Forearm Malunions and Radioulnar Synostosis: Surgical Management
Key Takeaway
Forearm malunions significantly compromise upper extremity kinematics, often leading to restricted pronosupination, distal radioulnar joint instability, and chronic pain. Management requires a meticulous understanding of forearm biomechanics, particularly the restoration of the radial bow and radiocapitellar congruity. Surgical interventions range from corrective osteotomies and radial head arthroplasty to the complex resection of radioulnar synostosis. This guide details the indications, operative techniques, and rehabilitation protocols for proximal and diaphyseal forearm malunions.
FOREARM MALUNIONS: BIOMECHANICS AND CLASSIFICATION
The forearm functions as a highly complex, articulated ring, analogous to the pelvic ring but with the added requirement of dynamic rotation. The radius and ulna articulate at the proximal radioulnar joint (PRUJ) and the distal radioulnar joint (DRUJ), tethered centrally by the interosseous membrane (IOM). Any alteration in the length, alignment, or rotational axis of either bone can profoundly disrupt the kinematics of pronation and supination.
Malunions of the proximal third of the radius and ulna present unique reconstructive challenges and can be systematically classified into five distinct categories:
1. Malunions of the radial head.
2. Malunions of the radial neck.
3. Malunions of the olecranon.
4. Malunions of the proximal third of the ulna with anterior dislocation of the proximal radius (Monteggia fracture-dislocation).
5. Malunions complicated by radioulnar synostosis.
RADIAL HEAD MALUNIONS
Malunion of the radial head with only mild deformity may remain asymptomatic and not inherently disabling. If symptoms are strictly localized and caused by a small, abnormal prominence of bone impinging on the radial notch of the ulna, isolated resection of the prominence may relieve mechanical blocks.
However, severe deformity invariably causes pain, limits pronation and supination, and can restrict terminal flexion or extension of the elbow.
Surgical Management: Excision vs. Arthroplasty
Historically, severe symptomatic malunions were treated by excising the radial head. During excision, all loose fragments of bone, excess heterotopic ossification, scar tissue, periosteum, and remnants of the annular ligament must be excised meticulously to prevent the formation of new bone in the region.
🚨 CRITICAL WARNING: While excising the radial head can restore function in isolated injuries, it frequently yields disappointing long-term results. Reported complications of isolated radial head excision include loss of grip strength, chronic wrist pain, proximal migration of the radius, DRUJ instability (Essex-Lopresti phenomenon), and valgus instability of the elbow.
Indications for Prosthetic Replacement:
Prosthetic radial head replacement (metallic, modular arthroplasty) is strictly indicated for patients with radial head malunions associated with:
* Distal radioulnar joint (DRUJ) pain or instability.
* Longitudinal radioulnar dissociation (interosseous membrane compromise).
* Laxity or insufficiency of the medial ulnar collateral ligament (MUCL) complex of the elbow.
RADIAL NECK MALUNIONS
While most radial neck fractures are managed successfully with nonoperative protocols, symptomatic malunions occasionally occur, presenting with pain, crepitance, elbow laxity, and severe limitation of forearm rotation.
Because of the potential adverse sequelae associated with radial head excision, the modern orthopedic consensus strongly favors maintaining radial length and restoring the congruity of the radiocapitellar articulation, provided the articular cartilage remains viable. Corrective osteotomy of the radial neck is the procedure of choice for symptomatic malunions. Clinical evidence demonstrates that correcting angular deformities (e.g., 30 degrees of ulnar angulation) via osteotomy can restore a pain-free, stable elbow with near-normal flexion, extension, and pronosupination.
🔪 Surgical Technique: Corrective Osteotomy of the Radial Neck
Preoperative Preparation and Positioning:
* The patient is positioned supine with the arm draped free on a hand table.
* A non-sterile tourniquet is applied high on the brachium.
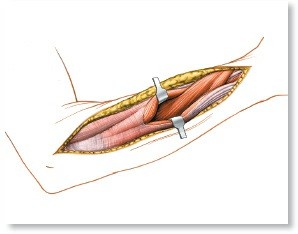
Surgical Approach:
* Expose the proximal radius and radiocapitellar joint through a standard posterolateral (Kocher) approach, utilizing the internervous plane between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).
* Débride the joint of inflamed synovium and meticulously inspect the articular cartilage of the capitellum and proximal radius.
Surgical Pearl: If the extent of arthritic change is severe (Outerbridge Grade IV), an osteotomy will likely fail, and radial head arthroplasty should be performed instead.
Osteotomy and Fixation:
* If the cartilage is preserved, perform an osteotomy in the proximal radius approximately 1.5 cm from the articular surface. Use a small motorized oscillating saw under continuous saline irrigation to prevent thermal necrosis. Protect the surrounding soft tissues, particularly the posterior interosseous nerve (PIN), with Hohmann retractors.
* Alternatively, a sharp, thin osteotome can be used to divide the bone to minimize bone loss from the saw kerf.
* Realign the proximal radius to restore the anatomical congruity of the radiocapitellar joint.
* Fix the osteotomy with two Herbert screws directed from proximal to distal.
* Alternative Fixation: Kirschner wires or minifragment lag screws (2.0 mm or 2.7 mm). If hardware is placed through the articular surface of the proximal radius, it is imperative to recess the screw head below the surface of the cartilage to prevent capitellar abrasion.
* Pack autogenous cancellous bone graft (harvested from the lateral epicondyle of the humerus or olecranon) at the osteotomy site to promote union.
* Repair the annular ligament and lateral ulnar collateral ligament (LUCL) meticulously during closure to prevent posterolateral rotatory instability (PLRI).
Postoperative Protocol:
The elbow is immobilized in a posterior splint in mid-flexion (90 degrees) and mid-supination for 2 weeks. Following this, a removable functional orthosis is applied, and progressive active range-of-motion (ROM) exercises are initiated. External support is discontinued once radiographic healing of the osteotomy is secure (typically 6 to 8 weeks).
OLECRANON MALUNIONS
In the setting of an olecranon malunion, attempting an osteotomy and realignment of the fragments is generally contraindicated. Such operations almost always increase disability due to the difficulty of restoring perfect articular congruity in a chronically deformed greater sigmoid notch, leading to profound stiffness.
Instead, elbow function can be significantly improved by excising the deformed, malunited portion of the bone and advancing the triceps.
The "0.3 cm Rule" for Olecranon Excision
Extensive biomechanical studies have shown that a large portion of the olecranon can be excised without causing elbow instability, provided the critical stabilizing portion of the coronoid and the base of the olecranon remain intact.
Determining the Resection Level:
1. Obtain a true lateral radiograph of the elbow flexed to 90 degrees.
2. Draw a line through the center of the longitudinal axis of the humerus, extending across the joint.
3. Crucial Landmark: At least 0.3 cm of the olecranon must project posterior to this line. This minimal osseous block is required to prevent anterior subluxation of the proximal ulna relative to the distal humerus.
4. The malunited bone proximal to this mark can be safely excised.
5. The triceps tendon must be reattached accurately and firmly to the proximal ulna using heavy non-absorbable sutures passed through transosseous drill holes or utilizing modern suture anchors.
MONTEGGIA FRACTURE MALUNIONS (PROXIMAL ULNA WITH RADIAL HEAD DISLOCATION)
A Monteggia fracture that unites in a malaligned position creates a profoundly disabling deformity. The shortened, angulated ulna forces the radial head to remain dislocated, leading to severe pain, restricted rotation, and progressive radiocapitellar arthrosis. Reconstruction is technically demanding but essential to salvage upper extremity function.
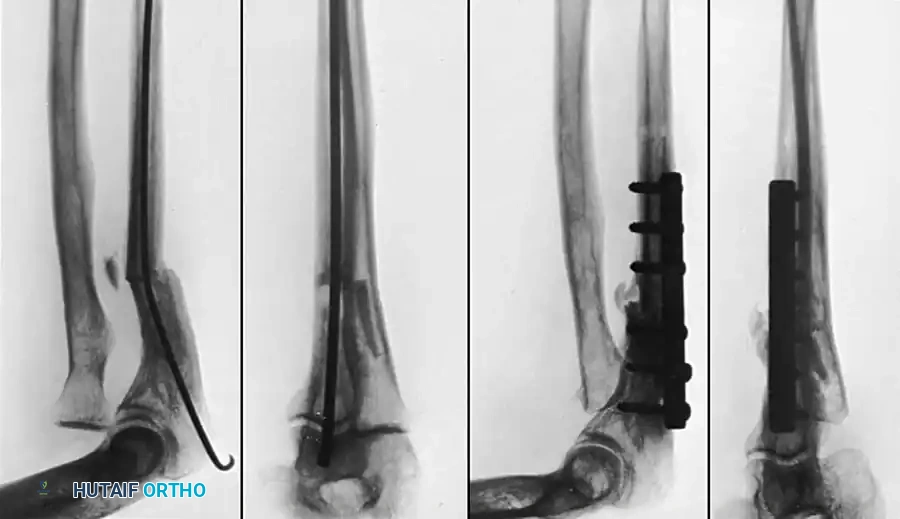
Fig. 55-29: (A) Malunited fracture of the shaft of the ulna with chronic dislocation of the proximal radius (Monteggia fracture). (B) Four months post-reconstruction involving ulnar osteotomy, application of a compression plate, and radial head excision with the fragmented bone used as autograft for the ulna. Excellent motion was restored.
🔪 Surgical Technique: Monteggia Malunion Reconstruction
Approach and Radial Head Management:
* Expose the radial head and the ulnar malunion through a single extensile posterior incision (Boyd approach), or utilize two separate incisions to minimize soft-tissue stripping.
* If using two incisions, make a 5 cm posterolateral (Kocher) incision. Free the chronically dislocated radial head from all fibrotic attachments and capsular adhesions.
* Divide the neck of the radius just proximal to the bicipital tuberosity.
* Technique Tip: Drill several holes transversely through the bone at the level of the anticipated osteotomy to prevent splintering. Complete the division with double-action bone-cutting forceps while rotating the radial shaft, and smooth the end of the bone with a small rongeur.
Ulnar Osteotomy and Fixation:
* Make a second incision 7.5 cm long over the subcutaneous border of the posterior ulna.
* Perform an osteotomy of the ulna as near to the apex of the old fracture deformity as possible.
* Biomechanical Imperative: The ulna must be distracted and realigned to restore its anatomical length. Failure to restore ulnar length will result in recurrent subluxation of the radius.
* Fix the realigned ulna with a robust dynamic compression plate (DCP) or locking compression plate (LCP).
* Pack autogenous cancellous bone graft (often utilizing the excised radial head, fragmented into cancellous chips) around the ulnar osteotomy site to ensure rapid consolidation.
Postoperative Protocol:
Apply a long arm cast with the elbow at 90 degrees of flexion and the forearm in neutral rotation. The cast is maintained until osseous union is solid, usually at about 12 weeks, after which intensive active exercises are begun.
Pediatric Consideration: In children with malunited Monteggia fractures, radial head excision is strictly contraindicated. Treatment consists of an opening wedge osteotomy of the ulna, open reduction of the radial head, and temporary transarticular radiocapitellar Kirschner wire fixation to maintain reduction until the interosseous membrane and annular ligament heal.
RADIOULNAR SYNOSTOSIS
Synostosis (cross-union) between the radius and the ulna is a devastating complication that abolishes forearm pronation and supination. It typically develops at the proximal radioulnar joint following severely comminuted fractures, high-energy trauma, or traumatic brain injuries.
Classification (Jupiter and Ring)
Jupiter and Ring classified proximal radioulnar synostosis into three distinct anatomical types:
* Type A: Synostosis located at or distal to the bicipital tuberosity.
* Type B: Synostosis involving the radial head and the proximal radioulnar joint.
* Type C: Synostosis contiguous with heterotopic bone extending across the elbow joint to the distal aspect of the humerus.
Timing of Surgical Intervention
Historically, surgical dogma dictated delaying operative resection for 6 to 12 months to allow the heterotopic bone to "mature," theoretically reducing the risk of recurrence. However, modern evidence challenges this. Jupiter and Ring, along with other contemporary authors, advocate for early resection. Early intervention limits the degree of secondary soft-tissue contracture, prevents capsular fibrosis, and significantly reduces the overall period of severe patient disability.
Surgical Options: Resection vs. Pseudarthrosis Creation
The most direct treatment is the complete en bloc resection of the synostosis mass. Various interpositional materials (free fat grafts, vascularized anconeus muscle pedicle grafts) have been used to prevent recurrence, though their absolute necessity remains debated if the resection is thorough and early motion is achieved.
When a proximal radioulnar synostosis is too extensive for safe resection, involves the articular surface, or is associated with severe anatomical deformity, creation of a pseudarthrosis (Kamineni technique) is a highly reliable salvage procedure.
🔪 Surgical Technique: Creation of Radial Pseudarthrosis (Kamineni Technique)
This technique restores forearm rotation by creating a controlled non-union distal to the fused proximal radioulnar joint.
- With the patient supine under general anesthesia, apply and inflate a sterile tourniquet.
- Bring the affected arm across the patient’s chest, stabilized by an assistant.
- Utilize a Kocher approach to the proximal radius.
- Enter the interval between the anconeus and the extensor carpi ulnaris. Direct the deep dissection toward the ulnar shaft and the synostosis mass. Follow the synostosis to its distal margin by carefully elevating the supinator muscle off the radius.
- The Resection: Using a power oscillating saw, resect a precise 1-cm cylindrical section of the radial diaphysis. This can be done either proximal or distal to the bicipital tuberosity, dictated by the distal extent of the synostosis.
- Crucial Step: Apply bone wax generously to the exposed medullary canals and cortical ends of the resected radius. This is the single most important technical factor to prevent re-ankylosis and ensure a permanent pseudarthrosis.
- Examine the range of motion of the forearm intraoperatively. Gently manipulate the forearm to break any residual soft-tissue adhesions.
Postoperative Rehabilitation:
Continuous passive motion (CPM) therapy is utilized for the first 48 hours. Following this, a rigorous static pronation-supination splinting program is initiated. A two-component splint is used: an arm-to-forearm component and an inner gauntlet shell. A Velcro strap dynamically rotates the forearm to maximal attainable pronation and supination.
* Weeks 1-3: Full supination at night; active/passive motion for 1 hour in the morning; full pronation until noon; 1 hour free at lunch; full supination until dinner; 1 hour free at dinner; full pronation in the evening.
* After 3 weeks: Splint-free periods are progressively increased based on clinical progress.
SHAFTS OF THE RADIUS AND ULNA IN ADULTS
Malunion of diaphyseal both-bone forearm fractures frequently causes functional deficits severe enough to warrant complex surgical correction. The forearm relies on a delicate spatial relationship between the radius and ulna; malrotation, angular deformity encroaching on the interosseous space, and loss of the anatomical radial bow all compromise functional outcomes.
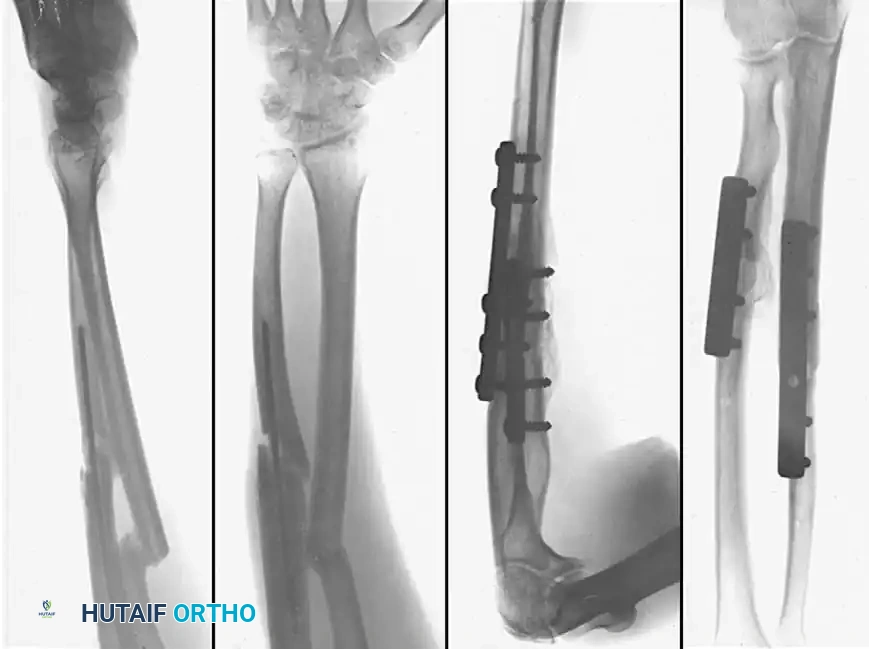
Diaphyseal malunion of the radius and ulna treated with corrective osteotomies and rigid internal fixation using dynamic compression plates.
Biomechanics of Diaphyseal Deformity
The degree of deformity that mandates surgical intervention is based on biomechanical thresholds:
* Matthews et al. demonstrated in cadaveric models that a 10-degree angular deformity causes an insignificant reduction in forearm rotation. However, a 20-degree angulation causes a profound, clinically unacceptable loss of pronation and supination.
* Tarr et al. confirmed that angular or rotational deformities of 10 degrees or less result in minimal limitation, but 15 degrees of total deformity reduces forearm motion by more than 27% (except in distal-third fractures, which are more forgiving).
* Schemitsch and Richards highlighted the critical importance of the radial bow. The maximum radial bow normally measures approximately 15 mm and is located at roughly 60% of the radial length from the bicipital tuberosity. Failure to restore the proper magnitude and location of the radial bow directly correlates with permanently reduced forearm rotation and diminished grip strength.
Indications for Surgical Correction
The decision to operate on a diaphyseal forearm malunion should be individualized, based on the patient's functional limitations and physical demands rather than radiographic appearance alone.
Primary indications include:
1. Clinically significant loss of pronosupination affecting activities of daily living.
2. Distal radioulnar joint (DRUJ) instability or impingement secondary to shortening.
3. Unacceptable cosmetic deformity (rarely the sole indication).
Clinical Pitfall: Restoring proper skeletal alignment via osteotomy may not fully reverse functional deficits if there is severe, concurrent soft-tissue contracture of the interosseous membrane or prolonged joint immobilization. Patients must be counseled preoperatively regarding the limitations of osseous correction in the presence of chronic soft-tissue fibrosis.
Surgical Principles for Diaphyseal Correction:
* Preoperative Templating: Contralateral normal forearm radiographs are essential to template the exact location and magnitude of the normal radial bow.
* Approach: The radius is typically approached via a volar (Henry) approach to allow for optimal plate placement on the flat tension surface, while the ulna is approached directly over its subcutaneous border.
* Fixation: Following corrective osteotomy (often requiring a structural tricortical iliac crest bone graft to restore length and correct angular deformity), rigid fixation with 3.5 mm limited contact dynamic compression plates (LC-DCP) or locking compression plates (LCP) is mandatory. At least six cortices of fixation (three screws) are required proximal and distal to the osteotomy site on both bones.
You Might Also Like