Patellar Fracture ORIF: An Intraoperative Masterclass in Tension Band Wiring
Key Takeaway
Welcome, fellows, to a deep dive into patellar fracture ORIF. Today, we'll meticulously explore the anatomy, preoperative planning, and step-by-step intraoperative execution of tension band wiring. We'll cover crucial surgical techniques, potential pitfalls, and comprehensive postoperative care, ensuring you master this essential procedure for restoring knee extensor mechanism integrity and articular congruence.
Introduction to Patellar Fracture Management: A Masterclass Overview
Good morning, fellows. Let's scrub in. Today, we're tackling a patellar fracture, a common injury that, if not managed meticulously, can severely compromise knee function. Our goal, as always, is to restore the extensor mechanism's integrity and achieve an anatomically congruent articular surface. This is not just about fixing a bone; it's about preserving the intricate biomechanics of the knee.
Comprehensive Surgical Anatomy of the Patella
First, let's refresh our understanding of the patella and its surrounding structures. The patella, the largest sesamoid bone in the body, is truly a marvel of biomechanical engineering. It's embedded within the quadriceps tendon, acting as a fulcrum to significantly increase the moment arm of the extensor mechanism, particularly crucial during terminal knee extension when the quadriceps would otherwise be at a mechanical disadvantage.
- Blood Supply: Remember, the patella receives its blood supply from a rich peripatellar plexus, with the main intraosseous supply typically running in a distal-to-proximal direction. This network is derived from multiple arteries around the knee, including branches from the genicular arteries. While robust, severe comminution or extensive soft tissue stripping can compromise this supply, increasing the risk of avascular necrosis.
- Articular Surface: On its posterior aspect, the patella presents a highly specialized articular surface, composed of medial and lateral facets. The medial facet, notably, exhibits the most variability in size and shape. Subtle horizontal ridges further subdivide these facets. Most medially, we find the "odd facet," which articulates primarily in deep flexion. Importantly, the distal pole of the undersurface is extra-articular. This distinction is vital for understanding fracture patterns and reduction goals.
- Fellows, observe: The portion of the patella articulating with the femur shifts from distal to proximal with increasing degrees of flexion. This explains why the fracture pattern from direct blows often corresponds to the articulating portion of the patella at the time of injury, directly correlating with the amount of knee flexion.
- Extensor Mechanism Attachments:
- The superior pole (base) serves as the primary attachment for the quadriceps tendon. The most superficial fibers of the quadriceps tendon actually course over the anterior patellar surface, becoming contiguous with the patellar tendon.
- The inferior pole (apex) is the origin of the patellar tendon, which then courses distally to insert on the tibial tubercle.
- Patellar Retinaculum: This critical structure is formed by thickenings of the fascia lata of the thigh, fused with the aponeuroses of the vastus medialis and lateralis. Beyond its role in stabilizing the patella, the retinaculum acts as a secondary extensor. Its integrity is paramount; disruption allows hematoma to escape the joint capsule and can lead to significant extensor lag.
- Neurovascular Risks: While direct neurovascular injury during patellar ORIF is uncommon given its superficial location, we must always be mindful of the infrapatellar branch of the saphenous nerve. This sensory nerve crosses the surgical field, particularly with transverse incisions, and is susceptible to iatrogenic injury, leading to an area of numbness or dysesthesia over the anteromedial knee. While generally a nuisance rather than a functional deficit, patient satisfaction demands we minimize this risk.
Pathogenesis and Fracture Classification
Patellar fractures arise from either direct force to the anterior knee (e.g., dashboard injury in an MVA), indirect forces transmitted through the extensor mechanism (e.g., sudden, unanticipated knee flexion against a powerfully contracting quadriceps), or a combination. Indirect mechanisms tend to result in less comminuted fractures.
Common descriptive terms classify these fractures: stellate or comminuted, transverse, vertical, apical or inferior pole, and sleeve fractures. Our approach today, tension band wiring, is particularly effective for transverse patterns, or those that can be converted to a transverse pattern.
Clinical Presentation and Diagnostic Workup
When a patient presents with a suspected patellar fracture, a thorough evaluation is essential.
Patient History and Physical Findings
- History: Elicit the mechanism of injury. High-energy direct trauma (e.g., head-on MVA) often correlates with associated injuries to the knee or even the distal femur and acetabulum due to force transmission through a flexed knee.
- Physical Examination:
- Palpation: Often, a palpable defect in the patella is present, especially with displaced fractures.
- Effusion: A new onset of joint effusion post-injury typically signifies an intra-capsular injury. However, if the retinaculum is significantly disrupted, hematoma may extravasate, leading to a less pronounced effusion.
- Extensor Function: Pain can severely limit the assessment of active knee extension or extensor lag. In such cases, aspiration of the hematoma and injection of local anesthetic can facilitate a more accurate assessment. Always note any extravasation of local anesthetic, as this can indicate an intra-articular extension of skin defects, a crucial finding for open fractures.
- Associated Injuries: Always perform a thorough secondary survey. Check peripheral pulses and neurologic function. Evaluate knee stability – patellar fractures can be accompanied by cruciate ligament or meniscal injuries.
- Patella Alta/Baja: The Insall-Salvati ratio (height of the patella over the distal from the inferior pole to the tibial tubercle) is normally around 1.0. Values less than 1.0 suggest patella alta, potentially indicating a patellar tendon rupture or, in pediatrics, a patellar sleeve fracture.
Imaging and Other Diagnostic Studies
- Radiographs: Standard anteroposterior (AP) and lateral views of the knee are indispensable. An axial view of the patella, such as the Merchant view, is critical for assessing articular step-off and displacement, particularly in the trauma setting where it's often best tolerated.

* Fellows, note: A Merchant view is crucial for assessing congruence.
* Aspiration: If an effusion is present, aspiration can provide diagnostic information. The presence of fat lobules in the syringe is pathognomonic for an intra-capsular fracture.
Differential Diagnosis
It's important to distinguish patellar fractures from other conditions:
* Quadriceps rupture
* Patellar tendon rupture
* Bipartite patella: This developmental anomaly, resulting from failed fusion of ossification centers, can be mistaken for a fracture. Bipartite patellae are typically superolateral, more common in males, and bilateral in 40% of cases. They have sclerotic margins, unlike acute fractures.

* Fellows, examine this image: Note the classic superolateral position and sclerotic margins of a bipartite patella.
* Ligamentous or meniscal injury
* Distal femur or tibial plateau fracture
* Inflammatory or septic arthritis
* Osteochondral injury
* Patellar dislocation or retinacular injury
Nonoperative vs. Operative Management: Decision Making
The decision for operative intervention is critical and hinges on specific criteria.
Nonoperative Management Criteria
Nonoperative management is reserved for a select group of patients whose fractures meet all of the following strict criteria:
* No associated extensor mechanism disruption: The patient must be able to actively extend the knee against gravity, indicating an intact extensor mechanism.
* Minimal displacement: Less than 2 mm of articular surface displacement or less than 3 mm separation of fracture fragments. Some authors tolerate even less displacement for transverse fractures.
* Intact retinaculum: If the retinaculum is intact, it acts as a secondary extensor, potentially allowing for non-operative treatment even with some fracture displacement.
Our preferred nonoperative protocol involves partial weight-bearing with crutches and a hinged knee brace. The leg is maintained in extension for 2 weeks, then progressively advanced to 0-45 degrees of flexion for 2 weeks, 0-90 degrees for another 2 weeks, followed by full motion for 2 weeks. Full weight-bearing is allowed after this 8-week course. While generally successful for appropriate fractures, loss of flexion remains the most common complication.
Surgical Management Indications
Operative treatment is the preferred course for the vast majority of patellar fractures that do not meet the stringent nonoperative criteria. This includes:
* Displaced fractures (greater than 2mm articular step-off or 3mm fragment separation).
* Disruption of the extensor mechanism, evidenced by an inability to actively extend the knee.
* Open fractures, which require urgent operative debridement and fixation to minimize infection risk.
* Fractures with significant comminution that would lead to unacceptable incongruity without fixation.
The primary goals of operative management are anatomic reconstruction of the articular surface and restoration of the extensor mechanism.
Preoperative Planning and Patient Positioning
Before we make any incision, meticulous planning is paramount.
Operative Timing
Timing is dictated by the patient's overall condition, the presence of open fractures (urgent), and the condition of the soft tissues. Swollen, compromised soft tissues may necessitate a delay for swelling reduction.
Patient Positioning
We'll place our patient in the supine position on a radiolucent operating table. This allows for unrestricted fluoroscopic imaging throughout the procedure.
- Tourniquet Placement: A tourniquet is essential for a bloodless field, crucial for identifying fracture fragments and achieving precise reduction. It must be placed as proximally as possible on the thigh.
> SURGICAL WARNING: Ensure the quadriceps muscle belly is not trapped under the tourniquet. If it is, inflation can cause superior retraction of the proximal patellar fragment, making reduction significantly more challenging.- Technique: Flex the knee to 90 degrees before elevating the tourniquet. If the retinaculum is disrupted and the superior patella is high-riding, gently pull the quadriceps distally to reduce the patella before inflating the tourniquet. Inflate the tourniquet to a standard pressure (e.g., 250-300 mmHg or 100 mmHg above systolic blood pressure).
- Fluoroscopy Setup: The C-arm should be positioned to allow for both AP and lateral views of the knee without repositioning the patient. Ensure the image intensifier can be brought into the field easily and draped sterilely.
- Examination Under Anesthesia (EUA): This is a critical step, fellows. Before prepping and draping, perform a thorough EUA. Pain often limits assessment preoperatively. Check for coexisting ligamentous injuries (Lachman, pivot shift, posterior drawer, varus-valgus stress testing). This ensures we don't miss any associated pathology that might require concomitant management.
Surgical Approach
For patellar fractures, we have a choice between longitudinal and transverse incisions.
- Incision Choice:
- A transverse approach follows skin lines and may offer a cosmetic advantage. It also minimizes the risk of injury to the infrapatellar branch of the saphenous nerve.
- However, our preference is typically a longitudinal approach. Why? It provides superior exposure, especially for complex or comminuted fractures, and allows for easy extension distally to the tibial tubercle if wire augmentation or a patellar tendon repair is required. Furthermore, a longitudinal incision is often better tolerated for future reconstructive surgeries, which can be a consideration in elderly patients or those with pre-existing osteoarthritis.
- Soft Tissue Management: Remember, the patella has only a thin soft tissue envelope covering it. Handle all soft tissues with extreme care. This care begins in the emergency department – ensure splints or immobilizers are copiously padded to prevent pressure sores, which can compromise the surgical field.
Incision and Exposure
- Skin Incision: With the tourniquet inflated and the leg prepped and draped in a sterile fashion, make a longitudinal skin incision directly over the anterior aspect of the patella. Extend it sufficiently proximally and distally to ensure adequate exposure of both fracture fragments.
- Subcutaneous Dissection: Carefully dissect through the subcutaneous tissues. You'll encounter the patellar bursa immediately deep to the skin.
- Bursotomy and Hematoma Evacuation: Incise the patellar bursa. As you open it, you'll almost certainly encounter a significant hematoma. This is expected. Use copious irrigation with saline and small curettes to meticulously clear the hematoma and any debris from the fracture site. A clear view of the fracture surfaces is paramount for accurate reduction.
- Retinacular Assessment: Follow the fracture line out to the retinacular tissue. You'll identify the superior and inferior leaves of the retinaculum.
> SURGICAL PEARL: Tag these retinacular leaves with absorbable sutures (e.g., 2-0 Vicryl) for later repair. This not only aids in re-approximation but also helps in maintaining the reduction during the initial stages of fixation.
Intraoperative Execution: Open Reduction and Internal Fixation (Tension Band Wiring)
Today, fellows, we'll focus on the tension band wiring technique, which is excellent for stabilizing transverse fracture patterns. For more complex comminuted fractures, we may first convert them to a transverse pattern by fixing smaller pieces with screws or Kirschner wires before applying the tension band. This construct can also be adapted for distal pole fractures by placing the Kirschner wires closer together to capture the fragment effectively.
Step 1: Fracture Assessment and Initial Debridement
- Once the fracture site is exposed and cleared of hematoma, thoroughly inspect the fracture fragments. Remove any small, non-viable articular fragments without attached subchondral bone. These pieces, if left, can act as a nidus for post-traumatic arthritis.
- Gently reduce any depressed articular fragments using a Freer elevator or a small dental pick. Our goal is a perfectly smooth articular surface.
> SURGICAL PEARL: Palpate the articular surface directly with your gloved finger or a Freer elevator to ensure anatomic reduction. This tactile feedback is often more reliable than visual inspection alone for detecting subtle step-offs.
Step 2: Temporary Fracture Reduction and Fixation
- Reduce the Main Fragments: Carefully bring the main proximal and distal fragments into anatomic alignment. This often requires significant traction on the quadriceps mechanism and counter-traction on the patellar tendon.
- Apply Reduction Clamps: Once reduced, hold the fracture in place with patellar reduction clamps or Weber clamps. These clamps provide stable temporary fixation, freeing your hands for hardware placement.

* Fellows, observe: The Weber clamp maintains reduction while we prepare for K-wire insertion.
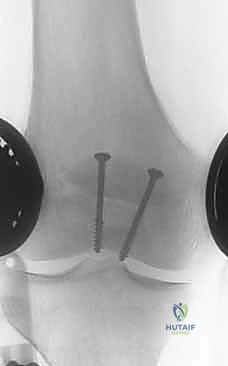
Step 3: Kirschner Wire (K-wire) Placement
We will use two 1.6 to 2.0 mm Kirschner wires to span the fracture in parallel.
- Entry Point and Trajectory:
- Retrograde: You can introduce the K-wires through the fracture site into the proximal fragment first.
- Antegrade: Alternatively, introduce them into the distal fragment in an antegrade fashion.
- Our approach: For this transverse fracture, we'll start antegrade. Position the first K-wire parallel to the anterior surface of the patella, aiming for its central axis.
- Initial Advancement: Advance the K-wire until its tip is flush with the fracture line. Confirm your reduction one final time.
- Cross the Fracture: Now, with the fracture reduction held firmly by the clamps, advance the K-wire across the fracture line and into the opposite fragment.

* Fellows, see how the K-wire crosses the fracture.
4. Second K-wire: Repeat this process for the second K-wire, ensuring it is parallel to the first and spaced appropriately to provide a stable construct.

* Here, both K-wires are in place, providing initial stability.
5. Depth Control: Ideally, the Kirschner wires should be positioned approximately 5 mm below the anterior surface of the patella. This ensures they are subcortical but not so superficial as to risk skin irritation.
> SURGICAL WARNING: Avoid penetrating the articular surface with your K-wires. Use fluoroscopy to confirm appropriate placement and depth. A lateral fluoroscopic view is invaluable here.
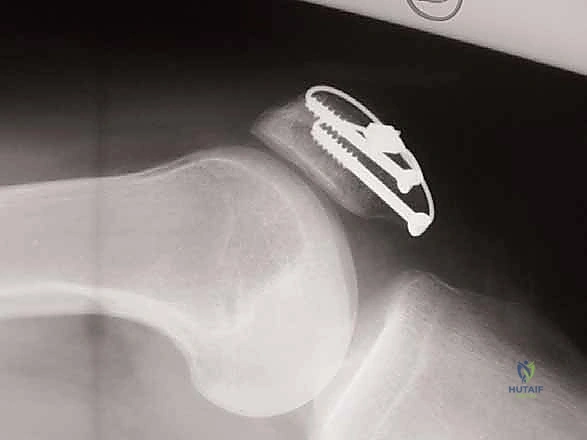
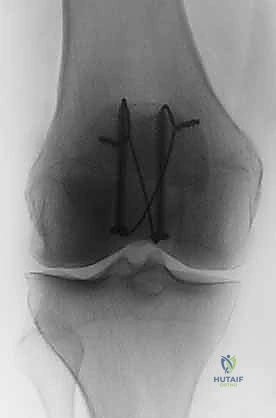
Step 4: Cerclage Wire Passage (Tension Band Application)
Now we'll apply the cerclage wire, which converts the tensile forces on the anterior patella into compressive forces at the articular surface.
- Superior Pole Wire Placement: Take a 1.0 mm thick cerclage wire. Pass it just deep to the Kirschner wires, abutting the superior pole of
Additional Intraoperative Imaging & Surgical Steps































REFERENCES
-
Functional outcomes after long-term follow-up of tension band wiring have been reported to be the same as age-matched standards. 15
-
Atkison PJ, Haut RC. Injuries produced by blunt trauma to the human patellofemoral joint vary with flexion angle of the knee. J Orthop Res 2001;19:827–833.
-
Benjamin J, Bried J, Dohm M, et al. Biomechanical evaluation of various forms of fixation of transverse patellar fractures. J Orthop Trauma 1987;1:219–222.
-
Bostrum A. Fracture of the patella: a study of 422 patellar fractures. Acta Orthop Scand Suppl 1972;143:3–80.
-
Braun W, Wiedemann M, Ruter A. Indications and results of nonoperative treatment of patellar fractures. Clin Orthop Relat Res 1993;289:197–201.
-
Carpenter JE, Kasman R, Matthews LS. Fractures of the patella. J Bone Joint Surg Am 1993;75A:1550–1561.
-
Edwards B, Johnell O, Redlund-Johnell L. Patellar fractures: a 30year follow-up. Acta Orthop Scand 1989;60:712–714.
-
Green WT. Painful bipartite patellae: a report of three cases. Clin Orthop Relat Res 1975;110:197–200.
-
Insall J, Goldberg V, Salvati E. Recurrent dislocation of the highriding patella. Clin Orthop Relat Res 1972;88:67–69.
-
Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am 1971;53A:1551–1560.
-
Matthews LS, Sonstegard DA, Henke JA. Load-bearing characteristics of the patellofemoral joint. Acta Orthop Scand 1977;48:511–516.
-
Merchant AC, Mercer RL, Jacobsen RH, et al. Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am 1974; 56A:1391–1396.
-
Nerlich M, Weigel B. Patella. In: Ruedi TP, Murphy WM, eds. AO Principles of Fracture Management. New York: Thieme, 2000: 487–501.
-
Reider B, Marshall JL, Koslin B, et al. The anterior aspect of the knee joint: an anatomical study. J Bone Joint Surg Am 1981;63A: 351–356.
-
Scapinelli R. Blood supply of the human patella: its relation to ischaemic necrosis after fracture. J Bone Joint Surg Br 1967;49B: 563–570.
-
Schemitsch EH, Weinberg J, McKee MD, et al. Functional outcome of patella fractures following open reduction and internal fixation. J Orthop Trauma 1999;13:279.
-
Smith ST, Cramer KE, Karges DE, et al. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997; 11:183–187.
-
Torchia ME, Lewallen DG. Open fractures of the patella. J Orthop Trauma 1996;10:403–409.
-
Wilber JH. Patellar fractures: open reduction internal fixation. In: Wiss DA, ed. Master Techniques in Orthopaedic Surgery: Fractures. Philadelphia: Lippincott Williams & Wilkins, 1998:335–346.
You Might Also Like

