Surgical Anatomy and Vascularity of the Wrist

Key Takeaway
The wrist is a complex biomechanical linkage requiring precise anatomical knowledge for surgical intervention. This guide details the radiocarpal and midcarpal joints, the triangular fibrocartilage complex (TFCC), intrinsic and extrinsic ligamentous networks, and the intricate dorsal and palmar arterial arches. Mastery of these structures is essential for executing safe surgical approaches, preserving carpal vascularity, and optimizing postoperative functional recovery in complex wrist pathologies.
Osteoarticular Anatomy of the Wrist
The wrist is a highly complex, multi-articulated joint designed to balance profound mobility with structural stability. It comprises the radiocarpal, midcarpal, and distal radioulnar joints, functioning as an integrated biomechanical unit.
Radiocarpal and Midcarpal Articulations
The radiocarpal joint is formed by the articulation of the distal radius with the proximal carpal row (scaphoid and lunate) via distinct concave facets. The triquetrum articulates with the triangular fibrocartilage complex (TFCC) rather than directly with the distal ulna.
The midcarpal joint is formed by the distal concave articular surfaces of the proximal carpal row articulating with the distal carpal row (trapezium, trapezoid, capitate, hamate).
Metacarpal Articulations
The distal carpal row articulates with the metacarpal bases, dictating the mobility of the hand rays:
* Thumb (1st Metacarpal): Highly mobile saddle joint (trapeziometacarpal).
* Index and Long Fingers (2nd/3rd Metacarpals): Rigidly stable, forming the central fixed unit of the hand.
* Ring and Little Fingers (4th/5th Metacarpals): Increased mobility (15–30 degrees of flexion/extension) to facilitate power grip and cupping.
Distal Radioulnar Joint (DRUJ) and TFCC
DRUJ Osteology
The distal ulnar convexity articulates with the lesser sigmoid notch of the distal radius. The sigmoid notch accommodates the ulnar head through approximately two-thirds of its rotational arc. The distal ulna exhibits a 20-degree inclination at its articulation with the radius. The ulnar styloid is positioned dorsal to the ulnar head and extends distally.
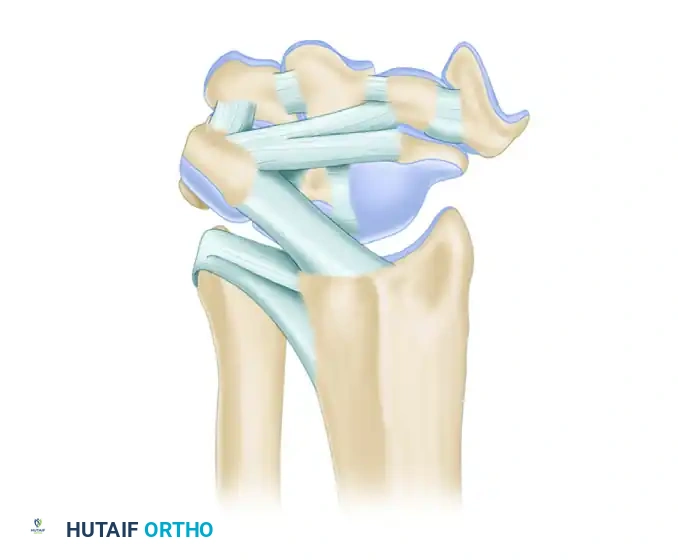
Triangular Fibrocartilage Complex (TFCC)
The TFCC is the primary stabilizer of the DRUJ and the ulnar carpus. It separates the hyaline cartilage-covered ulnar head from the ulnar styloid and carpus.
Key Components of the TFCC:
* Articular Disc: Central avascular portion, primarily load-bearing.
* Radioulnar Ligaments (Dorsal and Volar): Primary stabilizers of the DRUJ during pronation and supination.
* Ulnar Collateral Ligament (UCL): Provides ulnar-sided capsular support.
* Meniscal Homologue: Fibrous tissue connecting the disc to the triquetrum.
* Extensor Carpi Ulnaris (ECU) Subsheath: Dynamic stabilizer.
* Ulnolunate and Ulnotriquetral Ligaments: Prevent volar subluxation of the ulnar carpus.
Surgical Warning: The central portion of the TFCC is avascular and incapable of primary healing. Tears in this region require debridement. The peripheral 10-20% is vascularized and amenable to primary surgical repair.
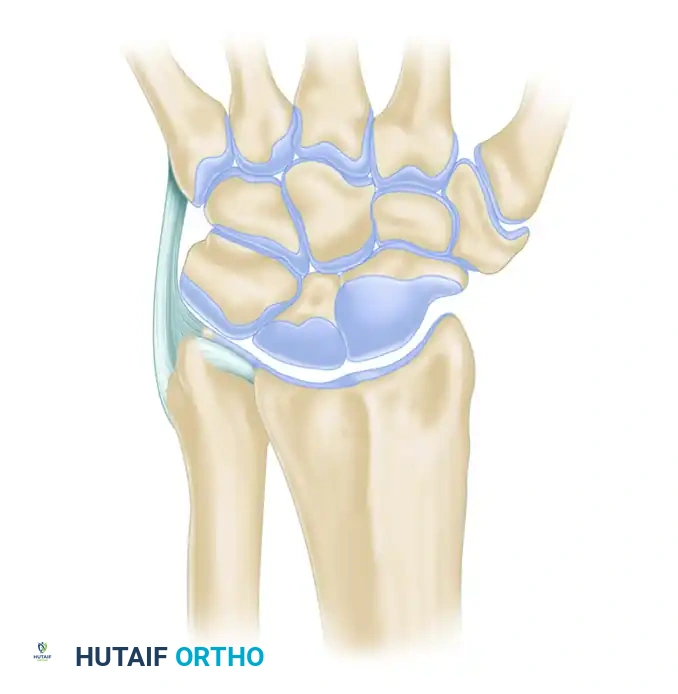
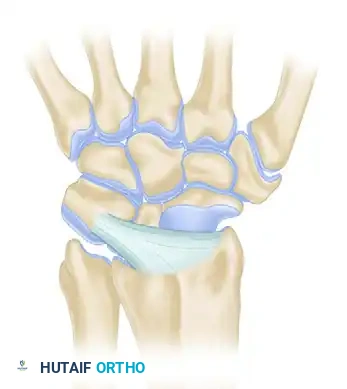
Carpal Ligamentous Architecture
Carpal stability relies entirely on its complex ligamentous network, divided into intrinsic (interosseous) and extrinsic (capsular) ligaments.
Palmar (Volar) Ligaments
Palmar ligaments are thicker and mechanically stronger than their dorsal counterparts. They form a double-V configuration that guides carpal kinematics and prevents volar intercalated segment instability (VISI) or dorsal intercalated segment instability (DISI).
Extrinsic Palmar Ligaments:
* Radioscaphocapitate (RSC): Acts as a fulcrum for scaphoid flexion.
* Long Radioscapholunate (LRSL): Primarily a neurovascular conduit rather than a mechanical stabilizer.
* Short Radiolunate (SRL): Primary stabilizer of the lunate to the radius.
Intrinsic Palmar Ligaments:
* Scapholunate (SL) Interosseous Ligament: The dorsal band is the thickest and most critical for stability.
* Lunotriquetral (LT) Interosseous Ligament: The volar band is the thickest and most critical for stability.
Dorsal Ligaments
Dorsal ligaments are thinner but crucial for preventing dorsal carpal subluxation. They are categorized by their morphological variations.
Dorsal Radiocarpal Ligaments (Four Types):



Dorsal Intercarpal Ligaments (Three Types):



Comprehensive Dorsal Perspective:
The dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments form a horizontal "V" that stabilizes the proximal row during wrist flexion.
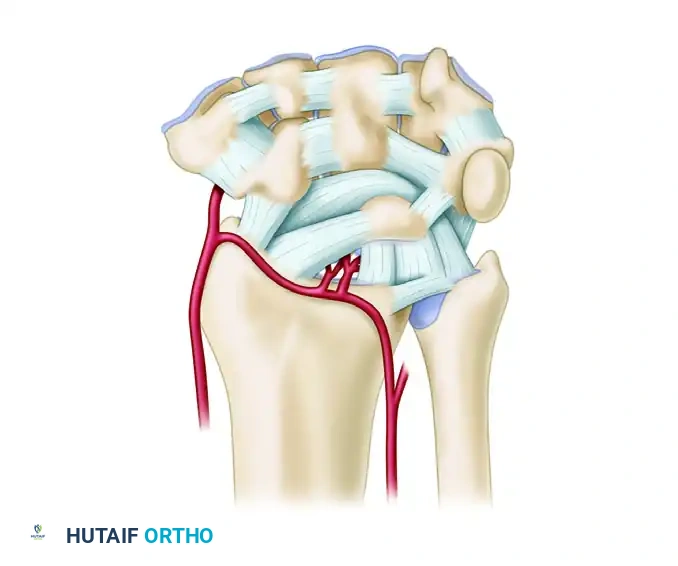
Vascular Anatomy and Circulation
The extraosseous blood supply to the carpus is derived from the terminal branches of the radial, ulnar, and anterior interosseous arteries. These form a highly redundant network of three dorsal and three palmar transverse arterial arches.
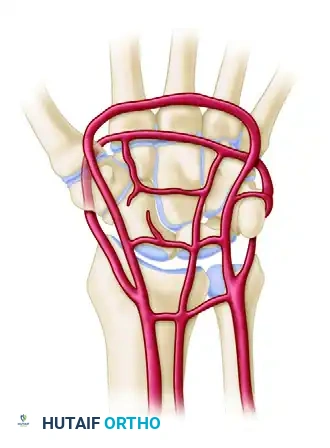
Dorsal Arterial Arches
- Dorsal Radiocarpal Arch: Located at the radiocarpal joint; supplies the proximal poles of the scaphoid, lunate, and triquetrum.
- Dorsal Intercarpal Arch: The largest dorsal arch, located between the proximal and distal rows. It supplies the distal carpal row and anastomoses with the radiocarpal arch.
- Basal Metacarpal Arch: Highly variable; supplies the distal carpal row and carpometacarpal joints.
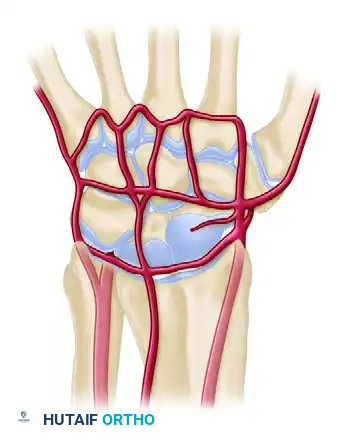
Palmar Arterial Arches
- Palmar Radiocarpal Arch: Supplies the palmar surfaces of the lunate and triquetrum.
- Palmar Intercarpal Arch: Highly variable; rarely contributes significant nutrient vessels to the intraosseous carpus.
- Deep Palmar Arch: Consistent and robust; communicates directly with the dorsal basal metacarpal arch.
Lateral Arterial Perspective
The lateral circulation highlights the critical radial artery branches supplying the scaphoid tubercle and trapezium.
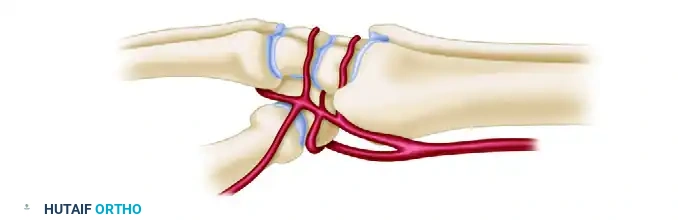
Clinical Pearl: The scaphoid and lunate rely heavily on retrograde intraosseous blood flow. The scaphoid receives 70-80% of its blood supply via dorsal ridge vessels entering distally, making proximal pole fractures highly susceptible to avascular necrosis (AVN) and nonunion.
Biomechanics and Kinematics
Load Transmission
- Neutral Variance: The radius absorbs 80% of axial loads; the ulna absorbs 20%.
- Ulnar Variance: A +2.5mm ulnar variance increases ulnar load transmission to 42%, predisposing to ulnocarpal impaction syndrome. A negative variance increases radial loading, associated with Kienböck's disease (lunate AVN).
Carpal Kinematics (Row Theory)
During wrist deviation, the proximal row acts as an intercalated segment.
* Radial Deviation: The scaphoid flexes to avoid impingement on the radial styloid, forcing the lunate and triquetrum into flexion via intrinsic ligaments.
* Ulnar Deviation: The proximal row extends. Disruption of the SL ligament uncouples the scaphoid (which flexes) from the lunate (which extends with the triquetrum), resulting in DISI.
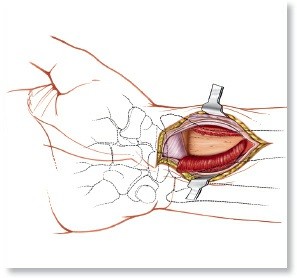
Surgical Approaches to the Wrist
Dorsal Approach to the Wrist
Indications: Proximal row carpectomy, four-corner fusion, scaphoid fixation, dorsal ganglion excision.
Positioning: Supine, arm on hand table, forearm pronated.
Step-by-Step Execution:
1. Incision: Longitudinal incision centered over Lister's tubercle.
2. Superficial Dissection: Protect dorsal sensory branches of the radial and ulnar nerves.
3. Extensor Retinaculum: Incise the 3rd extensor compartment. Transpose the Extensor Pollicis Longus (EPL) radially.
4. Deep Dissection: Elevate the 2nd compartment (ECRL/ECRB) radially and the 4th compartment (EDC/EIP) ulnarly.
5. Capsulotomy: Perform a ligament-sparing capsulotomy (e.g., Berger's dorsal capsular flap) by incising parallel to the DRC and DIC ligaments to preserve carpal stability and vascularity.
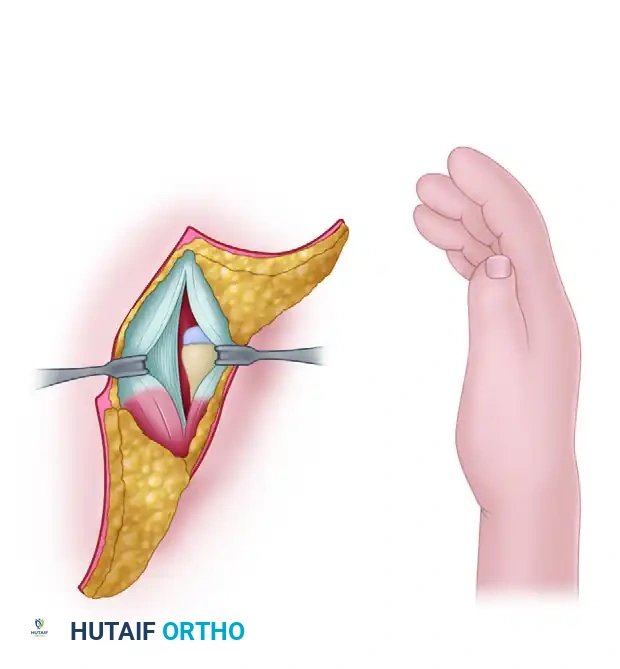
Volar Approach to the Wrist (FCR Bed)
Indications: Distal radius fractures, volar scaphoid fixation, perilunate dislocation reduction.
Positioning: Supine, arm on hand table, forearm supinated.
Step-by-Step Execution:
1. Incision: Longitudinal incision over the Flexor Carpi Radialis (FCR) tendon, zig-zagging across the wrist crease.
2. Superficial Dissection: Incise the FCR sheath. Retract the FCR tendon ulnarly to protect the median nerve.
3. Deep Dissection: Incise the floor of the FCR sheath. Identify and retract the Flexor Pollicis Longus (FPL) ulnarly.
4. Pronator Quadratus: Elevate the pronator quadratus from its radial border (L-shaped incision) to expose the distal radius.
5. Capsulotomy: If accessing the carpus, perform a volar capsulotomy, carefully preserving the robust RSC and SRL ligaments.
Clinical Indications and Pathology
Scaphoid Fractures and Nonunions
Due to the retrograde vascular supply, proximal pole fractures require prompt surgical fixation (headless compression screws). Nonunions may require vascularized bone grafting (e.g., 1,2-Intercompartmental Supraretinacular Artery [1,2-ICSRA] graft) harvested from the dorsal radius.
SLAC and SNAC Wrist
Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC) follow predictable patterns of articular degeneration:
* Stage I: Radial styloid arthrosis.
* Stage II: Entire radioscaphoid fossa arthrosis.
* Stage III: Capitolunate arthrosis. (Radiolunate joint is typically spared).
* Surgical Options: Radial styloidectomy, proximal row carpectomy (PRC), or scaphoid excision with four-corner fusion.
TFCC Pathology
- Type 1 (Traumatic): Peripheral tears (1B) are repaired arthroscopically or open. Central tears (1A) are debrided.
- Type 2 (Degenerative): Associated with ulnocarpal impaction. Treated with ulnar shortening osteotomy or arthroscopic wafer procedure.
Postoperative Protocols
Phase I: Immobilization (Weeks 0-2)
- Strict elevation to minimize edema.
- Volar resting splint or sugar-tong splint depending on DRUJ involvement.
- Immediate active range of motion (AROM) of digits to prevent tendon adhesions and CRPS.
Phase II: Early Motion (Weeks 2-6)
- Suture removal at 10-14 days.
- Transition to custom thermoplastic orthosis.
- Initiate gentle AROM of the wrist (flexion/extension, pronation/supination) if rigid fixation was achieved.
- Avoid passive stretching or loading.
Phase III: Strengthening (Weeks 6-12)
- Radiographic confirmation of union or stable repair.
- Wean from orthosis.
- Initiate progressive resistance exercises (isometric to isotonic).
- Return to heavy manual labor or sports typically restricted until 3-4 months postoperatively.
You Might Also Like