Surgical Management of Patellofemoral Instability and Dislocation
Key Takeaway
Surgical intervention for patellar dislocation is dictated by the underlying pathoanatomy. Acute operative indications include osteochondral fractures and loose bodies. For recurrent instability, procedures range from medial patellofemoral ligament (MPFL) reconstruction to distal tibial tubercle osteotomies. Successful outcomes rely on correcting specific anatomical deficits, such as abnormal tibial tubercle-trochlear groove (TT-TG) distances, while avoiding complications like medial overtightening or physeal arrest in pediatric patients.
INTRODUCTION TO PATELLOFEMORAL SURGERY
The surgical management of patellofemoral instability represents one of the most complex and nuanced domains in operative orthopaedics. The patellofemoral joint relies on an intricate interplay of static osseous geometry, passive ligamentous restraints, and dynamic muscular forces. When this delicate balance is disrupted—whether through an acute traumatic event or chronic anatomical malalignment—the resulting instability can lead to profound functional impairment, apprehension, and progressive chondral degeneration.
Historically, more than 100 surgical procedures have been described for the treatment of patellofemoral instability, reflecting both the complexity of the joint and the historical lack of consensus on a single "gold standard" procedure. Today, the paradigm has shifted toward an à la carte approach. The key to successful surgical intervention is correctly identifying and treating the specific pathological anatomy producing the instability. No single operation is universally successful; rather, the complexity of the procedure chosen must be precisely matched to the problem identified, focusing on reproducible, low-risk, high-reward techniques with historically high success rates.
ACUTE PATELLAR DISLOCATION
While the majority of first-time, acute patellar dislocations are managed nonoperatively with a brief period of immobilization followed by aggressive physical therapy, specific clinical scenarios mandate early surgical intervention.
Indications for Acute Operative Intervention
Operative intervention for an acute, first-time patellar dislocation is strictly indicated in the presence of:
1. Osteochondral Fracture: Often occurring as the medial facet of the patella impacts the lateral femoral condyle during dislocation or reduction.
2. Loose Body Formation: Intra-articular fragments that act as mechanical blocks or third-body wear particles.
3. Joint Incongruity: Significant disruption of the articular surface requiring anatomical reduction and internal fixation.
4. Elite Athletic Status: Surgery may be indicated for competitive athletes at or near the end of their season if they plan to pursue high-level athletic activities without the unacceptable risk of recurrent instability during critical competition.
Biomechanics and Pathoanatomy of Acute Dislocation
Studies utilizing advanced cadaveric models have definitively established that the Medial Patellofemoral Ligament (MPFL) is the primary passive restraint against lateral patellar translation, providing 50% to 60% of the restraining force from 0 to 30 degrees of knee flexion. The patellotibial and patellomeniscal ligaments act as secondary stabilizers.
In the setting of an acute lateral patellar dislocation, the MPFL is almost universally injured. A tear of the MPFL off its femoral origin (near the adductor tubercle and Schöttle's point) is highly frequent. Furthermore, this injury is often accompanied by the partial disruption of the vastus medialis obliquus (VMO), characterized by the ripping away of the muscle fibers from the adductor magnus tendon.
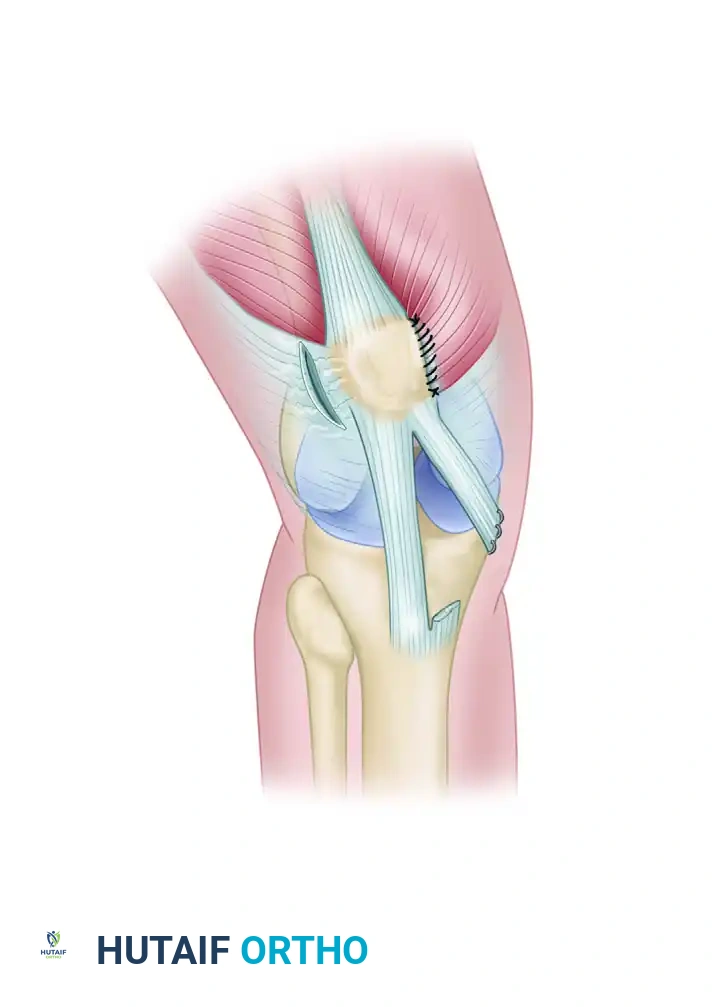
Surgical Technique: Acute MPFL and VMO Repair
When acute repair is indicated, the procedure focuses on restoring the native anatomy before chronic tissue retraction and scarring occur.
- Patient Positioning: The patient is positioned supine on the operating table. A well-padded tourniquet is applied to the proximal thigh. The operative leg is prepped and draped free to allow full range of motion during the procedure.
- Incision and Dissection: A small (approximately 4 cm) longitudinal incision is centered over the adductor tubercle and the medial epicondyle of the femur. Dissection is carried down through the subcutaneous tissue to the deep fascia.
- Identification of Pathology: The hematoma is evacuated. The avulsed edge of the MPFL and the disrupted distal fibers of the VMO are identified.
- Anatomical Repair: The MPFL is repaired back to its anatomical femoral footprint using suture anchors. The VMO is meticulously repaired to the adductor magnus tendon and the medial intermuscular septum using heavy, non-absorbable sutures.
- Dynamic Assessment: The knee is cycled through a full range of motion to ensure the repair is isometric, stable, and does not over-constrain the patella in flexion.
Clinical Pearl: Accelerated rehabilitation with no immobilization is highly recommended following acute MPFL/VMO repair. Early, controlled range of motion is critical to prevent postoperative arthrofibrosis, which is a devastating complication in patellofemoral surgery.
PATELLOFEMORAL MALALIGNMENT AND RECURRENT SUBLUXATION
If dislocation of the patella continues despite appropriate and exhaustive nonoperative treatment (including core, gluteal, and VMO strengthening), surgical intervention is indicated.
The Pathophysiology of Chronic Instability
Without surgical stabilization, the patient often develops profound apprehension, becoming afraid to use the knee in daily activities. With continued recurrence, the joint may be severely and irreversibly damaged.
The progressive deterioration of the knee joint in recurrent instability is multifactorial, driven by:
* Abnormal patellofemoral articulation
* Abnormal quadriceps pull (increased Q-angle)
* Osteochondral free fragments
* Chondromalacia of the patella
* Meniscal tears and secondary degeneration
Surgical Warning: With recurrent dislocation of the patella, the articulating surfaces degenerate not so much because the patella is sometimes or often dislocated, but because the excursions of the patella are abnormal during any motion of the knee. Chronic maltracking causes repetitive microtrauma and shear stress to the articular cartilage, leading to early-onset osteoarthritis.
Preoperative Evaluation and Decision Making
The physical and imaging examinations must provide ample information for determining the specific anatomical areas that require surgical treatment. Advanced imaging (MRI and CT) is utilized to quantify the Tibial Tubercle-Trochlear Groove (TT-TG) distance, assess patellar height (Caton-Deschamps index for patella alta), and evaluate trochlear dysplasia (Dejour classification).
SURGICAL PROCEDURES FOR RECURRENT INSTABILITY
During all operative procedures for recurrent dislocation or subluxation of the patella, a thorough arthroscopic inspection of the articular surfaces and intraarticular structures is mandatory. This diagnostic step dictates the final surgical strategy.
The "Three-in-One" Procedure (Proximal and Distal Soft Tissue Realignment)
For patients with recurrent instability without severe underlying bony malalignment (e.g., normal TT-TG distance), soft tissue realignment procedures are utilized. The classic "Three-in-One" procedure combines lateral decompression with medial tightening and distal soft-tissue vector realignment.
Surgical Steps of the Three-in-One Procedure:
* (A) Lateral Release: The lateral retinaculum is released to decompress the lateral facet and allow the patella to centralize. Care must be taken to preserve the superior lateral geniculate artery to prevent patellar avascular necrosis.
* (B) Vastus Medialis Muscle Advancement: The VMO is mobilized and advanced distally and laterally over the patella, increasing its dynamic medializing force during terminal extension.
* (C) Transfer of the Medial Third of the Patellar Tendon: The medial third of the patellar tendon is sharply detached from the tibial tubercle, routed medially, and sutured to the medial collateral ligament (MCL) or the medial tibia using two metal or biocomposite suture anchors. This alters the distal pull vector, tethering the patella against lateral subluxation.
Distal Realignment: Tibial Tubercle Osteotomy (TTO)
When the primary pathology is an abnormal lateralization of the tibial tubercle (TT-TG > 20 mm) or severe patella alta, a bony distal realignment is required.
Anteromedialization (Fulkerson Osteotomy)
Symptomatic chondral changes inferiorly and laterally can be significantly improved by anteromedialization of the tibial tuberosity. By cutting the tibial tubercle on an oblique plane (typically 45 to 60 degrees) and translating it anteriorly and medially, the surgeon achieves two goals:
1. Medialization: Corrects the abnormal TT-TG distance, realigning the extensor mechanism vector.
2. Anteriorization: Elevates the patella, transferring the compressive stress proximally and medially, thereby unloading the damaged inferior and lateral facets.
Pitfall: Symptomatic chondral changes of the medial facet are exacerbated by overtightening medially or excessive medialization of the tubercle. If a patient has isolated medial facet arthrosis, medializing procedures must be used with extreme caution or avoided entirely.
Absolute Contraindications for Bony Realignment
CRITICAL WARNING: Procedures that involve transplantation or osteotomy of the tibial tuberosity are strictly contraindicated until the proximal tibial physis has completely closed.
Performing a tibial tubercle osteotomy in a skeletally immature patient risks premature closure of the anterior portion of the proximal tibial physis. Because the posterior physis continues to grow, this iatrogenic arrest leads to a progressive genu recurvatum deformity, which is highly morbid and requires complex corrective osteotomies (e.g., opening wedge proximal tibial osteotomy) to resolve. In pediatric patients with open physes, surgeons must rely exclusively on soft-tissue procedures, such as MPFL reconstruction utilizing hamstring autograft routed avoiding the femoral physis, or Roux-Goldthwait procedures.
POSTOPERATIVE REHABILITATION PROTOCOLS
The success of any patellofemoral stabilization procedure is heavily dependent on the postoperative rehabilitation protocol. The goals are to protect the surgical repair, restore normal joint kinematics, and prevent arthrofibrosis.
Phase I: Maximum Protection (Weeks 0-4)
* Weight-bearing: Typically weight-bearing as tolerated (WBAT) in a hinged knee brace locked in extension for soft tissue procedures. For TTOs, partial weight-bearing (e.g., 50%) may be indicated until early radiographic consolidation is noted.
* Range of Motion (ROM): Early, controlled ROM is initiated immediately. For MPFL repairs/reconstructions, ROM is usually permitted from 0 to 90 degrees to prevent stiffness without overstretching the medial repair.
* Muscle Activation: Immediate initiation of quadriceps sets, straight leg raises (in the brace), and core strengthening.
Phase II: Moderate Protection and ROM Restoration (Weeks 4-8)
* Bracing: The brace is gradually unlocked and eventually discontinued once the patient demonstrates good quadriceps control without an extensor lag.
* ROM: Progression to full, symmetrical range of motion.
* Strengthening: Introduction of closed kinetic chain exercises (e.g., mini-squats, leg presses) focusing on VMO activation and gluteal strengthening to control femoral internal rotation.
Phase III: Advanced Strengthening and Return to Play (Weeks 8-16+)
* Progression to sport-specific drills, plyometrics, and agility training.
* Return to competitive sports is typically permitted between 4 to 6 months postoperatively, contingent upon the restoration of 90% or greater limb symmetry index (LSI) on functional testing and the complete absence of apprehension.
CONCLUSION
The surgical treatment of patellar dislocation requires a meticulous, individualized approach. Whether addressing an acute MPFL avulsion in an elite athlete or executing a complex distal realignment for chronic maltracking, the orthopaedic surgeon must deeply understand patellofemoral biomechanics. By matching the correct procedure to the specific pathoanatomy—and rigorously avoiding pitfalls such as medial overtightening or physeal injury—surgeons can reliably restore stability, alleviate apprehension, and protect the patellofemoral joint from progressive degeneration.
You Might Also Like
