting or transposition may be required for symptomatic neuromas.
-
Stiffness and Contracture:
- Incidence: Common, especially with prolonged immobilization, severe inflammation, or delayed treatment.
-
Manifestations:
- Web Space Contracture: Particularly of the first web space (thumb-index), leading to abduction deficit, but can occur in any interdigital web.
- Joint Stiffness: Restricted range of motion of the MCP and IP joints due to capsular contracture, adhesions, or prolonged splinting in non-functional positions.
- Tendon Adhesions: Limiting flexor or extensor tendon gliding.
- Salvage Strategies: Early and aggressive hand therapy is paramount. Dynamic splinting for web space widening or joint mobilization. Surgical release of contractures (e.g., Z-plasty, skin grafts, local flaps) may be required for severe, intractable web space contractures. Tenolysis or capsulectomy may be considered for severe stiffness.
-
Recurrent Infection:
- Incidence: Varies, often related to inadequate initial drainage, presence of unremoved foreign body, resistant organisms, or immunocompromised host.
- Manifestations: Recurrence of pain, swelling, purulent drainage, or systemic signs after initial improvement.
- Salvage Strategies: Re-exploration of the web space, repeat cultures (including fungal/mycobacterial if indicated), re-debridement, careful search for retained foreign bodies, and adjustment of antibiotic therapy based on new sensitivities.
-
Delayed Wound Healing:
- Incidence: Common in infected wounds left open for secondary intention.
- Manifestations: Persistent wound discharge, prolonged epithelialization, hypertrophic scarring.
- Salvage Strategies: Optimization of wound care, ensuring adequate debridement, nutritional support, and control of systemic factors (e.g., diabetes). Local wound care, negative pressure wound therapy (NPWT) in select cases, or surgical closure with skin grafting once the infection is fully resolved and the wound bed is healthy.
-
Disfiguring Scarring:
- Incidence: Inherent risk with surgical incisions, especially in areas of high tension or if wound healing is complicated.
- Manifestations: Hypertrophic or keloid scars, aesthetic concerns.
- Salvage Strategies: Scar massage, silicone sheeting, corticosteroid injections. Surgical scar revision may be considered after maturation of the scar.
Table: Common Complications of Web Space Infection Drainage
| Complication | Incidence (Qualitative) | Salvage Strategy |
|---|---|---|
| Spread of Infection | Uncommon if prompt I&D | - Urgent re-exploration and debridement |
| (Midpalmar, Tenar, FTS, | - Targeted systemic antibiotics based on cultures | |
| Osteomyelitis, Sepsis) | - Serial debridements if necessary | |
| Neurovascular Injury | Rare | - Meticulous blunt dissection technique |
| (Digital Nerves/Arteries) | - If nerve transected: Primary repair (if clean field) or consider nerve graft/neuroma excision | |
| - If artery injured: Microvascular repair (if feasible) or careful digital monitoring | ||
| Stiffness & Contracture | Common if prolonged immobility | - Early, guided hand therapy with active and passive range of motion |
| (Web Space, Joint, Tendon) | - Dynamic splinting for web space widening or joint mobilization | |
| - Surgical release (e.g., Z-plasty, skin grafts) for severe contractures | ||
| Recurrent Infection | Uncommon if complete I&D | - Re-exploration, debridement, repeat cultures |
| - Search for and remove foreign bodies | ||
| - Adjust antibiotic regimen based on new sensitivities | ||
| Delayed Wound Healing | Common | - Optimize local wound care (dressing changes, debridement) |
| - Address systemic factors (e.g., nutrition, diabetes control) | ||
| - Consider NPWT or eventual secondary closure/skin grafting after infection resolution | ||
| Disfiguring Scarring | Variable | - Scar massage, silicone sheeting, steroid injections |
| - Surgical scar revision (e.g., Z-plasty, W-plasty) after scar maturation |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of management for web space infections, crucial for restoring function, preventing stiffness, and minimizing long-term disability. The protocol generally progresses through phases, focusing on infection resolution, wound healing, pain control, edema management, and progressive motion.
Phase 1: Acute Inflammatory and Healing Phase (Days 0-7)
Goals:
* Control pain and edema.
* Prevent spread of infection.
* Maintain open drainage and facilitate wound healing.
* Prevent joint stiffness in non-infected areas.
Interventions:
*
Elevation:
The hand should be kept elevated above heart level at all times (e.g., on pillows when supine, in a sling with the hand higher than the elbow when ambulatory). This is critical for edema reduction.
*
Splinting:
A volar splint is typically applied to immobilize the wrist and prevent vigorous finger motion, while maintaining the MCP joints in 70-90 degrees of flexion and the IP joints in extension (the "intrinsic plus" or safe position). This position prevents collateral ligament shortening and maintains the optimal length of intrinsic muscles, minimizing the risk of joint contractures. For the affected web space, a small gauze roll or web space spacer can be gently placed in the web to prevent early contracture.
*
Wound Care:
Daily dressing changes are essential. If the wound was packed, the packing should be removed and replaced daily or every other day, with careful irrigation (e.g., saline) of the wound cavity. This facilitates ongoing drainage, prevents premature skin closure, and promotes healing by secondary intention. Monitor for signs of persistent infection or complications.
*
Pain Management:
Administer appropriate analgesia (oral or intravenous) to ensure patient comfort and facilitate compliance with elevation and early gentle mobilization.
*
Antibiotics:
Continue the prescribed intravenous antibiotics, transitioning to oral antibiotics based on culture sensitivities and clinical improvement. Close monitoring of inflammatory markers (CRP, ESR) and clinical signs (fever, pain, erythema) is important.
Phase 2: Early Mobilization and Scar Management (Weeks 1-4)
Goals:
* Initiate controlled active range of motion (AROM).
* Begin scar management.
* Continue to reduce edema.
* Prevent web space contracture.
Interventions:
*
Active Range of Motion (AROM):
Once acute pain and swelling subside, and the wound shows signs of healthy granulation, gentle AROM exercises for the wrist and digits should commence, typically under the guidance of a hand therapist. This includes individual finger flexion and extension, fist making, and thumb opposition. Avoid passive motion initially if there is still significant inflammation or pain.
*
Edema Control:
Continue elevation and consider compressive garments or gentle retrograde massage as tolerated.
*
Scar Management:
Once the wound has closed or is progressing well with granulation tissue, scar massage (e.g., with lanolin-based creams) can be initiated to soften the scar tissue and prevent adhesions. Silicone gel sheets or scar pads may be introduced to flatten and soften hypertrophic scars.
*
Splinting Adjustment:
The static intrinsic plus splint may be continued at night or for protection during activities. Dynamic splints or web space conformers (e.g., custom-molded silicone or thermoplastic spacers) may be fabricated to specifically address or prevent web space contractures, especially in the first web.
*
Progressive Activities:
Gradually increase the duration and intensity of therapeutic exercises.
Phase 3: Strengthening and Functional Integration (Weeks 4-12+)
Goals:
* Achieve full, pain-free range of motion.
* Improve grip and pinch strength.
* Optimize functional use of the hand.
* Return to work/sport specific activities.
Interventions:
*
Progressive Strengthening:
Introduce gentle strengthening exercises using therapy putty, resistance bands, and light weights. Focus on grip strength, pinch strength (tip, lateral, palmar), and intrinsic muscle strengthening.
*
Advanced Range of Motion:
Progress to more aggressive passive range of motion (PROM) as needed to address residual stiffness, always respecting tissue tolerance. Joint mobilization techniques may be employed by the therapist.
*
Functional Activities:
Incorporate activities that mimic daily living, work, or sport-specific tasks to improve dexterity, coordination, and endurance.
*
Sensory Re-education:
If there was any nerve involvement or residual altered sensation, sensory re-education exercises may be beneficial.
*
Return to Activity:
Gradually progress towards full return to normal activities, work, or sports, guided by the patient's functional recovery and tolerance. Education on injury prevention and hygiene is reinforced.
Throughout all phases, close collaboration between the orthopedic surgeon, hand therapist, and patient is crucial for optimal outcomes. Regular re-assessment of pain, edema, wound status, range of motion, and strength guides the progression through the rehabilitation protocol.
Summary of Key Literature / Guidelines
The effective management of web space infections is guided by established principles in hand surgery, primarily emphasizing early diagnosis and aggressive surgical drainage complemented by appropriate antimicrobial therapy and rehabilitation.
-
Fundamental Principles of Hand Infection Management: Standard hand surgery texts, such as Green's Operative Hand Surgery , Campbell's Operative Orthopaedics , and specialized infection manuals, universally advocate for timely incision and drainage of abscesses as the definitive treatment. They highlight that antibiotics alone are insufficient for pus collections. This principle is paramount for web space infections.
-
Anatomical Considerations: The literature consistently emphasizes the unique anatomy of the hand, particularly the fascial planes and potential for infection spread. Studies by Koch and Mason in the early to mid-20th century elucidated the deep spaces of the hand and their communications, which remain fundamental to understanding web space infections. The communication via the lumbrical canals into the midpalmar space is a critical anatomical consideration underscored in all authoritative sources, explaining the propensity for proximal spread if neglected.
-
Microbiology and Antibiotics: Consensus guidelines, often disseminated by organizations like the Infectious Diseases Society of America (IDSA) or the American Society for Surgery of the Hand (ASSH), recommend empiric broad-spectrum antibiotic coverage initially, targeting Staphylococcus aureus (including MRSA) and Streptococci, especially considering the rising prevalence of community-acquired MRSA. Subsequent adjustment based on culture and sensitivity results is standard practice. The literature supports the use of intravenous antibiotics in the acute phase, transitioning to oral therapy upon clinical improvement.
-
Surgical Technique: The preference for a dorsal longitudinal or gently curvilinear incision for web space abscess drainage is well-documented. This approach capitalizes on the thinner dorsal skin and avoids crucial neurovascular structures that are more superficially located volarly. The importance of blunt dissection to protect these structures and thorough exploration to break down loculations is consistently stressed in surgical technique descriptions. The practice of leaving the wound open to heal by secondary intention, often with loose packing or a drain, is standard to ensure continuous drainage and prevent recurrence.
-
Role of Imaging: The utility of ultrasound as a first-line imaging modality to differentiate cellulitis from abscess and guide drainage is increasingly recognized and supported in the literature. Studies have shown its high sensitivity and specificity for identifying fluid collections in soft tissue infections of the hand, thereby reducing unnecessary surgical explorations or delayed interventions. MRI is reserved for complex cases or when deeper spread or osteomyelitis is suspected, offering superior soft tissue and bone detail.
-
Prevention of Complications: Literature reviews and clinical studies consistently highlight the importance of early diagnosis and intervention in preventing severe complications such as extensive deep space spread, osteomyelitis, septic arthritis, and permanent digital stiffness or contracture. The risk of web space contracture, particularly in the first web, and joint stiffness are significant concerns, prompting emphasis on early hand therapy and appropriate splinting protocols in the post-operative period.
-
Rehabilitation: The integral role of post-operative hand therapy is universally supported. Protocols typically follow a phased approach, commencing with edema and pain control, progression to controlled active range of motion in safe positions (e.g., intrinsic plus), and eventually strengthening and functional integration. This structured rehabilitation is critical for achieving optimal functional outcomes and mitigating long-term disability.
In summary, the management of web space infections integrates a robust understanding of hand anatomy, aggressive surgical principles of abscess drainage, targeted antimicrobial stewardship, and comprehensive post-operative rehabilitation. Adherence to these guidelines, as summarized across key literature, is essential for minimizing morbidity and preserving hand function.
You Might Also Like