Surgical Anatomy and Biomechanics of the Wrist: A Comprehensive Masterclass
Key Takeaway
The human wrist is a highly complex biomechanical interface comprising the distal radioulnar, radiocarpal, and midcarpal joints. Mastery of its intricate osteology, intrinsic and extrinsic ligamentous architecture, and unique vascular supply is paramount for orthopedic surgeons. This guide details the critical surgical anatomy, kinematic principles, and operative approaches necessary for managing complex carpal fractures, ligamentous instabilities, and degenerative conditions.
INTRODUCTION TO WRIST OSTEOLOGY AND ARTICULATIONS
The wrist is an extraordinarily complex anatomical region serving as the foundational kinematic link between the forearm and the hand. For the purposes of advanced surgical intervention, the wrist is defined as encompassing the distal radioulnar joint (DRUJ), the radiocarpal joint, the ulnocarpal articulation, and the midcarpal joint. It comprises eight carpal bones, their proximal and distal articulations, and a highly specialized network of intrinsic and extrinsic ligaments.
The eight carpal bones are anatomically and biomechanically divided into two distinct rows:
* The Proximal Row: Consists of the scaphoid, lunate, triquetrum, and pisiform. The proximal row functions as an intercalated segment, meaning no tendons insert directly onto the scaphoid, lunate, or triquetrum (the pisiform acts primarily as a sesamoid bone within the flexor carpi ulnaris tendon). Their movement is entirely dictated by mechanical forces exerted by the surrounding articulations and ligaments.
* The Distal Row: Consists of the trapezium, trapezoid, capitate, and hamate. This row is tightly bound together by stout interosseous ligaments and functions as a single functional unit that moves synchronously with the metacarpals.
The carpal bones vary significantly in size and articular cartilage coverage. The pisiform and trapezoid are the smallest, while the capitate is the largest, acting as the keystone of the carpal arch. The capitate articulates with seven surrounding bones, whereas the pisiform articulates solely with the triquetrum.
Clinical Pearl: Viegas and colleagues emphasized considerable anatomical variation within the carpus, particularly at the fourth carpometacarpal articulation, the scaphotrapeziotrapezoid (STT) joint, and the capitolunate/hamatolunate articulations. A critical variation is the "Type II Lunate," present in up to 50% of individuals, which features a medial facet that articulates directly with the proximal pole of the hamate. Failure to recognize a Type II lunate can lead to misdiagnosis of hamatolunate arthrosis as generalized midcarpal degenerative joint disease.
THE LIGAMENTOUS ARCHITECTURE OF THE WRIST
The stability of the wrist relies almost entirely on its ligamentous anatomy, which is broadly categorized into extrinsic ligaments (connecting the forearm to the carpus) and intrinsic ligaments (connecting carpal bones to one another).
Volar Extrinsic Ligaments
The volar ligaments are thicker and stronger than their dorsal counterparts, providing the primary restraint against palmar translation of the carpus. They are arranged in a double-V configuration.
* Radioscaphocapitate (RSC) Ligament: Originates from the radial styloid, crosses the waist of the scaphoid, and inserts onto the capitate. It acts as a critical fulcrum around which the scaphoid rotates.
* Long Radiolunate (LRL) Ligament: Originates from the volar margin of the distal radius and inserts onto the radial volar aspect of the lunate. It provides vital stability to the radiolunate articulation.
* Short Radiolunate (SRL) Ligament: Originates from the volar margin of the lunate fossa and inserts onto the proximal volar lunate.
* Radioscapholunate (RSL) Ligament (Ligament of Testut): Historically considered a mechanical ligament, it is now recognized primarily as a neurovascular conduit supplying the scapholunate interosseous ligament. It lacks the collagenous density of true stabilizing ligaments.
* Ulnocarpal Complex: Comprises the ulnolunate and ulnotriquetral ligaments, which arise from the palmar radioulnar ligament of the triangular fibrocartilage complex (TFCC) and insert onto the lunate and triquetrum.
Surgical Warning: The Space of Poirier is a relatively thin, weak area of the volar capsule located between the radioscaphocapitate ligament and the long radiolunate ligament, directly overlying the palmar surface of the lunate/capitolunate joint. In high-energy hyperextension injuries, this capsular defect allows the lunate to dislocate volarly into the carpal tunnel (Mayfield Stage IV perilunate dislocation).
Dorsal Extrinsic Ligaments
The dorsal extrinsic ligaments are thinner but play a crucial role in preventing dorsal carpal subluxation and guiding midcarpal kinematics.
* Dorsal Radiocarpal (DRC) Ligament: A trapezoidal structure originating from the dorsal articular margin of the radius (from Lister's tubercle to the sigmoid notch). It spans the lunotriquetral joint and inserts onto the dorsal tubercle of the triquetrum.
* Dorsal Intercarpal (DIC) Ligament: Originates from the distal dorsal surface of the triquetrum, courses radially across the midcarpal joint, and inserts onto the dorsal ridge of the scaphoid and the trapezium/trapezoid.
Clinical Pearl: The DRC and DIC ligaments form a "lateral V" configuration. The laminated, dynamic structure of the DIC ligament allows it to change shape during wrist movement, providing continuous dorsal stabilization to the scaphoid during wrist flexion.
Intrinsic (Interosseous) Ligaments
- Scapholunate Interosseous Ligament (SLIL): C-shaped ligament divided into dorsal, membranous (proximal), and volar regions. The dorsal band is the thickest and most biomechanically critical for preventing scapholunate dissociation.
- Lunotriquetral Interosseous Ligament (LTIL): Also C-shaped, but conversely, the volar band is the thickest and most critical for stability.
VASCULAR ANATOMY AND CIRCULATION
Understanding the vascular supply to the carpus is paramount, as disruption leads to devastating avascular necrosis (AVN), nonunions, and progressive carpal collapse.
Blood Supply to the Scaphoid
The scaphoid receives its primary blood supply from the radial artery.
* Dorsal Carpal Branch: Supplies 70-80% of the scaphoid, entering through the dorsal ridge and perfusing the proximal pole via retrograde flow.
* Volar Carpal Branch: Supplies the distal 20-30% of the bone, entering at the distal tubercle.
* Pathoclinical Implication: Fractures at the scaphoid waist or proximal pole disrupt the retrograde intraosseous blood supply, placing the proximal pole at an exceptionally high risk for AVN and nonunion.
Blood Supply to the Lunate
The lunate is supplied by a rich extraosseous plexus formed by the dorsal and volar carpal arches.
* In approximately 80% of individuals, the lunate receives blood from both volar and dorsal vessels (Y-shaped or X-shaped intraosseous anastomoses).
* In 20% of individuals, the lunate relies on a single volar or dorsal vessel. This anatomical variant significantly increases the susceptibility to Kienböck's Disease (avascular necrosis of the lunate) following repetitive microtrauma or altered biomechanical loading (e.g., ulnar minus variance).
BIOMECHANICS AND KINEMATICS
The wrist is not a simple hinge joint; it operates through complex, multi-planar kinematics.
The Intercalated Segment Principle
Because no tendons insert on the proximal row, its motion is entirely dependent on the mechanical forces of the distal row and the forearm.
* The scaphoid has a natural tendency to flex due to its oblique orientation and the compressive forces of the trapezium and trapezoid.
* The triquetrum has a natural tendency to extend due to its articulation with the hamate.
* The lunate acts as the central balancing link. When the SLIL is intact, the scaphoid pulls the lunate into flexion. When the LTIL is intact, the triquetrum pulls the lunate into extension.
Carpal Instability Patterns
- Dorsal Intercalated Segment Instability (DISI): Occurs when the SLIL is ruptured. The scaphoid flexes independently, and the lunate, now tethered only to the triquetrum, extends.
- Volar Intercalated Segment Instability (VISI): Occurs when the LTIL is ruptured. The triquetrum extends independently, and the lunate, tethered to the scaphoid, flexes.
Dart Thrower's Motion (DTM)
Most functional activities of daily living do not occur in pure flexion/extension or radial/ulnar deviation. They occur in an oblique plane known as the Dart Thrower's Motion—moving from radial extension to ulnar flexion.
* During DTM, there is minimal movement at the radiocarpal joint (specifically the scaphoid and lunate remain relatively stationary).
* The majority of motion occurs at the midcarpal joint.
* Surgical Implication: Rehabilitation protocols following scapholunate ligament repair often utilize DTM early in the recovery phase, as it minimizes stress on the healing SLIL while allowing functional midcarpal movement.
SURGICAL APPROACHES TO THE WRIST
Mastery of surgical approaches is critical for the management of fractures, nonunions, and ligamentous reconstructions.
The Dorsal Approach to the Wrist
Indications: Scaphoid nonunion (proximal pole), perilunate dislocations, proximal row carpectomy, partial or total wrist arthrodesis, and dorsal ganglion excision.
Step-by-Step Technique:
1. Positioning: Supine, arm on a hand table, pronated. Tourniquet applied.
2. Incision: A longitudinal incision centered over Lister's tubercle.
3. Superficial Dissection: Identify and protect the dorsal sensory branches of the radial and ulnar nerves.
4. Extensor Retinaculum: Open the third extensor compartment. Transpose the Extensor Pollicis Longus (EPL) tendon radially.
5. Subperiosteal Elevation: Elevate the second compartment (ECRL, ECRB) radially and the fourth compartment (EDC, EIP) ulnarly.
6. Capsulotomy:
* Berger's Ligament-Sparing Capsulotomy: Create a radially based flap by incising the capsule in line with the fibers of the Dorsal Radiocarpal (DRC) and Dorsal Intercarpal (DIC) ligaments. This preserves the proprioceptive innervation and vascularity of the dorsal capsule, preventing postoperative stiffness.
Pitfall: Avoid a simple vertical midline capsulotomy. Transecting the DRC and DIC ligaments perpendicularly destroys the dorsal stabilizing sling of the carpus and significantly increases the risk of postoperative iatrogenic carpal instability.
The Volar Approach (Extended FCR Approach)
Indications: Distal radius fractures, scaphoid waist fractures, volar perilunate dislocations, and excision of volar carpal tumors.
Step-by-Step Technique:
1. Positioning: Supine, arm on a hand table, supinated.
2. Incision: Longitudinal incision over the Flexor Carpi Radialis (FCR) tendon, zig-zagging across the wrist crease if extending into the palm.
3. Superficial Dissection: Incise the FCR sheath. Retract the FCR tendon ulnarly to protect the median nerve.
4. Deep Dissection: Incise the floor of the FCR sheath. This exposes the Parona's space.
5. Pronator Quadratus: Identify the pronator quadratus. Release it from its radial border (L-shaped incision) and reflect it ulnarly to expose the distal radius and volar radiocarpal capsule.
6. Capsulotomy: If accessing the carpus, perform a volar radiocarpal capsulotomy, being meticulously careful to repair the stout volar extrinsic ligaments (RSC, LRL) during closure to prevent volar subluxation of the carpus.
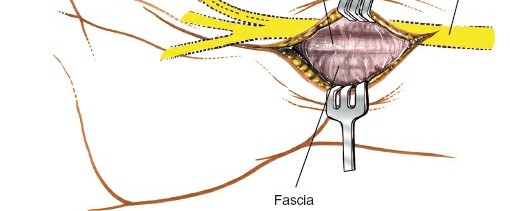
Surgical Warning: The Palmar Cutaneous Branch of the Median Nerve (PCBMN) arises approximately 5 cm proximal to the wrist crease and travels in the fascia between the FCR and the Palmaris Longus. Always retract the FCR ulnarly and avoid aggressive radial dissection in the subcutaneous tissues to prevent painful neuromas.
DISTAL RADIOULNAR JOINT (DRUJ) AND TFCC ANATOMY
The DRUJ and the Triangular Fibrocartilage Complex (TFCC) are the primary stabilizers of the ulnar aspect of the wrist.
Components of the TFCC
The TFCC is a complex, multi-component structure that absorbs 20% of the axial load transmitted across the wrist and stabilizes the DRUJ during forearm rotation.
* Articular Disc (Triangular Fibrocartilage): The central portion, which is avascular and prone to degenerative tearing.
* Volar and Dorsal Radioulnar Ligaments: The primary stabilizers of the DRUJ. The dorsal ligament is tight in pronation; the volar ligament is tight in supination.
* Meniscus Homologue: Connects the articular disc to the triquetrum.
* Ulnocarpal Ligaments: Ulnolunate and ulnotriquetral ligaments.
* Extensor Carpi Ulnaris (ECU) Subsheath: Intimately blended with the dorsal aspect of the TFCC.
Surgical Implications for DRUJ Instability
- Ulnar Impaction Syndrome: Positive ulnar variance leads to excessive load-bearing across the ulnar carpus, resulting in central TFCC tears, lunate/triquetral chondromalacia, and LTIL tears. Treatment often requires Ulnar Shortening Osteotomy to decompress the ulnocarpal joint and tighten the ulnocarpal ligaments.
- TFCC Repairs: Peripheral tears (vascular zone) are amenable to arthroscopic or open repair. Central tears (avascular zone) require arthroscopic debridement.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Successful outcomes in wrist surgery depend as much on meticulous postoperative rehabilitation as on surgical execution.
- Immobilization: Following ligamentous repair (e.g., SLIL reconstruction) or complex carpal fracture fixation, the wrist is typically immobilized in a short-arm cast or rigid orthosis for 4 to 8 weeks, depending on the rigidity of the fixation.
- Early Motion: For stable internal fixation (e.g., headless compression screw for scaphoid fractures), early active range of motion (AROM) can be initiated at 2 weeks to prevent capsular contracture.
- Proprioceptive Rehabilitation: The wrist ligaments are rich in mechanoreceptors. Postoperative therapy must include proprioceptive neuromuscular facilitation (PNF) and dart thrower's motion exercises to retrain the dynamic muscular stabilizers (FCR, FCU, ECU, ECRL/B) to protect the static ligamentous repairs.
- Load Bearing: Heavy lifting and axial loading are strictly prohibited until radiographic evidence of bony union or complete ligamentous healing is confirmed, typically at 10 to 12 weeks postoperatively.
You Might Also Like