Hemi-Hamate Autograft for Proximal Interphalangeal Joint Reconstruction
Key Takeaway
The hemi-hamate autograft is a highly effective surgical technique for reconstructing unstable dorsal fracture-dislocations of the proximal interphalangeal (PIP) joint. By harvesting the distal articular ridge of the hamate, surgeons can anatomically restore the volar articular concavity and volar lip of the middle phalanx. This procedure provides superior osseous stability compared to soft tissue arthroplasty, allowing for early postoperative mobilization and optimizing functional outcomes in complex intra-articular hand injuries.
Introduction and Biomechanical Rationale
Fracture-dislocations of the proximal interphalangeal (PIP) joint present a formidable challenge to the orthopedic hand surgeon. When the volar lip of the middle phalanx is fractured, the critical restraint to dorsal subluxation is lost. While fractures involving less than 30% to 40% of the articular surface can often be managed with extension block splinting or volar plate arthroplasty, injuries involving greater than 50% of the articular surface typically result in chronic dorsal instability and require structural osseous reconstruction.
The hemi-hamate autograft, popularized by Williams et al., has emerged as the gold standard for reconstructing these massive volar articular defects. The biomechanical genius of this procedure lies in the unique morphological match between the distal articular surface of the hamate and the base of the middle phalanx. The hamate articulates distally with the fourth and fifth metacarpals, separated by a distinct central longitudinal ridge. This ridge perfectly mimics the median ridge of the middle phalangeal base, allowing for an anatomic restoration of the PIP joint's biconcave articular geometry. By restoring the volar buttress, the surgeon re-establishes the intrinsic stability of the joint, permitting the early active range of motion (ROM) necessary to prevent debilitating stiffness.
Indications and Preoperative Planning
Surgical Indications
- Unstable Dorsal PIP Fracture-Dislocations: Specifically, those involving >40% to 50% of the volar articular surface of the middle phalanx.
- Chronic PIP Joint Instability: Cases presenting weeks to months post-injury where primary repair or closed reduction is no longer feasible.
- Failed Conservative Management: Inability to maintain concentric reduction using extension block splinting.
- Pilon-type Fractures: Where the volar articular fragments are too comminuted for primary open reduction and internal fixation (ORIF), but the dorsal cortex remains intact.
Contraindications
- Inadequate Dorsal Bone Stock: The middle phalanx must have a sufficient dorsal cortical bridge to support the graft and accept screw fixation. If the dorsal cortex is highly comminuted, an alternative salvage procedure (e.g., joint arthrodesis or silicone arthroplasty) must be considered.
- Active Infection: Absolute contraindication for any autograft procedure.
- Severe Pre-existing Osteoarthritis: Degenerative changes in the proximal phalangeal head will compromise the outcome of the hemi-hamate arthroplasty.
💡 Clinical Pearl: Preoperative Imaging
Standard posteroanterior (PA), true lateral, and oblique radiographs of the affected digit are mandatory. A true lateral view is critical to assess the percentage of articular surface involvement and the degree of dorsal subluxation. In complex or chronic cases, a computed tomography (CT) scan with 3D reconstructions is highly recommended to precisely quantify the defect size and evaluate the integrity of the dorsal middle phalangeal cortex.
Surgical Technique: Step-by-Step Masterclass
Patient Positioning and Anesthesia
The procedure is performed with the patient in the supine position with the operative arm extended on a radiolucent hand table. Regional anesthesia (axillary or supraclavicular brachial plexus block) is preferred to provide excellent intraoperative analgesia and postoperative pain control. A well-padded upper arm tourniquet is applied and inflated to 250 mm Hg after exsanguination of the limb. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
1. Approach and Exposure of the PIP Joint
The goal of the approach is to achieve circumferential visualization of the middle phalangeal base without compromising the delicate vascular supply to the remaining bone.
- Incision: Expose the PIP joint through a volar V-shaped incision (Bruner-type). The apex of the V can be directed either radially or ulnarly, extending from the palmar digital crease proximally to the distal interphalangeal (DIP) joint flexion crease distally.
- Neurovascular Protection: Carefully elevate the skin flaps. Identify and meticulously protect the radial and ulnar neurovascular bundles throughout the procedure.
- Flexor Sheath Management: Open the flexor tendon sheath precisely between the A2 and A4 pulleys. The A2 and A4 pulleys must be preserved to prevent postoperative flexor tendon bowstringing.
- Tendon Retraction: Retract the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons to the side. This is facilitated by releasing them from the accessory collateral ligaments.
2. Joint Preparation and the "Shotgun" Maneuver
Unparalleled exposure of the articular surface is required to prepare the defect and inset the graft accurately.
- Volar Plate Excision: Excise any comminuted, non-viable bone fragments attached to the volar plate. Retract the volar plate proximally to expose the middle phalangeal fracture site and the head of the proximal phalanx.
- Collateral Ligament Release: Release the proper collateral ligaments from their insertions on the middle phalanx.
> 🚨 Surgical Warning: You must leave a small, robust portion of the collateral ligament attached to the base of the middle phalanx. This remnant is critical to facilitate the reattachment of the volar plate during closure. - The "Shotgun" Exposure: Hyperextend the PIP joint to "shotgun" the articular surfaces. This maneuver hinges the joint open dorsally, providing a direct, en face view of the proximal phalangeal head and the fractured base of the middle phalanx.
- Defect Preparation: Remove all remaining loose bone fragments from the defect. Prepare the base of the middle phalanx using a fine rongeur and a micro-oscillating saw. Create a flat, bleeding cancellous bed to accept the graft.
> 🚨 Pitfall: Take special care not to remove excessive dorsal bone. Over-resection will compromise the dorsal cortical bridge, leading to an iatrogenic fracture of the middle phalanx during screw insertion. - Measurement: Use sterile calipers to measure the exact dimensions (width, depth, and height) of the prepared defect.
3. Harvesting the Hemi-Hamate Autograft
The graft is harvested from the ipsilateral wrist, minimizing the surgical footprint while providing an ideal osteochondral match.
- Incision: Under fluoroscopic guidance, make a 3-cm transverse incision over the dorsal aspect of the carpometacarpal (CMC) joints, centered at the bases of the ring and small fingers.
- Exposure: Dissect through the subcutaneous tissue, protecting the dorsal sensory branches of the ulnar nerve. Perform a longitudinal capsulotomy over the 4th and 5th CMC joints to locate the distal articular surface of the hamate.
- Marking the Graft: Identify the central articular ridge of the distal hamate. Mark the desired graft dimensions centered exactly on this ridge. The harvested graft should be slightly larger than the measured phalangeal defect to allow for precise final contouring.
- Osteotomies:
- Make the axial hamate cut and the sagittal hamate cuts using a fine osteotome or a micro-sagittal saw.
- The coronal cut is best made with a curved osteotome. This cut is significantly facilitated by first removing a small notch of bone proximal to the axial cut.
🚨 Surgical Warning: Ensure the coronal cut is not made too obliquely. The deep surface of the graft must be contoured to cup the head of the proximal phalanx accurately.
4. Graft Contouring and Fixation
Precise inset and rigid fixation are the cornerstones of a successful hemi-hamate arthroplasty.
- Contouring: Bring the graft to the recipient site. Use a high-speed burr or fine rongeur to contour the deep and peripheral surfaces of the graft until it fits perfectly into the defect. If the defect is excessively deep, cancellous bone graft (harvested from the hamate site) can be placed under the distal end of the graft to ensure it maintains a cupped shape.
- Provisional Fixation: Reduce the graft into the defect and provisionally secure it with a single 0.9-mm (0.035-inch) Kirschner wire placed through the center of the graft into the dorsal cortex of the middle phalanx.
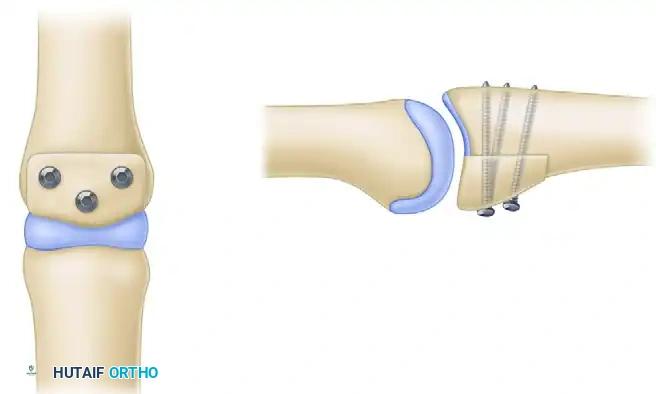
- Definitive Fixation: Fix the graft rigidly in place using two or three 1.0-mm to 1.5-mm screws directed from volar to dorsal. The screws should be placed in lag fashion to compress the graft into the host bone bed. A third screw can be placed in the hole left by the provisional K-wire if the graft size permits.
Volar view of the PIP joint demonstrating the hemi-hamate graft secured with three interfragmentary screws.

Lateral view of the PIP joint showing the inset graft reconstituting the articular concavity and the volar lip.
Detail of the 1.0 mm or 1.3 mm screws placed through the hamate graft.
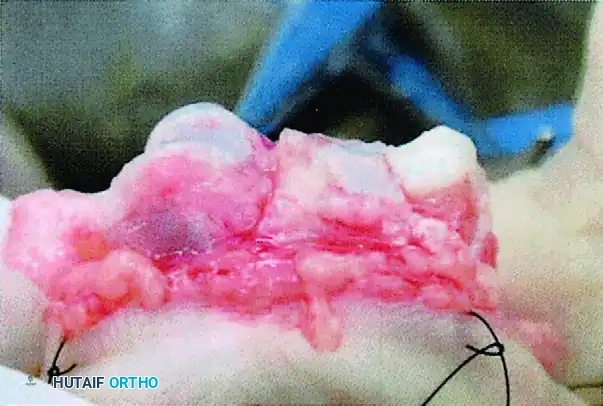
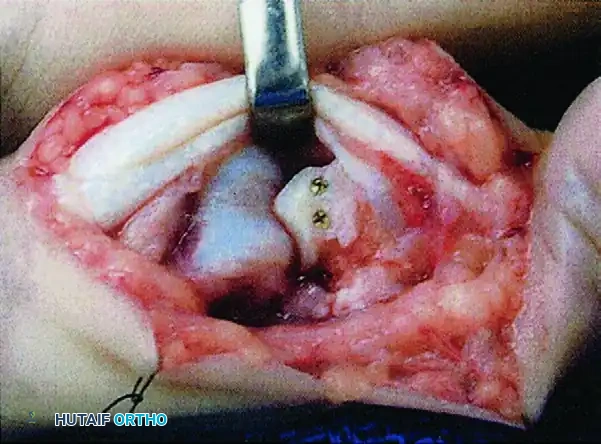
Clinical intraoperative photograph showing the hemi-hamate graft held securely in place with interfragmentary screws.
5. Radiographic Assessment and The "False Step-Off" Phenomenon
Once the graft is secured, reduce the PIP joint and assess the reduction and hardware placement using intraoperative fluoroscopy.
💡 Clinical Pearl: The Radiographic Illusion
It is critical to understand that the articular cartilage of the hamate is significantly thicker than the native cartilage of the proximal phalangeal base. Consequently, when the cartilaginous surfaces are perfectly flush and anatomically reduced visually, the subchondral bone lines on the radiograph will not align. This creates an apparent radiographic "step-off." This false step-off should not be worrisome as long as the visual reduction of the articular cartilage was confirmed to be satisfactory prior to joint closure.
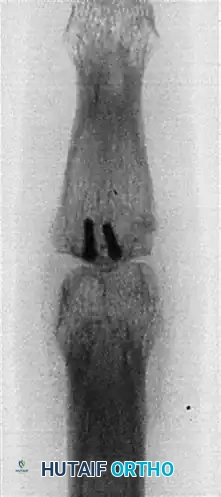
Postoperative AP radiograph demonstrating graft incorporation and screw trajectory.
Postoperative lateral radiograph. Note the false articular step-off created by the thicker articular cartilage at the distal hamate compared with the base of the middle phalanx.
6. Closure and Soft Tissue Reconstruction
- Distal Contouring: Contour the distal edge of the graft so that it transitions smoothly with the volar cortex of the middle phalanx, preventing any sharp edges that could abrade the flexor tendons.
- Volar Plate Reattachment: Reattach the volar plate to the collateral ligament stumps that were preserved earlier.
- Tendon Gliding: To prevent postoperative adhesions, the reflected flexor sheath may be interposed between the flexor tendons and the repaired volar plate.
- Hemostasis: Deflate the tourniquet, obtain meticulous hemostasis using bipolar electrocautery, and close the skin with non-absorbable sutures.
- Splinting: Apply a bulky soft dressing and a dorsal plaster splint, blocking the PIP joint in 20 degrees of flexion to prevent immediate stress on the volar reconstruction.
Postoperative Care and Rehabilitation Protocol
The success of a hemi-hamate autograft relies heavily on a strict, supervised hand therapy protocol. Early motion is essential to prevent stiffness, but it must be protected to avoid graft displacement.
- Days 1-7: The patient remains in the initial dorsal blocking splint (PIP joint at 20 degrees of flexion). Elevation and strict edema control measures are instituted immediately.
- Week 1: The bulky dressing is removed. A custom thermoplastic figure-of-eight splint is fabricated with a 15-degree extension block. This splint provides lateral stability while preventing terminal extension, which is the position of maximum instability. Active and active-assisted range-of-motion (ROM) exercises for PIP and DIP flexion are initiated under the guidance of a certified hand therapist.
- Weeks 2-6: The extension block is gradually reduced by 10 degrees each week, provided concentric reduction is maintained on weekly lateral radiographs.
- Weeks 6-8: The splint is discontinued for daily activities. Gentle passive stretching and strengthening exercises are introduced.
- Months 3-6: Unrestricted activity is gradually permitted. Maximum medical improvement regarding ROM and swelling may take up to 12 months.
Complications and Alternative Treatments
Potential Complications
Despite achieving a concentric reduction and rigid fixation, some fractures around the PIP joint result in poor outcomes.
* Persistent Swelling and Stiffness: Limited motion and intrinsic imbalance commonly accompany comminuted fractures of the middle phalangeal base, regardless of the method of open reduction. The PIP joint is notoriously unforgiving regarding capsular scarring.
* Graft Failure/Resorption: Rare, but can occur if the vascular bed is inadequate or if fixation fails.
* Hardware Prominence: Screws may require removal if they irritate the flexor tendons or dorsal skin.
* Donor Site Morbidity: Pain or subluxation at the 4th/5th CMC joints is uncommon but possible.
Alternative: Closed Reduction and Extension Block Splinting
Marked comminution of the middle phalangeal shaft or base that extends beyond the volar lip may be treated better by traction or splinting than by internal devices. These highly complex, "pilon-type" injuries are often not suited to open reduction techniques, as stripping the undisturbed soft tissues around the fracture fragments can devascularize the bone and delay healing.
Extension Block Splinting Technique:
1. After closed reduction under local anesthesia, a malleable metal dorsal splint is incorporated into a forearm gauntlet plaster cast.
2. The involved finger is maintained in flexion at both the PIP and metacarpophalangeal (MCP) joints.
3. Because dorsal instability occurs when the PIP joint is extended, the exact angle of subluxation is determined fluoroscopically before applying the plaster.
4. The PIP joint is blocked in flexion 15 degrees short of this demonstrated position of instability.
5. The proximal phalanx must be held securely against the dorsal splint to avoid compensatory extension at the PIP joint caused by further flexion of the MCP joint.
6. Immediate active flexion of the PIP joint is permitted and encouraged.
7. Full extension is strictly prohibited for 6 to 12 weeks. However, the extension block is decreased incrementally each week to allow progressive extension as the fracture consolidates.
Conclusion
The hemi-hamate autograft is a sophisticated, highly effective technique for the salvage of unstable dorsal PIP fracture-dislocations. By utilizing an osteochondral graft that perfectly matches the native anatomy of the middle phalanx, surgeons can restore joint congruity, re-establish the volar buttress, and permit the early mobilization necessary for optimal functional recovery. Mastery of the precise osteotomies, rigid lag screw fixation, and understanding of the radiographic "false step-off" are essential for any hand surgeon undertaking this complex reconstruction.
📚 Medical References
- hemi-hamate autograft, J Hand Surg 28A:856, 2003.
- Wolfe SW, Katz LD: Intraarticular impaction fractures of the phalanges, J Hand Surg 20A:327, 1995.
- Wood MB, Dobyns JH: Chronic, complex volar dislocations of the metacarpophalangeal joint, J Hand Surg 6A:73, 1981.
- Zielinski CJ: Irreducible fracture-dislocation of the distal interphalangeal joint, J Bone Joint Surg 65A:109, 1983.
- Zimmerman NB, Weiland AJ: Ninety-ninety intraosseous wiring for internal fi xation of the digital skeleton, Orthopedics 12:99, 1989.
- Mallet Finger Crawford GP: The molded polythene splint for mallet fi nger deformities, J Hand Surg 9A:231, 1984.
- Doyle JR: Extensor tendon injuries. In Green DP, ed:
You Might Also Like

