Mastering Digital and Peripheral Nerve Blocks in Hand Surgery

Key Takeaway
Digital nerve blocks provide profound anesthesia for surgical procedures of the hand and digits. By targeting the proper digital nerves proximal to the web space, surgeons can achieve excellent pain control while minimizing ischemic complications. This guide details evidence-based techniques for digital and peripheral nerve blocks, safe tourniquet application, and optimal patient positioning to ensure successful surgical outcomes in operative orthopedics.
INTRODUCTION TO REGIONAL ANESTHESIA IN HAND SURGERY
Regional anesthesia is a cornerstone of operative orthopedics, particularly in hand and upper extremity surgery. The ability to achieve profound, localized anesthesia without the systemic risks of general anesthesia allows for safer interventions, faster recovery, and the unique advantage of intraoperative patient cooperation. Digital nerve blocks and peripheral nerve blocks at the wrist provide excellent anesthesia for a vast array of procedures, ranging from simple laceration repairs and foreign body removals to complex tenolyses, capsulotomies, and fracture fixations.
This comprehensive guide delineates the anatomical foundations, pharmacological principles, and step-by-step surgical techniques required to master digital and peripheral nerve blocks. Furthermore, it addresses the critical application of digital tourniquets, ensuring that hemostasis is achieved safely without compromising the delicate vascular supply of the digits.
PHARMACOLOGIC AGENTS AND PRINCIPLES
The selection of the appropriate local anesthetic agent is dictated by the anticipated duration of the surgical procedure and the required postoperative analgesia.
- Lidocaine (1% or 2%): Provides rapid onset (3–5 minutes) with a moderate duration of action (1–2 hours). It is the workhorse for brief procedures.
- Bupivacaine (0.25% or 0.5%): Features a slower onset (10–20 minutes) but offers a significantly prolonged duration of action (4–8 hours), making it ideal for complex procedures and extended postoperative pain control.
- Ropivacaine (0.5%): Offers a similar duration to bupivacaine but with a potentially lower risk of cardiac and central nervous system toxicity.
Clinical Pearl: We rarely use epinephrine in the local anesthetic agent in the digits for routine blocks, although extensive literature on the WALANT (Wide Awake Local Anesthesia No Tourniquet) technique has proven that epinephrine (typically 1:100,000 or 1:200,000) can be used safely in the hand and digits. If epinephrine-induced ischemia becomes prolonged, phentolamine (1–2 mg in 1–5 mL of saline) can be injected locally to reverse the vasoconstriction.
PERIPHERAL NERVE BLOCKS AT THE WRIST
The median, radial, and ulnar nerves can be effectively blocked at the elbow and wrist. Wrist blocks are extremely helpful for brief procedures and are particularly advantageous when the surgeon needs to observe active motion of the fingers during surgery, such as during tenolyses and capsulotomies.
When utilizing a wrist block, a proximal arm tourniquet may not be required, or it may be used only for a short period (usually ≤ 30 minutes). However, if the patient is adequately sedated and the tourniquet is well-padded, it can be tolerated for longer durations. It is essential to possess a precise understanding of the location of the respective nerves before attempting regional blocks to avoid intraneural injection and subsequent neuropathy.
Ulnar Nerve Block
The ulnar nerve at the wrist lies deep to the flexor carpi ulnaris (FCU) tendon and medial to the ulnar artery. The dorsal sensory branch of the ulnar nerve branches off approximately 5 cm proximal to the wrist crease.
Technique:
1. Identify the FCU tendon at the proximal wrist crease.
2. Insert the needle just radial or ulnar to the FCU, directing it beneath the tendon.
3. Aspirate to ensure the needle is not within the ulnar artery.
4. Inject 3 to 5 mL of local anesthetic to block the volar branches.
5. To capture the dorsal sensory branch, deposit a subcutaneous wheal of anesthetic extending dorsally toward the ulnar styloid.
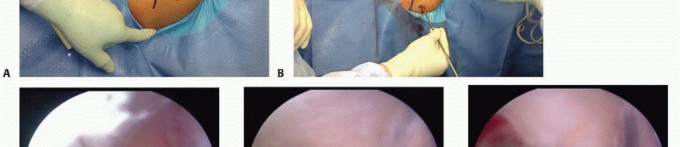
FIGURE 64-7A: Technique of peripheral nerve blocks. Ulnar nerve, superficial branch infiltration.
Median Nerve Block
The median nerve is located between the palmaris longus (PL) and the flexor carpi radialis (FCR) tendons. It lies superficial to the flexor digitorum superficialis tendons.
Technique:
1. Identify the PL and FCR tendons at the proximal wrist crease. If the PL is absent, the nerve lies approximately 1 cm ulnar to the FCR.
2. Insert the needle perpendicular to the skin between these two tendons.
3. Advance the needle until it pierces the deep fascia (usually 0.5 to 1 cm deep). If the patient reports paresthesia, withdraw slightly to avoid intraneural injection.
4. Inject 3 to 5 mL of local anesthetic.
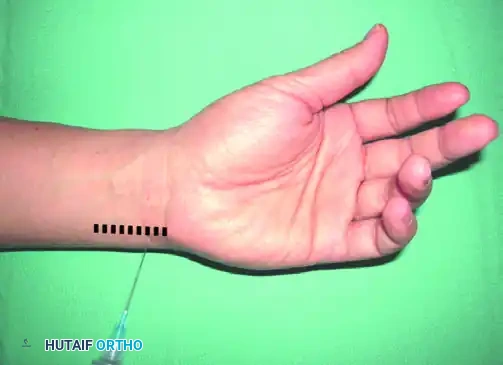
FIGURE 64-7B: Technique of peripheral nerve blocks. Median nerve infiltration.
Superficial Radial Nerve Block
The superficial branch of the radial nerve provides sensation to the dorsal-radial aspect of the hand. It emerges from beneath the brachioradialis approximately 7 cm proximal to the wrist and branches extensively in the subcutaneous tissue.
Technique:
1. Because the nerve arborizes widely, a field block is required.
2. Begin the injection at the level of the radial styloid.
3. Infiltrate 5 to 7 mL of local anesthetic subcutaneously in a V-shaped or transverse band extending from the FCR tendon volarly to the extensor carpi radialis longus dorsally.
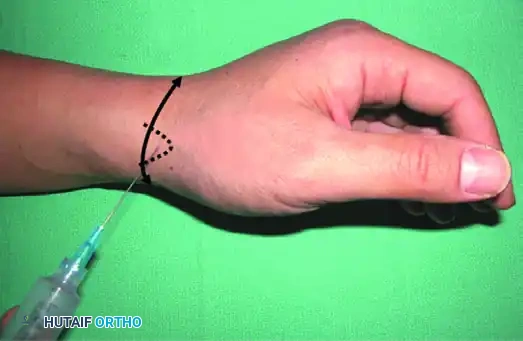
FIGURE 64-7C: Technique of peripheral nerve blocks. Superficial radial nerve field block.
DIGITAL NERVE BLOCKS
Digital nerve blocks provide excellent, profound anesthesia for procedures on the fingers, such as fracture reduction, nail bed repair, and foreign body extraction.
Surgical Warning: Usually, perineural injection around the digital nerves proximal to the finger web spaces is a safer technique than injection of the nerves in a circumferential ring at the base of the fingers. Because severe ischemia and subsequent necrosis may develop after injection of an anesthetic agent in a tight circle around the base of the finger (the "ring block"), this circumferential technique should be strictly avoided.
Traditional Web Space Block
The traditional approach targets the common digital nerves just before they bifurcate into the proper digital nerves, or targets the proper digital nerves directly in the web space.
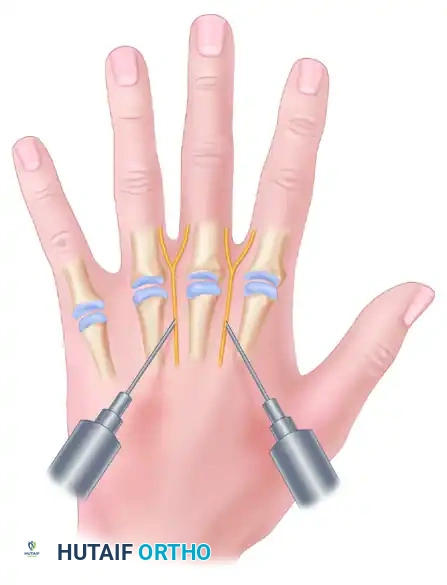
FIGURE 64-8A: Digital nerve blocks. Volar approach targeting the common digital nerves.
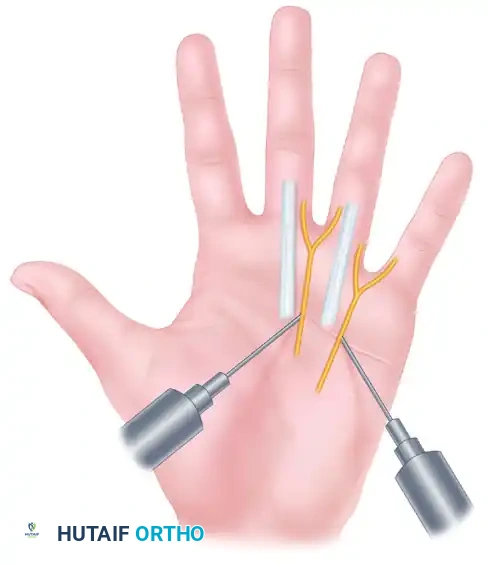
FIGURE 64-8B: Digital nerve blocks. Dorsal approach targeting the proper digital nerves.
Technique:
1. Dorsal Approach: Insert a 25- or 27-gauge needle into the dorsal web space, directing it volarly toward the neurovascular bundle. Inject 1 to 2 mL of anesthetic. Withdraw the needle slightly and redirect it dorsally to block the dorsal sensory branches, injecting another 1 mL. Repeat on the opposite side of the digit.
2. Volar Approach: Insert the needle at the proximal palmar crease, directing it toward the common digital nerve. Inject 2 to 3 mL of anesthetic. This approach often blocks the adjacent sides of two fingers simultaneously.
Transthecal (Flexor Sheath) Block
The transthecal block utilizes the flexor tendon sheath as a conduit for the anesthetic agent. The anesthetic diffuses through the synovial sheath to bathe the adjacent proper digital nerves.
Technique:
1. Palpate the flexor tendon at the level of the distal palmar crease (A1 pulley region).
2. Insert the needle at a 45-degree angle until it contacts the flexor tendon, then withdraw slightly.
3. Inject 2 to 3 mL of anesthetic. The fluid should flow easily; resistance indicates the needle is within the tendon substance.
Note: While effective, digital blocks using a transthecal approach have shown no distinct advantage compared with the traditional digital block technique in large comparative studies.
Single Volar Injection Technique
For procedures that require anesthesia from the mid-middle phalanx distally (e.g., nail bed repairs, distal interphalangeal joint fusions, and fingertip amputations), digital anesthesia can be easily and rapidly achieved by a single volar injection technique.

FIGURE 64-9A: Just proximal to the palmar digital crease, through pinched skin, 3 to 5 mL of local anesthetic is injected superficial to the flexor sheath.

FIGURE 64-9B: Anesthesia achieved (colored area) from the block of proper and dorsal sensory digital nerve branches. Note: if more proximal anesthesia is needed, an additional block can be given at the metacarpophalangeal joint dorsally.
Technique:
1. Pinch the skin just proximal to the palmar digital crease to minimize injection pain.
2. Insert the needle centrally and inject 3 to 5 mL of local anesthetic superficial to the flexor sheath.
3. The volume of the anesthetic will spread circumferentially within the subcutaneous tissue, effectively blocking both the proper volar digital nerves and the dorsal sensory branches.
LOCAL INFILTRATION
Local infiltration of an anesthetic agent may be used for more proximal conditions in the hand or forearm that do not require deep, extensive anesthesia. This is particularly useful for superficial mass excisions, trigger finger releases, or superficial laceration repairs. The anesthetic is injected directly into the subcutaneous tissue surrounding the surgical site. Care must be taken to aspirate prior to injection to avoid intravascular administration, and the total dose must be calculated to prevent systemic local anesthetic toxicity (LAST).
DIGITAL TOURNIQUETS AND HEMOSTASIS
Achieving a bloodless surgical field is paramount in hand surgery to identify delicate neurovascular structures and perform precise repairs. If hemostasis is required, several techniques can be employed to create safe ischemia in the digit.
Traditional Methods
Traditionally, a Penrose drain or a French rubber catheter applied tightly around the base of the finger has provided satisfactory and safe ischemia. Commercially available finger tourniquets (e.g., T-Ring) and the finger of a sterile rubber glove cut to allow it to be rolled onto the finger as an exsanguinating tourniquet are also highly effective tools.
Pitfall: Pressures achieved beneath these improvised tourniquets cannot be determined accurately. Extreme caution is advised. Excessive pressure can cause irreversible crush injury to the digital neurovascular bundles.
Vascular Precautions
At times, especially in the elderly and in patients with underlying vascular disorders in the fingers (e.g., Raynaud disease, severe atherosclerosis, long-standing diabetes mellitus), vascular insufficiency may develop in the digit postoperatively. Care should be taken when using digital tourniquets in these patients. The duration of digital tourniquet application should strictly not exceed 20 to 30 minutes without a reperfusion interval.
The Esmarch Wrap Technique
A broad-based finger tourniquet can be easily fabricated from an Esmarch wrap, which usually accompanies upper extremity surgical packages. This technique provides both exsanguination and a broad area of compression, reducing the risk of focal nerve crush.
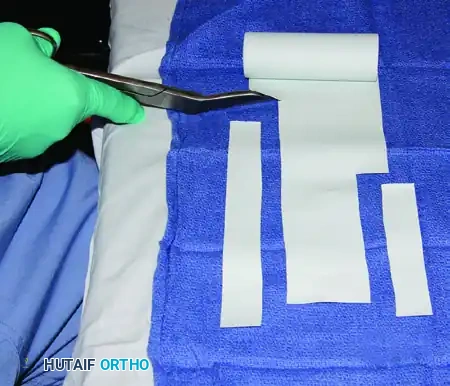
FIGURE 64-10A: Long and short strips, 2.5 cm wide, are cut from opposite sides of an Esmarch bandage.

FIGURE 64-10B: The short strip is loosely applied across the finger base and is held in place with a curved hemostat. The longer strip is used to exsanguinate the finger by wrapping it tightly from distal to proximal.

FIGURE 64-10C: Tension is applied to the short section, and the hemostat is applied close to the dorsal skin with the two limbs of the short Esmarch section fully opposed. The distal exsanguinating wrap is then removed.
SURGICAL PREPARATION AND POSITIONING
Proper preparation of the surgical field is critical to minimize skin reactions and prevent surgical site infections.
- Positioning: The patient is positioned supine with the operative arm extended on a well-padded hand surgery table (arm board).
- Draping: A waterproof sheet is placed on the hand table, followed by a sterile drape sheet. Combinations of sterile towels and sheets are applied, leaving exposed only the upper extremity, hand, and any other areas that may require access during the operation (e.g., iliac crest for bone graft).
- Surgeon Ergonomics: The gloves used in the initial preparation of the surgical field are removed. The surgeon dons a fresh sterile gown and gloves and sits down, usually on the axillary side of the forearm, allowing optimal visualization and ergonomic access to the hand.
- Lighting and Marking: The operating lights are adjusted to eliminate shadows, and the planned skin incisions are carefully outlined with a sterile surgical marker prior to exsanguination and tourniquet inflation.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Following procedures performed under regional digital or wrist blocks, patients must be educated regarding the expected duration of anesthesia.
- Protection of the Insensate Digit: Patients must be warned to protect the anesthetized digit from extreme temperatures and inadvertent trauma until full sensation returns.
- Ischemic Complications: If a digital tourniquet was used, the surgeon must confirm brisk capillary refill immediately upon tourniquet removal. If vasospasm occurs, warming the hand, applying topical vasodilators, or performing a digital block with plain lidocaine (to induce sympathectomy) may be required.
- Systemic Toxicity: Although rare with the small volumes used in digital blocks, surgeons must remain vigilant for signs of Local Anesthetic Systemic Toxicity (LAST), including perioral numbness, tinnitus, visual disturbances, and arrhythmias. Immediate access to 20% lipid emulsion therapy must be available in the operative setting.
By adhering to these rigorous anatomical and technical principles, the orthopedic surgeon can consistently achieve safe, effective regional anesthesia, facilitating optimal surgical outcomes in the operative management of the hand and upper extremity.
You Might Also Like