Regional Anesthesia of the Foot and Ankle: Forefoot & Ankle Block Techniques
Key Takeaway
Regional anesthesia, specifically the forefoot and ankle block, is an essential skill for orthopedic surgeons performing foot and ankle procedures. These blocks provide excellent intraoperative anesthesia and prolonged postoperative analgesia while mitigating the risks associated with general anesthesia. This guide details the precise neurovascular anatomy, pharmacological principles, and step-by-step needle placement techniques required to safely and effectively execute forefoot and ankle blocks in clinical practice.
INTRODUCTION TO REGIONAL ANESTHESIA IN FOOT AND ANKLE SURGERY
Regional anesthesia has revolutionized the perioperative management of foot and ankle pathology. For the practicing orthopedic surgeon, mastering the forefoot block and ankle block is paramount. These techniques provide profound intraoperative anesthesia, facilitate the use of a calf or ankle tourniquet, and deliver extended postoperative analgesia, thereby reducing opioid consumption and facilitating early mobilization.
When performed meticulously, regional blocks mitigate the systemic risks associated with general anesthesia, making them particularly advantageous for patients with multiple medical comorbidities. This comprehensive guide delineates the precise neurovascular anatomy, pharmacological principles, and step-by-step surgical techniques required to execute highly successful forefoot and ankle blocks.
NEUROVASCULAR ANATOMY AND BIOMECHANICS
A profound three-dimensional understanding of the pedal neurovascular arborization is the foundation of successful regional anesthesia. The foot is innervated by five primary nerves, all of which must be considered depending on the surgical site.
The Five Primary Nerves of the Foot
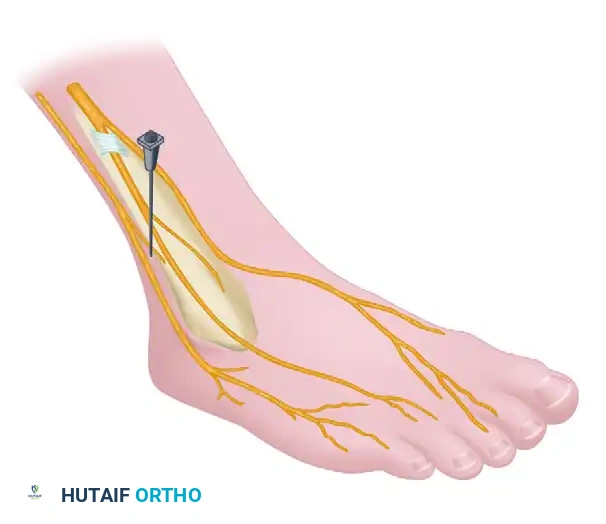
- Deep Peroneal Nerve: Courses anterior to the ankle joint, adjacent to the dorsalis pedis artery. It provides sensory innervation to the first dorsal web space.
- Superficial Peroneal Nerve: Pierces the deep fascia in the distal third of the leg, dividing into the medial and intermediate dorsal cutaneous nerves. It supplies the majority of the dorsum of the foot and toes.
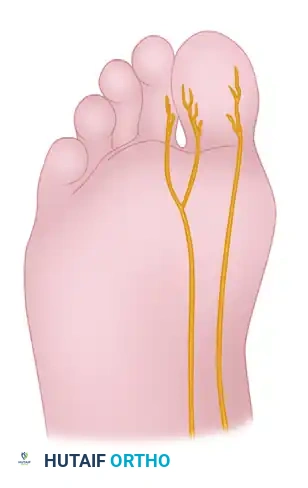
- Tibial Nerve (Medial and Lateral Plantar Nerves): Passes through the tarsal tunnel posterior to the medial malleolus. It bifurcates into the medial and lateral plantar nerves, supplying the entire plantar aspect of the foot and the plantar surfaces of the digits.
- Sural Nerve: Courses posterior to the lateral malleolus alongside the small saphenous vein, supplying the lateral margin of the foot and the fifth digit.
- Saphenous Nerve: The terminal sensory branch of the femoral nerve. It courses anterior to the medial malleolus alongside the great saphenous vein, supplying the medial column of the foot.
Arterial Landmarks
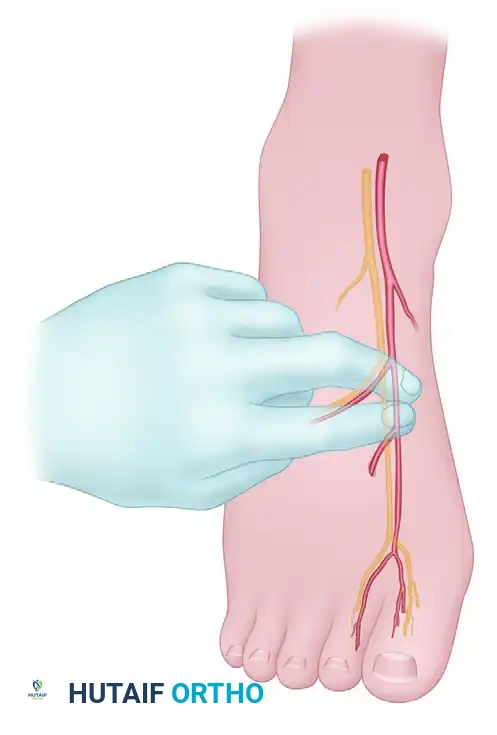
The dorsalis pedis artery is the critical landmark for the forefoot block. As it reaches the base of the first intermetatarsal space, it bifurcatates into the first dorsal intermetatarsal artery and the plantar penetrating branch. The plantar penetrating branch dives at a near right angle to communicate with the deep plantar arch—a vascular configuration biomechanically analogous to the dorsal branch of the radial artery in the hand.
Surgical Warning: Intravascular injection into the dorsalis pedis or its branches can lead to rapid Local Anesthetic Systemic Toxicity (LAST). Meticulous aspiration prior to every injection is mandatory.
PHARMACOLOGY AND PERIOPERATIVE PROTOCOLS
Anesthetic Agents and Dosing
A synergistic mixture of short-acting and long-acting local anesthetics is recommended to achieve rapid onset and prolonged duration.
* Short-Acting: 1% or 2% Lidocaine (Onset: 5-10 minutes; Duration: 1-2 hours).
* Long-Acting: 0.5% Bupivacaine or 0.5% Ropivacaine (Onset: 15-30 minutes; Duration: 4-8 hours).
In most adult patients, a total volume of 30 to 40 mL of a 50/50 mixture (e.g., 1% Lidocaine and 0.5% Bupivacaine) is sufficient for a complete ankle block. However, the total dose must be strictly calculated based on the patient's weight to avoid exceeding maximum recommended doses (e.g., 4.5 mg/kg for Lidocaine without epinephrine; 2.5 mg/kg for Bupivacaine).
The Role of Epinephrine
Clinical Pearl: We do not routinely use epinephrine with the anesthetic solution except as a long-acting postoperative analgesic supplementing general anesthesia in complex hindfoot procedures. When utilized, the concentration should be 0.5% Bupivacaine with 1:200,000 epinephrine.
CRITICAL RULE: Epinephrine must never be used distal to the midfoot. The digital arteries are end-arteries; epinephrine-induced vasospasm in the forefoot or digits can result in irreversible ischemia and subsequent necrosis.
Preoperative Patient Optimization
The same rigorous anesthetic precautions applied to general anesthesia must be enforced for regional blocks:
* Comprehensive history and physical examination.
* Appropriate preoperative laboratory data.
* Strict adherence to NPO guidelines (abstaining from food or drink 8 to 10 hours prior to surgery).
* Diabetic Exception: If minor procedures (e.g., nail surgery, single hammer toe correction, or tenotomy) are planned for a diabetic patient under local anesthesia, allowing a limited meal a few hours prior to surgery is reasonable to prevent hypoglycemia, provided the anesthesia team concurs.
* Patients must be counseled that general anesthesia or conscious sedation will be utilized if the regional block is incomplete or fails.
SURGICAL TECHNIQUE: THE FOREFOOT BLOCK
The forefoot block is highly efficacious for procedures involving the hallux, lesser toes, and distal metatarsals, such as hallux valgus correction, hammer toe reconstruction, and neuroma excision.
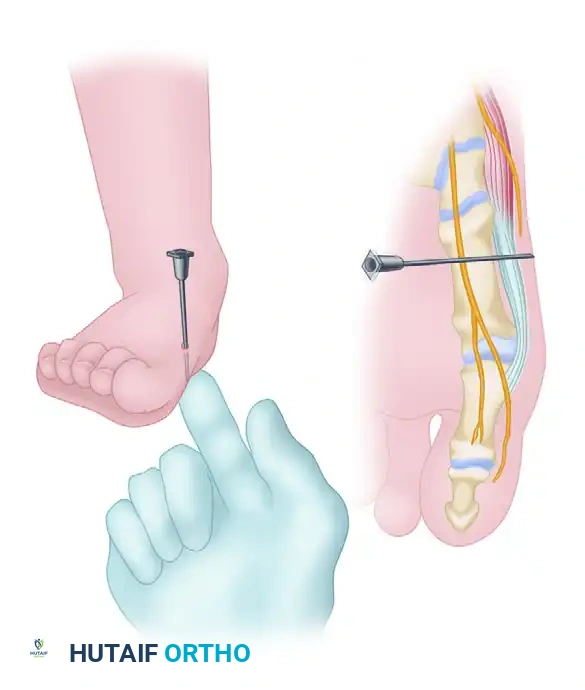
Step 1: Targeting the Deep Peroneal Nerve
Begin by palpating the dorsalis pedis artery as it courses distally and reaches the first intermetatarsal space. The deep peroneal nerve, which supplies the first web space, closely accompanies this artery.
Utilizing a 1.5-inch, 25-gauge needle, carefully avoid the artery. Inject 2 to 3 mL of the short-acting/long-acting anesthetic mixture subcutaneously to anesthetize the deep peroneal nerve.
Step 2: Blocking the Superficial Peroneal Branches (Lateral)
If a second or third hammer toe procedure is planned, do not withdraw the needle completely. From the same entrance point, redirect the needle laterally, passing just beneath the dorsal veins.
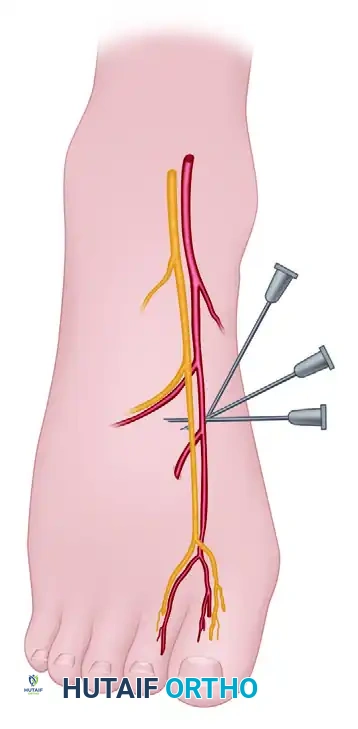
Advance the needle to block the common digital branches of the superficial peroneal nerve supplying the second (and third, if necessary) intermetatarsal spaces. An injection of an additional 2 to 3 mL is typically sufficient.
Step 3: Blocking the Medial Hallucal Branch
Return the needle to the original entrance point, but now direct it medially. Maintain a trajectory immediately beneath the dorsal veins and superficial to the extensor hallucis longus (EHL) tendon.
This maneuver blocks the medial hallucal branch of the dorsomedial superficial peroneal nerve—the sensory branch most frequently encountered dorsal and medial to the medial eminence ("bunion") during hallux valgus surgery. Conclude this dorsal sensory block at the dorsomedial aspect of the forefoot, approximately 1 cm distal to the first metatarsomedial cuneiform articulation. At this stage, 6 to 8 mL of anesthetic has been administered.
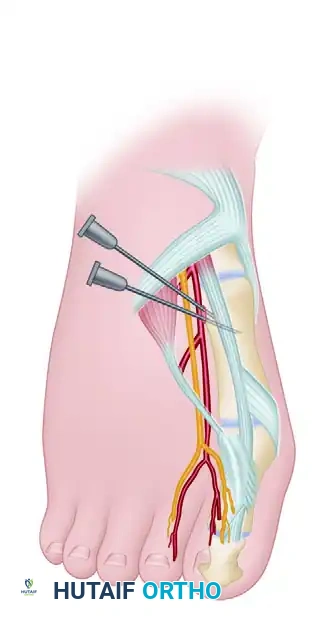
Step 4: Plantarward Progression
Entering the newly anesthetized area on the dorsomedial aspect of the forefoot, redirect the needle plantarward. Proceed through the subcutaneous space, remaining superficial to the abductor hallucis muscle, until the plantar surface of the medial side of the foot is reached.
Clinical Pearl: Instilling a small amount of anesthetic agent continuously as the needle progresses plantarward (hydrodissection) significantly lessens patient discomfort.
Step 5: Anesthetizing the Proper Plantar Branch
The proper plantar branch to the medial side of the hallux becomes superficial at this level. It penetrates the deep fascia over the abductor hallucis and flexor hallucis brevis near the first metatarsomedial cuneiform articulation.
Palpate the tip of the needle subcutaneously on the plantar aspect. Once felt, withdraw the needle 2 to 3 mm to ensure it is not intradermal, and instill 2 to 3 mL of the anesthetic agent.
Step 6: Completing the First Web Space Block
To complete the block, you must anesthetize the common digital branch of the medial plantar nerve supplying the first web space. Return to the dorsal surface at the base of the first intermetatarsal space.
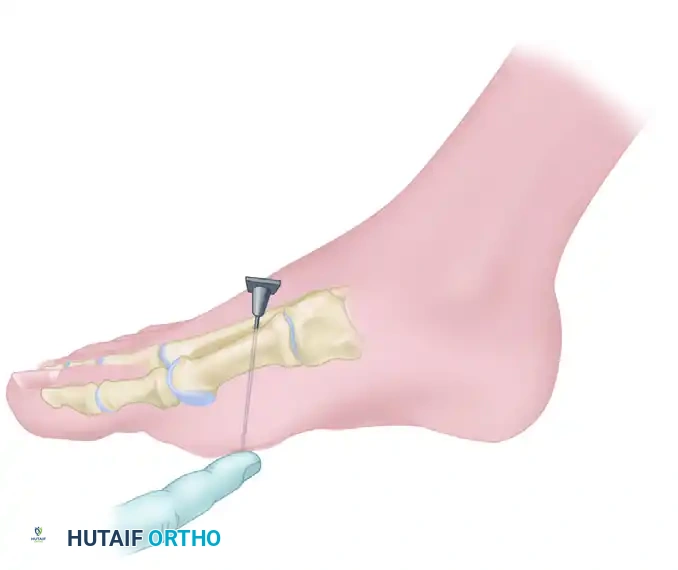
Step 7: Navigating the Arterial Bifurcation
At the base of the first intermetatarsal space, the dorsalis pedis artery bifurcates into the first dorsal intermetatarsal artery and the plantar penetrating branch.

To safely avoid this arterial bifurcation:
1. Move the needle entrance point distally by 1 to 1.5 cm.
2. Angle the needle obliquely at 10 to 20 degrees relative to the skin.
3. Pass the 1.5-inch, 25-gauge needle plantarward between the first and second metatarsals until the tip is palpable subcutaneously on the plantar surface.
4. Inject small amounts of anesthetic during advancement to minimize pain.
5. Withdraw the tip 2 to 3 mm from the plantar skin and instill 4 to 5 mL of solution.
If a hammer toe procedure is planned for the lesser digits, repeat this exact technique between the second and third metatarsals. This provides robust anesthesia for the third toe. Occasionally, supplementing the block with 1 mL of anesthetic directly at the base of the third toe near the web space may be required for complete coverage.
SURGICAL TECHNIQUE: THE ANKLE BLOCK
The ankle block is a highly versatile regional technique. Numerous hindfoot and midfoot procedures can be performed under ankle block anesthesia combined with a calf or rubber esmarch tourniquet.
Indications for Ankle Block
- Open reduction and internal fixation (ORIF) of tarsometatarsal (Lisfranc), midtarsal, and talocalcaneal injuries.
- Osteotomies and arthrodeses distal to the malleoli.
- Tarsal tunnel decompression.
- Excision of calcific deposits within the Achilles tendon insertion.
- Closed reduction of ankle fracture-dislocations.
Evidence-Based Efficacy
The reliability of the ankle block is well-documented in orthopedic literature. Rudkin et al. reported a 95% success rate in a prospective analysis of 1,000 patients undergoing foot or ankle surgery with ankle block anesthesia. Crucially, they noted that the frequency of anesthetic failure was drastically reduced when the time between block administration and surgical incision was 20 minutes or greater, allowing adequate time for neural blockade.
Furthermore, White et al. compared intra-articular blocks to conscious sedation for the closed reduction of ankle fracture-dislocations. They demonstrated that regional blockade provided superior, sufficient analgesia. The average time for reduction and splinting was significantly faster in the block group (63.8 minutes) compared to the sedation group (81.5 minutes), highlighting the efficiency of regional techniques in acute trauma settings.
Execution and Timing
Once the ankle block is administered (targeting the tibial, deep peroneal, superficial peroneal, sural, and saphenous nerves circumferentially around the ankle), the time required to formally prepare and drape the patient is usually sufficient to allow the block to take full effect. Always verify the absence of sharp sensation in all five nerve distributions prior to tourniquet inflation or skin incision.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Postoperative Care
Patients who receive a forefoot or ankle block will experience sensory and motor deficits lasting anywhere from 4 to 12 hours, depending on the concentration of Bupivacaine or Ropivacaine used.
* Weight-Bearing: Patients must be strictly counseled regarding their weight-bearing status. An insensate foot is at high risk for unrecognized trauma or Charcot-like acute breakdown if loaded improperly. Crutches, walkers, or a controlled ankle motion (CAM) boot must be utilized as dictated by the surgical procedure.
* Rebound Pain: The transition from complete regional anesthesia to normal sensation can cause sudden "rebound pain." Patients should be instructed to take their first dose of oral postoperative analgesics before the block completely wears off (typically when they first feel a tingling sensation returning to the toes).
Complications and Pitfalls
- Intravascular Injection: Can lead to LAST. Symptoms include perioral numbness, metallic taste, tinnitus, visual disturbances, seizures, and cardiovascular collapse. Immediate cessation of injection, airway management, and administration of 20% lipid emulsion therapy are required.
- Nerve Injury: Direct intraneural injection can cause severe, lasting neuropathy. If the patient reports a sharp, electric "paresthesia" during needle advancement, withdraw the needle 1-2 mm before injecting. Injection should never require high resistance.
- Hematoma: Puncture of the dorsalis pedis or its branches can cause a localized hematoma. Apply direct pressure for 3-5 minutes if arterial puncture occurs.
- Ischemia: As reiterated, the use of epinephrine distal to the midfoot is an absolute contraindication due to the risk of digital gangrene.
By adhering to these strict anatomical landmarks and pharmacological guidelines, the orthopedic surgeon can utilize forefoot and ankle blocks to maximize surgical efficiency, optimize patient comfort, and elevate the standard of perioperative care.
You Might Also Like