Upper Extremity Anesthesia: An Orthopaedic Surgeon's Masterclass in Perioperative Management
Key Takeaway
Join us in the OR for a masterclass on upper extremity anesthesia. We'll meticulously review preoperative planning, intricate surgical anatomy, and real-time intraoperative execution of regional and general anesthesia techniques. Learn critical pearls, avoid pitfalls, and optimize patient outcomes from a surgeon's perspective. This guide covers everything from nerve blocks to managing complex patient comorbidities like rheumatoid arthritis.
Welcome, fellows, to the operating theater. Today, we're not just discussing surgical technique, but rather, the critical, often underappreciated, role of anesthetic considerations in ensuring successful outcomes for our upper extremity cases. As orthopaedic surgeons, our focus is naturally on the bone and soft tissue, but the patient's journey, from preoperative assessment to postoperative recovery, is profoundly influenced by the anesthetic plan. Understanding this symbiotic relationship is paramount for any master surgeon.
Preoperative Evaluation: Laying the Foundation for Success
Before we even consider an incision, a meticulous preoperative evaluation is non-negotiable. This is where we identify potential challenges and collaborate with our anesthesiology colleagues to formulate a robust plan.
The Rheumatoid Arthritis Patient: A Unique Challenge
Patients with advanced rheumatoid arthritis (RA) present a complex scenario that demands our utmost attention. This isn't just a joint disease; it's a systemic inflammatory process with widespread implications.
- Cervical Spine Instability: A critical concern is the potential for atlantoaxial subluxation. This instability arises from erosion of the transverse ligament at the odontoid process of C2, which is normally tethered to C1. This C1-C2 instability can lead to dynamic subluxation, placing the spinal cord at risk of compression and potential paralysis.
- Our Protocol: For any RA patient, especially those with advanced disease, preoperative flexion and extension lateral cervical spine radiographs are absolutely mandatory. We need to rule out instability. If significant instability is identified, a cervical fusion, often C1 to the occiput, may be required before we proceed with any other orthopaedic procedure, particularly those requiring specific head positioning. The risk of neurological catastrophe during intubation or positioning is simply too high to ignore.
- Airway Management Challenges: Beyond the cervical spine, RA can cause anatomic changes in the temporomandibular joint (TMJ) and arytenoids, leading to limited jaw opening and neck mobility. This can make standard endotracheal intubation extremely difficult, even impossible.
- Anesthetic Collaboration: In such cases, our anesthesiologists may need to employ awake fiberoptic bronchoscope-guided intubation. This is a highly specialized technique that avoids general anesthesia until the airway is secured. We must be prepared for this extended induction time and ensure our OR schedule accommodates it.
- Systemic Comorbidities: Remember, RA is a systemic disease.
- Cardiovascular Disease: Atherosclerosis occurs at an accelerated rate in RA patients, significantly increasing their risk of myocardial infarction and cerebrovascular accident. The rate of cardiovascular morbidity and mortality is notably higher than in the general population.
- Respiratory Performance: The lungs can also be affected, leading to restrictive pulmonary disease.
- Our Due Diligence: For severe RA patients, we must advocate for a comprehensive preoperative workup, including an echocardiogram, cardiac stress testing, and pulmonary function testing. This helps us understand their physiological reserve and mitigate risks.
Trauma Patients: Urgency and Unpredictability
Orthopaedic trauma cases often present as surgical emergencies, demanding rapid decision-making under pressure.
- Uncleared Cervical Spine: In the trauma setting, an uncleared cervical spine necessitates in-line manual stabilization during endotracheal intubation, regardless of whether the patient is awake or asleep. This is a critical safety measure we must ensure is implemented.
- Radiologic Evaluation: The urgency of trauma may sometimes require general anesthesia before complete radiologic evaluations can be finalized. This underscores the importance of a rapid, focused assessment.
- Factors Influencing Anesthesia Choice: General anesthesia is frequently chosen for trauma due to:
- Involvement of multiple extremities.
- Unknown duration of the procedure.
- The need to assess postoperative neurologic function immediately.
- Surgeon or patient preference.
Pediatric Patients: A Special Population
Operating on children requires a unique approach, especially regarding anesthesia.
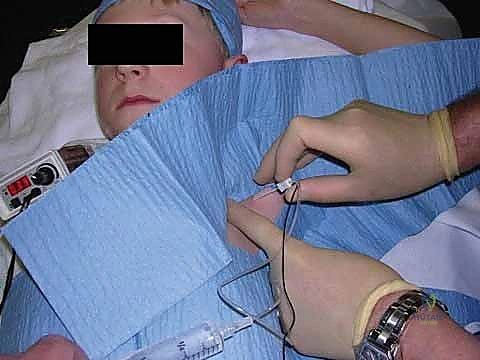
- Emotional and Intellectual Maturity: Children often lack the maturity to remain conscious and cooperative during a procedure, making general anesthesia a common choice.
FIG 1 • Pediatric axillary brachial plexus block.
* Regional Anesthesia in Pediatrics: While general anesthesia is prevalent, regional techniques offer significant benefits. However, they carry specific considerations:
* Needle Size: Historically, smaller needles for pediatric regional techniques were less available. Modern advancements have improved this, but continuous blocks often still utilize adult equipment, which is not always optimal.
* Loss of Patient Feedback: Performing regional anesthesia in a child already under general anesthesia increases the risk of neural injury due to the absence of patient feedback (pain, paresthesia).
* Nerve Injury Risk: While nerve blocks under anesthesia have caused severe injury in adults, these incidents are less common in children.
* Ultrasound Guidance: Ultrasound-guided nerve blocks during general anesthesia are crucial. Direct visualization of neural targets significantly reduces the risk of nerve injury.
* Local Anesthetic Toxicity: Pediatric patients require cautious local anesthetic selection and administration to avoid toxicity. Dosing must be precise and weight-based.
* Dilute Local Anesthetics: Due to incomplete myelination of neural fibers in children, which permits greater local anesthetic penetration, continuous peripheral nerve catheters may be dosed with dilute local anesthetics (e.g., bupivacaine or ropivacaine 0.1%) to decrease the risk of systemic toxicity. Recommended infusion rates often begin at 0.15 mL/kg per hour of bupivacaine 0.25%.
* Fasting Guidelines for Pediatric Patients: Strict adherence to fasting guidelines is essential to prevent aspiration.
* Age-Specific Guidelines:
* < 6 months: 4 hours for milk/solids, 2 hours for clear liquids.
* 6-36 months: 6 hours for milk/solids, 3 hours for clear liquids.
* > 36 months: 8 hours for milk/solids, 3 hours for clear liquids.
Fasting Guidelines for Pediatric Patients
| Age | Milk and Solids (hr) | Clear Liquids (hr) |
|---|---|---|
| < 6 mo | 4 | 2 |
| 6–36 mo | 6 | 3 |
| > 36 mo | 8 | 3 |
Pediatric Doses of Clinical Characteristics of Commonly Used Local Anesthetics*
| Local Anesthetic | Concentration (%) | Usual Doses (mg/kg) | Maximum Dose, Plain † (mg/kg) | Maximum Dose, with Epinephrine † (mg/kg) | Latency (min) | Duration of Effects (hr) |
|---|---|---|---|---|---|---|
| Lidocaine | 0.5–2.0 | 5 | 7.5 | 10 | 5–15 | 0.75–2.0 |
| Prilocaine | 0.5–1.5 | 5 | 7.0 | 10 | 15–25 | 0.75–2.0 |
| Mepivacaine | 0.5–1.5 | 5–7 | 8.0 | 10 | 5–15 | 1–1.25 |
| Bupivacaine | 0.25–0.5 | 2 | 2.5 | 3 | 15–30 | 2.5–6.0 |
| Ropivacaine | 0.2–10.0 | 3 | 3.5 | NA | 7–20 | 2.5–5.0 |
| *Data are not applicable to spinal anesthesia or intravenous regional anesthesia. † Maximum doses vary; free and unbound local causes toxicity, not total dose. Do not apply if previously injected or local anesthetic infusion maintained. |
Anticoagulation Guidelines: A Team Approach
Managing patients on anticoagulants requires precise coordination with anesthesia. The risk of hematoma formation, particularly with neuraxial or deep peripheral nerve blocks, must be carefully weighed against the benefits of regional anesthesia.
American Society of Regional Anesthesia Guidelines for Anticoagulation
| Medication | Discontinuation Recommendation |
|---|---|
| Herbal medications: ginkgo, ginseng, and garlic (greatest effect) | No discontinuation |
| Nonsteroidal anti-inflammatories and acetaminophen | No discontinuation |
| Ticlopidine and clopidogrel | 14 days |
| Heparin SQ | No discontinuation |
| IV Heparin | Stop and 1 hour after block |
| Low-molecular-weight heparin | 12 hours after last dose |
| Coumadin | Discontinue 4 days |
| Thrombolytics | Avoid regional |
Anesthesia Selection for Upper Extremity Procedures: Our Intraoperative Strategy
The choice of anesthesia for arm and hand surgery is rarely a one-size-fits-all decision. It can be general, regional, or, most commonly, a combination of techniques. Our anesthetic plan is a carefully considered strategy, balancing patient safety, surgical needs, and postoperative recovery.
The Case for General Anesthesia
While regional techniques offer many advantages, general anesthesia remains a vital tool in our armamentarium.
- Reliability: It's often easier to apply, with virtually no anesthetic failures in terms of providing unconsciousness and immobility.
- Procedure Duration and Positioning: For long procedures or those requiring uncomfortable or sustained positions (e.g., specific shoulder positions), general anesthesia provides the necessary unconsciousness and muscle relaxation.
- Patient Demographics: Pediatric and mentally retarded patients are often easier to manage under general anesthesia.
- Cadaveric Conditions: For procedures requiring absolute immobility, such as microsurgery or complex reconstructions, general anesthesia ensures a "cadaveric" surgical field.
- Multiple Surgical Sites: When we need to perform surgery on the upper extremity and harvest a graft from a different anatomic location (e.g., iliac crest, fibula), general anesthesia allows for simultaneous access without patient discomfort.
- Postoperative Neurologic Assessment: In some cases, we need to assess nerve function immediately after surgery. If a regional block would obscure this, general anesthesia is preferred.
- Efficient Recovery: Modern inhalational agents like sevoflurane or desflurane, or intravenous agents like propofol, allow for efficient anesthesia recovery, though often slower than regional techniques.
- Factors Unrelated to Evidence: Sometimes, patient anxiety, anticipated extended case duration, or the need for immediate postoperative neurologic examination can sway the decision towards general anesthesia.
The Power of Regional Anesthesia
Regional anesthesia, particularly peripheral nerve blocks, has revolutionized upper extremity surgery. The benefits are substantial, both for the patient and for our surgical efficiency.
- Enhanced Analgesia: Regional blocks provide superior analgesia, significantly reducing postoperative pain and opioid requirements.
- Reduced Side Effects: We see a lower incidence of postoperative nausea and vomiting (PONV), urinary retention, pruritus, and ileus compared to opioid-heavy general anesthesia.
- Faster Recovery and Discharge: Patients often experience shorter wake-up times, faster recovery from anesthesia, and earlier discharge from the hospital.
- Increased OR Efficiency: Nerve blocks can often be performed in a pre-operative holding area, eliminating the time needed for induction and emergence from general anesthesia in the OR itself.
- Simplified Perioperative Management: For patients with significant comorbidities like malignant hyperthermia, cardiomyopathy, or obstructive/restrictive lung conditions, regional anesthesia can simplify perioperative management by avoiding the systemic effects of general anesthetics.
- Improved Patient Satisfaction: The combination of superior pain control and fewer side effects directly translates to increased patient satisfaction.
- Decreased Postoperative Cognitive Dysfunction (POCD): By providing superior pain control, reducing sleep disturbances, and leading to fewer unplanned hospital admissions, regional anesthesia significantly lowers the incidence of POCD. Studies show a reduction from 9.8% to 3.5%.
- Specific Advantages for Trauma:
- Increased blood flow in the anesthetized area, potentially aiding tissue perfusion.
- Decreased blood loss intraoperatively.
- Avoidance of difficult endotracheal intubation, particularly relevant in trauma patients with potential airway compromise.
- Decreased phantom limb pain following amputation by preventing pain centralization.
- Continuous Regional Analgesia: This is a game-changer. Using an indwelling nerve catheter and a local anesthetic pump, we can maintain analgesia until the acute pain state dissipates.
- Outpatient Pumps: Elastomeric pumps have been developed for outpatient infusions, offering a compact, simple-to-operate, and safe method for continuous local anesthetic delivery in the home environment. This eliminates the frustration of single-shot blocks dissipating mid-night and the return of severe pain.
- Enhanced Rehabilitation: Continuous peripheral nerve catheters have been associated with enhanced physical rehabilitation after shoulder surgery due to superior pain control, facilitating early mobilization.
Contraindications to Regional Anesthesia
While highly beneficial, regional anesthesia is not without its contraindications.
- Absolute Contraindications:
- Patient Refusal: Always respect patient autonomy.
- Infection at the Puncture Site: Risk of spreading infection.
- Bleeding Disorders: Full anticoagulation, thrombolytic therapy, or hemophilia significantly increase the risk of hematoma, especially around nerves.
- Acute or Resolving Nerve Injury: Administering a block in the distribution of an acutely injured nerve can mask worsening deficits and impede accurate neurological assessment.
- Progressive Peripheral Neuropathy: Similar to acute nerve injury, it can complicate assessment and potentially exacerbate the condition.
- Relative Contraindications:
- Stable Nerve Impairment: Requires careful consideration and discussion.
- Severe Chronic Obstructive Pulmonary Disease (COPD): Interscalene blocks can cause ipsilateral phrenic nerve paralysis, which might be poorly tolerated in patients with severe respiratory compromise.
- Fever, Bacteremia: Increased risk of infection.
- Multiple Sclerosis: Spinal anesthesia is contraindicated.
- Stroke, Diabetes Mellitus: These conditions require careful assessment of baseline neurological status and potential for nerve susceptibility.
Propofol with Regional Blocks: The Sedation Spectrum
Propofol may be administered with regional blocks to provide light or heavy sedation, allowing the patient to remain comfortable and still, while avoiding the deeper physiological impact of general anesthesia.
Regional Anesthesia for Upper Extremity Surgery: A Deep Dive
Let's walk through the specific regional techniques we utilize for different upper extremity procedures.
Shoulder Surgery: The Interscalene Block
Shoulder surgery, particularly arthroplasty or open rotator cuff repairs, is notoriously painful. General anesthesia alone is rarely sufficient for adequate perioperative pain control.
- Anatomical Basis: The shoulder is primarily innervated by the brachial plexus, with minor sensory contributions from the superficial cervical plexus.
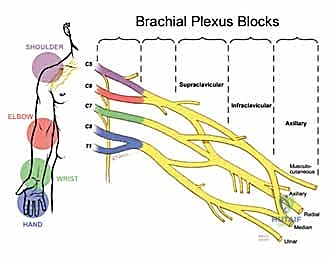


FIG 2 • Brachial plexus blocks.
* The Interscalene Block: This is our workhorse for shoulder procedures. It targets the brachial plexus at the level of the trunks, effectively blocking the superior and middle trunks, along with the superficial cervical plexus.
* Localization: The anesthesiologist identifies the superficial landmarks and needle puncture site by palpating the interscalene groove—the space created by the anterior and middle scalene muscles—at the level of the cricoid cartilage.



FIG 3 • Interscalene block. (A) Identification of superficial landmarks and needle puncture site by palpating the space created by the trunks between the anterior and middle scalene muscles at the level of the cricoid cartilage. (B) The nerves can be localized using paresthesia, nerve stimulator, or ultrasound. (By permission of Mayo Foundation for Medical Education and Research. All rights reserved.)
* Execution (Anesthesiologist's View): Once the needle is in close approximation to the brachial plexus trunks (confirmed by paresthesia, nerve stimulator, or ultrasound guidance), a local anesthetic (typically bupivacaine or ropivacaine) is incrementally injected. This provides excellent anesthesia of the shoulder and proximal arm.
* Surgical Benefit: Interscalene blocks cause a sympathectomy in the anesthetized area, leading to redistribution of blood away from the surgical site. This often translates to decreased intraoperative blood loss and improved visualization for us.
* Adjunctive Analgesia: Occasionally, incisions or arthroscopic port holes may fall slightly outside the primary block distribution. In these instances, we, the surgical team, can inject local anesthetic directly into the affected area to supplement the block. Intra-articular local anesthetic and narcotic infusions can also be helpful, but they must be combined with an interscalene block for maximum postoperative analgesia.
* Continuous Interscalene Blocks: For prolonged analgesia, especially in acute surgical shoulder pain, chronic pain patients, or those requiring aggressive mobilization therapy for frozen shoulder, a continuous interscalene block with an indwelling catheter is invaluable. These have been shown to enhance physical rehabilitation due to superior pain control.
Patient Positioning for Shoulder Surgery
The semisitting (beach chair) position is frequently selected for shoulder surgery. This position requires specific attention to patient safety.
- Head and Neck Positioning: The OR table must be equipped with a specialized headpiece securing the patient's head with a padded strap at the forehead. Head and neck positioning is crucial to avoid spinal cord compression and potential neurologic deficits. This can be challenging for the anesthesiologist, as the proximity of the surgical field limits access to the head.
- Air Embolism Risk: Both the semisitting and lateral decubitus positions place the operative site above the heart, which, though rare, can increase the risk of air embolism if venous sinuses are opened. Our anesthesiologists are vigilant for this complication.
Pearls and Pitfalls of Interscalene Blocks
- Side Effects: Interscalene blocks are associated with specific side effects due to the proximity of other nerves:
- Phrenic Nerve Blockade: This results in transient loss of ipsilateral diaphragm function. While generally well-tolerated in healthy individuals, it can be a significant concern for patients with severe COPD.
- Recurrent Laryngeal Nerve Blockade: Can cause a weak, hoarse voice.
- Stellate Ganglion Blockade: Leads to Horner's syndrome (miosis, ptosis, anhydrosis on the ipsilateral side). These are typically transient and resolve with the block.
- Compartment Syndrome Masking:
> SURGICAL WARNING: Nerve blocks with concentrated local anesthetics (bupivacaine or ropivacaine 0.5% or higher) can mask the symptoms of compartment syndrome. This is a critical pitfall. We must avoid these high-concentration blocks in patients at risk for compartment syndrome (e.g., high-energy trauma, revascularization procedures, prolonged tourniquet times). Close communication with anesthesia and vigilant clinical monitoring are paramount. - Conversion to General Anesthesia Mid-Procedure:
> SURGICAL WARNING: If a patient with a regional anesthetic needs to be converted to general anesthesia in the middle of a procedure, it can be extremely difficult without disrupting the sterile surgical field. While general anesthesia can sometimes be administered via mask ventilation or laryngeal mask airway (LMA) in the semisitting position (offering some airway control but no aspiration protection), it often necessitates taking down the drapes and repositioning the patient supine for endotracheal intubation. This significantly prolongs OR time and increases the risk of contamination. Therefore, for complicated reoperations or cases requiring induced hypotension, a combined general anesthesia with an endotracheal tube and an interscalene block is often preferred by both surgeons and anesthesiologists.
Elbow Surgery: Facilitating Early Rehabilitation
Surgical procedures at the elbow, from arthroplasty to biceps tendon reattachment, also benefit greatly from regional anesthesia, though general anesthesia is frequently employed due to the complexity and duration of some cases.
- Early Rehabilitation: Functional outcomes after elbow surgery often depend on early rehabilitation, frequently utilizing continuous passive motion (CPM) devices. This therapy is greatly facilitated by continuous brachial plexus analgesia.
- Brachial Plexus Approaches: For elbow surgery, the infraclavicular and axillary approaches to the brachial plexus are excellent options for continuous catheter placement.
- Infraclavicular Block: This block targets the cords of the brachial plexus. The needle is typically placed about 1 inch distal to the midclavicle and advanced toward the axillary pulsation until a twitch or paresthesia is obtained (now more commonly ultrasound-guided).

- Infraclavicular Block: This block targets the cords of the brachial plexus. The needle is typically placed about 1 inch distal to the midclavicle and advanced toward the axillary pulsation until a twitch or paresthesia is obtained (now more commonly ultrasound-guided).


FIG 4 • Infraclavicular block. (By permission of Mayo Foundation for Medical Education and Research. All rights reserved.)
* Axillary Block: This approach targets the terminal nerves (median, ulnar, radial, musculocutaneous) in the axilla. It's often easier to perform and provides excellent distal arm and hand anesthesia.



FIG 5 • Axillary brachial plexus block. (By permission of Mayo Foundation for Medical Education and Research. All rights reserved.)
* Postoperative Neurologic Assessment: A key concern for us, the surgeons, is the proximity of nerves to the surgical incision in elbow procedures. If we anticipate needing to examine neurologic function in the immediate postoperative period (e.g., after ulnar nerve transposition or complex fracture fixation), a nerve block might obscure this assessment. In such cases, regional techniques may be performed after initial nerve function assessment in the recovery area, or a lower concentration block might be chosen.
* Duration of Analgesia: Typically, 48 hours of postoperative pain control is adequate for most elbow procedures, after which catheters are removed.
Forearm and Hand Surgery: Precision and Specificity
For forearm and hand surgery, our anesthetic options are tailored to the specific anatomical distribution and duration of the procedure.
- Infraclavicular Block: As discussed, this provides excellent coverage for the forearm and hand.
- Axillary Block: Highly effective for procedures distal to the elbow, blocking the median, ulnar, and radial nerves.
- Intravenous Regional Anesthesia (Bier Block): For short procedures (typically less than 1 hour) on the hand or forearm, an IV regional block is a rapid and effective option. This involves exsanguinating the limb and injecting local anesthetic (e.g., lidocaine) into an intravenous catheter distal to a tourniquet. It provides excellent anesthesia but has a limited duration due to tourniquet tolerance.
Nerve Blocks for Upper Extremity Surgery
| Procedure | Block |
|---|---|
| Shoulder surgery | Interscalene |
| Elbow surgery | Interscalene, supraclavicular, or infraclavicular |
| Forearm and hand surgery | Infraclavicular, axillary or IV regional (short procedures < 1 hour) |
Postoperative Rehabilitation and Complication Management
Our commitment to the patient extends well beyond wound closure. The anesthetic choices we make have a direct impact on the postoperative course.
Pain Management and Rehabilitation
- Continuous Regional Analgesia: This is a cornerstone of modern orthopaedic pain management. By providing sustained analgesia, it allows for earlier and more aggressive physical rehabilitation, leading to improved functional outcomes. Patients can participate in therapy without being limited by severe pain.
- Opioid Sparing: Regional techniques decrease the reliance on systemic opioids, thereby reducing their associated side effects (nausea, constipation, sedation, respiratory depression). This is a significant advantage for patient comfort and recovery.
- DVT Prophylaxis: While not directly related to peripheral nerve blocks, it's worth noting that neuraxial blocks (spinal, epidural) are associated with a lower incidence of deep venous thrombosis. For upper extremity surgery, our DVT prophylaxis typically involves early mobilization and, for higher-risk patients, pharmacological agents.
Managing Anesthetic Complications
- Local Anesthetic Toxicity: This is a rare but serious complication, especially with large volumes or high concentrations. Symptoms can range from CNS effects (tinnitus, perioral numbness, seizures) to cardiovascular collapse. Our anesthesiologists are trained to recognize and manage this immediately.
- Nerve Injury: While rare, direct needle trauma, intraneural injection, or hematoma formation can cause nerve injury. Ultrasound guidance has significantly reduced this risk. Meticulous technique and vigilance are key.
- Block Dissipation and Return of Pain: This is the primary frustration with single-shot blocks. Continuous catheters address this by providing sustained analgesia until the acute pain phase resolves, often 24-48 hours.
Surgical Warnings for the Orthopaedic Surgeon
- Communication is Key: Always maintain open and clear communication with your anesthesiology team. Discuss the anticipated surgical duration, potential for significant blood loss, the need for
REFERENCES
-
Auroy Y, Benhamou D, Barques L, et al. Major complications of regional anesthesia in France. Anesthesiology 2002;97:1274–1280.
-
Benumof JL. Permanent loss of cervical spinal cord function associated with interscalene block performed under general anesthesia. Anesthesiology 2000;93:1541–1544.
-
Canet J, Raeder J, Rasmussen LS, et al. Cognitive dysfunction after minor surgery in the elderly. Acta Anaesth Scand 2003;47:1204–1210.
-
Capdevila X, Pirat P, Bringuier S, et al. Continuous peripheral nerve blocks in hospital wards after orthopedic surgery: a multicenter prospective analysis of the quality of postoperative analgesia and complications in 1,416 patients. Anesthesiology 2005;103:1035–1045.
-
Chung F, Ritchie E, Su J. Postoperative pain in ambulatory surgery. Anesth Analg 1997;85:808–816.
-
Cohen NP, Levine WN, Marra G, et al. Indwelling interscalene catheter anesthesia in the surgical management of stiff shoulder: a
You Might Also Like


