Principles of Arthroscopic Anesthesia, Documentation, and Surgical Advantages

Key Takeaway
Arthroscopic surgery requires meticulous anesthetic planning, balancing patient comfort with optimal surgical visualization. While general anesthesia is preferred for complex procedures involving significant hemostasis, local anesthesia with a lidocaine-bupivacaine mixture offers an effective alternative for select cases. Multimodal pain management, including pre-emptive NSAIDs and intraarticular analgesics, significantly enhances postoperative recovery. Furthermore, arthroscopy provides superior diagnostic accuracy, reduced inflammatory response, and access to intraarticular structures inaccessible via traditional open arthrotomy.
INTRODUCTION TO ARTHROSCOPIC PERIOPERATIVE MANAGEMENT
The evolution of arthroscopic surgery represents one of the most profound paradigm shifts in the history of orthopaedics. Transitioning from extensile open arthrotomies to minimally invasive, endoscopically driven techniques has fundamentally altered the landscape of joint surgery. However, the success of an arthroscopic procedure is not solely dependent on the surgeon’s technical dexterity with a camera and motorized instruments; it relies heavily on meticulous perioperative management. This encompasses the strategic selection of anesthesia, rigorous multimodal pain management protocols, high-fidelity intraoperative documentation, and a comprehensive understanding of the physiological advantages conferred by the arthroscopic approach.
For the orthopaedic resident, fellow, and practicing consultant, mastering these perioperative principles is as critical as mastering the surgical techniques themselves. Proper anesthetic choice dictates the quality of the visual field, while robust documentation protects the surgeon medicolegally and facilitates longitudinal patient care.
ANESTHESIA IN ARTHROSCOPIC SURGERY
The selection of anesthesia for arthroscopy must be tailored to the anticipated complexity of the procedure, the expected duration of surgery, the patient's medical comorbidities, and the requirement for intraoperative hemostasis. The primary modalities include general anesthesia, regional anesthesia (neuraxial or peripheral nerve blocks), and local anesthesia.
General Anesthesia and Hemodynamic Control
When significant intraarticular bleeding is anticipated—such as during partial or complete synovectomies, extensive lysis of adhesions, or complex reconstructive procedures (e.g., anterior cruciate ligament reconstruction or rotator cuff repair)—general anesthesia remains the recommended standard of care.
General anesthesia provides several distinct advantages:
* Absolute Patient Immobility: Essential for delicate work near neurovascular structures.
* Controlled Hypotension: The anesthesiologist can manipulate systemic blood pressure to reduce capillary bleeding, thereby optimizing the arthroscopic visual field.
* Airway Security: Particularly critical in shoulder arthroscopy performed in the beach-chair or lateral decubitus positions, where airway access is restricted once the patient is draped.
Most advanced arthroscopic procedures performed in modern tertiary clinics are executed under general anesthesia, often supplemented by regional nerve blocks to preemptively manage postoperative pain.
Local Anesthesia Protocols
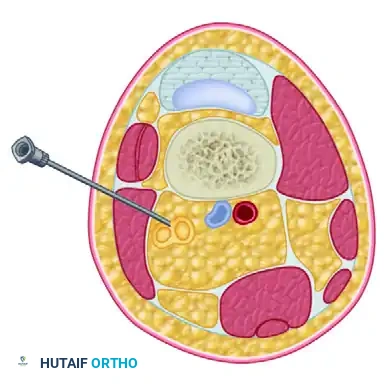
For diagnostic arthroscopies or minor therapeutic interventions (e.g., simple meniscectomy or removal of loose bodies), local anesthesia presents a viable, highly efficient alternative. When local anesthesia is selected, the pneumatic tourniquet is typically not inflated, as the ischemic pain generated by the tourniquet will rapidly exceed the patient's tolerance, negating the benefits of the local technique.
A highly effective and historically validated protocol for local anesthesia in knee arthroscopy was detailed by Yoshiya et al. The protocol utilizes a synergistic mixture of short-acting and long-acting amide local anesthetics:
* The Mixture: A 1:1 ratio of 1% lidocaine (providing rapid onset) and 0.25% bupivacaine (providing prolonged duration of action).
* Intraarticular Injection: Typically, 50 mL of this mixture is injected directly into the joint capsule prior to the initiation of the procedure. This distends the capsule and provides widespread synovial anesthesia.
* Portal Infiltration: At each anticipated arthroscopic portal site, an additional 5 mL of the mixture is injected. The surgeon must meticulously infiltrate the skin, subcutaneous tissue, and the underlying capsule to ensure a painless tract for the trocars.
Surgical Warning: Local Anesthetic Systemic Toxicity (LAST)
When utilizing high volumes of local anesthetics, the surgeon must remain acutely aware of toxic thresholds. Bupivacaine is highly cardiotoxic. The maximum safe dosage of bupivacaine must not exceed 2 mg/kg of body weight (or 2.5 mg/kg when combined with epinephrine). Careful calculation of the total administered volume (intraarticular + portal sites) is mandatory to prevent central nervous system (CNS) or cardiovascular complications.
When a longer procedure is anticipated under local anesthesia, a small amount of epinephrine (typically 1:100,000 or 1:200,000) can be added to the anesthetic mixture. Epinephrine induces local vasoconstriction, which serves a dual purpose: it helps maintain intraoperative hemostasis for better visualization and decreases the systemic absorption rate of the anesthetic agents, thereby prolonging their duration of action and increasing the margin of safety against systemic toxicity.
Clinical outcomes using this local anesthetic protocol have been exceptionally favorable. Literature reports indicate an extremely low complication rate, with isolated incidences of mild nausea and virtually no reports of toxic reactions, CNS disturbances, or cardiovascular events when dosing limits are strictly respected.
PERIOPERATIVE AND POSTOPERATIVE PAIN MANAGEMENT
The mitigation of postoperative pain begins in the preoperative holding area. A preemptive, multimodal approach to analgesia is the gold standard in modern operative orthopaedics, aiming to block pain pathways at multiple levels of the nervous system while minimizing opioid consumption.
The Role of Anti-inflammatory Medications
Postoperative pain and joint stiffness are largely driven by the inflammatory cascade initiated by surgical trauma.
* Nonsteroidal Anti-inflammatory Drugs (NSAIDs): The administration of oral NSAIDs both preoperatively and postoperatively, or via intramuscular/intravenous routes intraoperatively (e.g., IV ketorolac), has been shown to significantly diminish postoperative pain. By inhibiting cyclooxygenase (COX) enzymes and reducing prostaglandin synthesis, NSAIDs effectively reduce postoperative joint swelling and facilitate an earlier, more comfortable return to range of motion (ROM).
* Corticosteroids: In contrast to NSAIDs, the routine use of oral corticosteroids has not proven effective for routine postoperative pain management in arthroscopy and is generally avoided due to the potential risks of immunosuppression and delayed wound healing.
Intraarticular Analgesia and Pain Pumps
Direct intraarticular administration of analgesics at the conclusion of the procedure provides excellent targeted pain relief. Beneficial analgesic effects have been well-documented following the intraarticular injection of 30 mL of 0.25% bupivacaine. The addition of 3 mg of preservative-free morphine to this mixture can further enhance analgesia by binding to peripheral opioid receptors that are upregulated in inflamed synovial tissues.
Historically, the use of continuous-flow subacromial or intraarticular pain pumps was popularized to provide sustained postoperative pain relief, particularly for arthroscopic shoulder procedures where they demonstrated excellent efficacy. These elastomeric pumps deliver a continuous basal rate of local anesthetic directly to the surgical site. Conversely, they have shown less dramatic benefit in knee arthroscopy cases.
Critical Clinical Pitfall: Postarthroscopic Glenohumeral Chondrolysis (PAGCL)
While the historical text notes the excellent pain relief provided by intraarticular pain pumps in the shoulder, modern orthopaedic evidence mandates a severe warning. The continuous intraarticular infusion of high-volume bupivacaine (especially with epinephrine) has been definitively linked to Postarthroscopic Glenohumeral Chondrolysis—a devastating, irreversible destruction of the articular cartilage. Intraarticular placement of continuous bupivacaine pain pumps in the shoulder is now strictly contraindicated. If a pain pump is utilized, the catheter must be placed strictly in the subacromial space or utilized as a peripheral nerve block (e.g., interscalene catheter), meticulously cared for, and removed within 48 hours.
ARTHROSCOPIC DOCUMENTATION AND IMAGING
Accurate, high-resolution documentation of arthroscopic findings and surgical interventions is a fundamental medicolegal and clinical requirement. The arthroscopic image serves as the objective record of the joint's internal pathology, often superseding preoperative imaging modalities like MRI in definitive diagnostic accuracy.
Technological Infrastructure
The modern arthroscopic suite is equipped with a sophisticated imaging tower, as demonstrated in the documentation setup. The standard configuration includes a high-definition monitor, a camera control unit (CCU), a high-intensity light source (xenon or LED), a fluid management system, and a digital image capture device.
Digitalized pictures are routinely taken, catalogued, and stored on secure hospital servers or compact discs for later retrieval, patient education, and academic slide production.
Image Capture Specifications
To ensure clinical and academic utility, the imaging equipment must meet specific technical thresholds:
* Resolution: Any digital camera system utilized should possess a minimum of three megapixels of resolution and a macro function to capture the fine details of articular cartilage and synovial vascularity.
* Print Quality: If images are captured at high resolution (300 dpi or higher), they are deemed suitable for high-quality reproduction in printed materials, such as peer-reviewed journal articles or orthopaedic textbooks.
* Integration: Modern systems utilize an image capture unit that interfaces directly with the back of the arthroscopy camera. Activation is seamlessly controlled by a programmable button on the sterile camera head. When depressed, the screen image is instantly captured to a computer file.
* Video Documentation: In addition to static images, short video segments detailing dynamic pathology (e.g., demonstrating a positive arthroscopic drive-through sign or the reduction of a meniscus tear) can be similarly captured and stored, providing invaluable dynamic records of the joint's biomechanics.
FUNDAMENTAL ADVANTAGES OF ARTHROSCOPIC SURGERY
The universal adoption of arthroscopy over traditional open arthrotomy is justified by a multitude of physiological, diagnostic, and economic advantages. Understanding these benefits is crucial for appropriate surgical decision-making and patient counseling.
1. Less Intense Inflammatory Response
The physiological insult of an open arthrotomy is substantial. Large incisions through the joint capsule and synovium trigger a massive release of inflammatory cytokines. In contrast, arthroscopy utilizes micro-incisions (portals). This minimal disruption of the capsule and synovium results in a drastically reduced inflammatory response. Clinically, this translates directly to less postoperative pain, a marked reduction in arthrofibrosis, faster rehabilitation milestones, and an accelerated return to work and athletic participation.
2. Improved Thoroughness of Diagnosis
Arthroscopy remains the ultimate gold standard for intraarticular diagnosis. Most investigators report that diagnoses based purely on clinical examination or non-invasive imaging are incomplete in a significant percentage of patients.
* Shoulder Pathology: Malhi and Khan reviewed 130 consecutive shoulder arthroscopies, comparing operative findings with preoperative clinical assessments. They found that while clinical diagnoses of impingement and instability strongly correlated with arthroscopic findings, the clinical diagnosis of frozen shoulder and rotator cuff tears had a much weaker correlation. Strikingly, out of nine patients who had completely normal clinical examinations, all nine demonstrated distinct abnormalities during arthroscopic evaluation.
* Knee Pathology: Brooks and Morgan evaluated the diagnostic accuracy in the knee, reporting that both clinical diagnosis and MRI diagnosis had only a 79% agreement with the definitive arthroscopic diagnosis. In a series of 240 knee arthroscopies, only 10 knees (4%) were found to be truly normal, highlighting the superior sensitivity of direct endoscopic visualization.
3. Absence of Secondary Effects
Open arthrotomies around joints are fraught with secondary morbidities. Arthroscopic techniques effectively eliminate these risks, which include:
* Neuroma Formation: Open knee incisions frequently transect the infrapatellar branch of the saphenous nerve, leading to painful neuromas. Portal placement avoids major cutaneous nerve branches.
* Cosmesis: Painful, disfiguring, and hypertrophic scars are avoided.
* Functional Imbalance: Open approaches often require splitting or detaching muscles (e.g., the vastus medialis obliquus in the knee or the subscapularis in the shoulder), leading to potential functional imbalance of the extensor mechanism or rotator cuff. Arthroscopy is entirely muscle-sparing.
4. Reduced Hospital Cost and Outpatient Transition
The minimal morbidity of arthroscopy has driven a massive shift in health economics. The vast majority of arthroscopic procedures—including complex ligament reconstructions and rotator cuff repairs—are now performed safely on an outpatient basis in Ambulatory Surgery Centers (ASCs). If hospitalization is required due to patient comorbidities, a 1- or 2-day stay is generally the absolute maximum, compared with the several days of inpatient pain management and physical therapy historically required for open arthrotomy procedures.
5. Reduced Complication Rate
When performed by a trained orthopaedic surgeon, arthroscopy carries an exceptionally low complication rate. Deep joint infections, severe venous thromboembolism (VTE), and neurovascular injuries are statistically infrequent compared to open joint surgery, provided meticulous technique and appropriate prophylactic measures are employed.
6. Improved Follow-up Evaluation ("Second-Look" Procedures)
Because the morbidity associated with arthroscopy is so minimal, it allows surgeons to safely re-enter the joint to evaluate the healing of a previous operative procedure. These "relook" or "second-look" procedures are invaluable for assessing the integration of a meniscal repair, the maturation of an autologous chondrocyte implantation (ACI), or the stability of a reconstructed ligament if persistent symptoms warrant further direct evaluation.
7. Access to Difficult or Impossible Surgical Anatomies
Perhaps the most profound technical advantage of arthroscopy is the ability to perform surgical procedures that are exceptionally difficult, or anatomically impossible, to execute through an open arthrotomy without causing massive collateral tissue damage.
* Meniscal Access: Partial meniscectomy and meniscal repair are prime examples. Trimming, contouring, or suturing the inner posterior edge (posterior horn) of a meniscus via open means is extremely difficult due to the overhanging femoral condyles. Arthroscopy, utilizing 30-degree and 70-degree angled lenses, allows the surgeon to navigate around the condyles and visualize the posterior compartments with brilliant clarity. Many repairable meniscal tears are accessible only with arthroscopic techniques and simply cannot be satisfactorily viewed or instrumented through a standard arthrotomy.
You Might Also Like