Amputations of the Hand: Surgical Principles & Techniques
Key Takeaway
Hand and digit amputations require meticulous surgical planning to preserve maximum function, sensation, and length. This guide details evidence-based indications, biomechanical considerations, and step-by-step surgical techniques for primary amputations and complex reconstructions, including neurovascular island transfers for thumb salvage. Mastery of soft-tissue handling and joint preservation is essential for optimizing postoperative pinch and grasp mechanics.
Introduction to Hand Amputations
Surgical amputation through the fingers or metacarpals must never be viewed merely as a failure of salvage, but rather as a definitive reconstructive procedure designed to preserve maximum function in both the injured and uninjured parts of the hand. While acute traumatic incomplete and complete amputations may occasionally be salvaged by emergency microsurgical replantation, efforts to preserve severely damaged, non-viable, or insensate structures can delay healing, increase disability, and subject the patient to a prolonged, painful series of surgical interventions.
In many individuals, primary amputation is the procedure of choice. The overarching goals of any hand amputation are to maintain supple soft-tissue coverage, preserve functional digital length, retain critical joint mobility, and ensure durable skin sensation. In amputations involving several digits, the preservation of pinch and grasp remains the paramount functional objective.
Clinical Pearl: The ultimate function of the preserved part must be sufficient to warrant the time, surgical risk, and rehabilitative effort required of the patient. A stiff, painful, and insensate digit is functionally inferior to a well-constructed amputation stump.
Considerations and Indications for Amputation
Amputations are considered for a variety of conditions where hand function is severely limited by intractable pain, profound stiffness, insensibility, or severe cosmetic deformity. When a patient requests the amputation of a chronically injured, non-functional part, it is usually the culmination of a critical thought process and is frequently justified.
The Absolute Indication
The only absolute indication for a primary amputation is the irreversible loss of blood supply to the part that cannot be restored via microvascular techniques.
The "Rule of Three" for Tissue Assessment
When deciding whether to amputate or attempt complex salvage, an analysis of the five critical tissue areas is highly beneficial:
1. Skin (Coverage)
2. Tendon (Motor function)
3. Nerve (Sensation)
4. Bone (Structural stability)
5. Joint (Mobility)
Surgical Warning: If three or more of these five tissue areas require specialized reconstructive procedures (e.g., pedicled skin grafting, tendon grafting/transfer, nerve suturing/grafting, complex bony fixation, or joint arthrodesis/arthroplasty), primary amputation should be strongly considered. The survival of a mutilated, stiff finger frequently compromises the overall function of the remaining uninjured digits.
Pediatric Considerations
In children, the threshold for amputation is significantly higher. Amputation is rarely indicated unless the part is frankly nonviable and cannot be revascularized. Children possess extraordinary neuroplasticity and healing capabilities; therefore, even severely traumatized digits should be preserved if possible, as parts of the finger may serve as valuable donor tissue for later reconstructive procedures.
The "Spare Parts" Concept in Hand Trauma
When amputation is inevitable, the surgeon must adopt a "spare parts" mentality. Tissues from an otherwise useless or nonviable digit can be harvested to reconstruct adjacent injuries:
* Skin: Can be utilized as a full-thickness free graft.
* Filleted Grafts: Skin and deeper soft structures can be elevated as a filleted flap. The bone is removed primarily, and the remaining vascularized flap is fashioned to cover adjacent defects.
* Island Flaps: Skin well-supported by one or more neurovascular bundles (but lacking osseous support) can be salvaged as a vascular or neurovascular island graft.
* Nerves: Segments of healthy nerve from the amputated part can serve as autogenous interpositional grafts for adjacent nerve gaps.
* Tendons: Musculotendinous units (e.g., flexor digitorum superficialis [FDS], extensor indicis proprius [EIP], or extensor digiti minimi [EDM]) can be preserved for tendon transfers. For example, an FDS can be transferred to restore adductor power to the thumb if the third metacarpal shaft is destroyed.
* Bone: Discarded phalanges or metacarpals can be utilized as autologous peg grafts or to fill osseous defects in surviving digits.
Principles of Fingertip Amputations
Amputations occurring between the tip of the finger and the lunula of the nail (Zone 1) usually cannot be salvaged by microvascular techniques due to the diminutive caliber of the distal vessels. These injuries typically require amputation completion and robust soft-tissue coverage.
The Palmar Pocket Technique
For distal tip amputations in fingers other than the thumb, the amputated tip can occasionally be reattached as a composite graft and buried in a surgically created pocket in the ipsilateral palm.
* Technique: The fingertip is deepithelialized and sutured to the stump. A subcutaneous pocket is elevated in the palm, and the digit is sutured into this pocket to allow revascularization from the palmar bed.
* Timeline: The finger is surgically removed from the palmar pocket 16 to 20 days postoperatively.
* Outcomes: Studies (such as those by Arata et al.) have demonstrated highly successful salvage rates using this method, preserving critical length and contour.
Pediatric Fingertip Injuries
In pediatric patients, the simple resuturing of a defatted, amputated fingertip back into place as a composite graft frequently yields a highly satisfactory result. The robust angiogenic potential in children allows the graft to survive as a composite tissue transfer, provided the graft is meticulously defatted to reduce metabolic demand during the initial avascular phase.
Amputations of Single Fingers
The biomechanical role of each digit dictates the surgical approach to its amputation.
Index Finger Amputations
The index finger is the primary digit for precision pinch with the thumb. However, if amputated proximal to the proximal interphalangeal (PIP) joint, the remaining stump is often excluded from use, and the patient will subconsciously bypass the index stump, utilizing the middle finger for pinch.
* Ray Amputation: For proximal index amputations, a primary ray amputation (removal of the digit and the second metacarpal shaft) is often preferred. This creates a smooth, aesthetically pleasing web space between the thumb and middle finger, deepening the first web space and enhancing thumb-to-middle finger pinch.
Middle and Ring Finger Amputations
Amputations of the central digits (middle or ring) present a unique functional challenge: the resulting gap allows small objects (like coins or keys) to fall through the hand during grasp.
* Ray Amputation with Transposition: To close this functional and cosmetic gap, a ray amputation is performed, followed by digital transposition. For a middle finger loss, the index ray is transposed to the third metacarpal base. For a ring finger loss, the small finger ray is transposed to the fourth metacarpal base. This restores a solid, continuous palmar grasp.
Little Finger Amputations
The little finger is critical for power grip. Preservation of the carpometacarpal (CMC) joint and the hypothenar musculature is essential. If the digit must be amputated, preserving the base of the fifth metacarpal maintains the insertion of the extensor carpi ulnaris (ECU) and the structural integrity of the ulnar border of the hand.
Amputations of Multiple Digits
In devastating crush injuries or multi-level amputations, the primary objective shifts to salvaging any functional length to preserve sensate pinch and power grasp.
* Phalangeal Preservation: Every millimeter of proximal phalanx must be saved.
* Web Space Deepening: Relative lengthening of the remaining stumps can be achieved through Z-plasties or dorsal transposition flaps to deepen the web spaces, effectively increasing the functional length of the amputated digits.
Reconstruction of the Thumb: A Case Study in Salvage
The thumb accounts for approximately 40% to 50% of total hand function. Every conceivable effort must be made to salvage the thumb. Even a short, stiff, but sensate thumb is vastly superior to a prosthesis. When primary replantation fails, complex reconstructive salvage is mandatory.
Consider the following clinical scenario of a severe saw injury resulting in a failed thumb replantation, concomitant primary ray amputation of the index finger, and partial amputation of the middle finger.
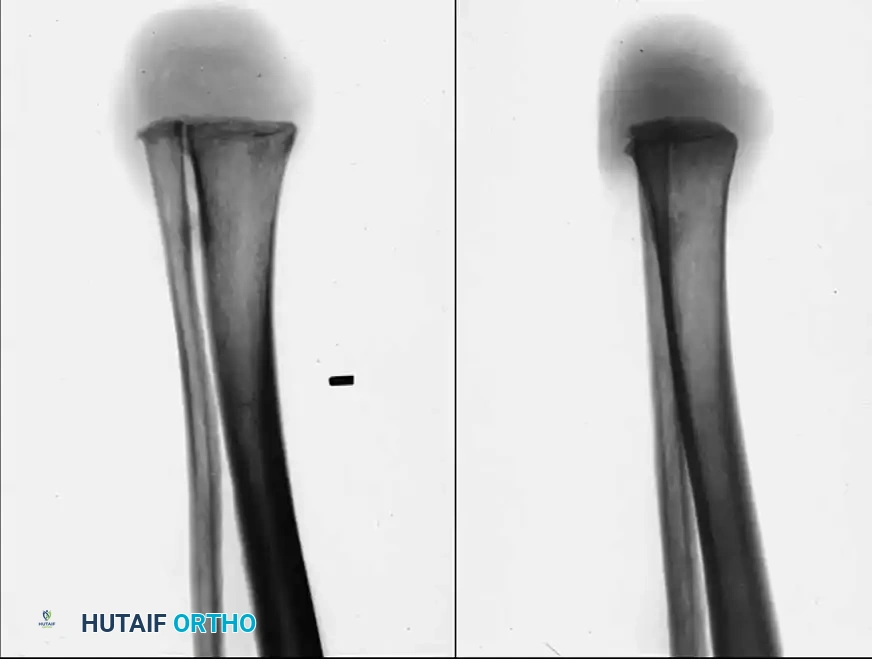
Figure 14-1A: Failed thumb replantation following a devastating saw injury. The replanted thumb has undergone complete ischemic necrosis, necessitating surgical debridement and complex reconstruction.
Step 1: Debridement and Preparation for Transfer
Following the demarcation of necrosis, the non-viable thumb is disarticulated at the metacarpophalangeal (MCP) joint level. To restore length and sensation, a neurovascular island transfer utilizing the proximal phalanx segment of the injured middle finger is planned.
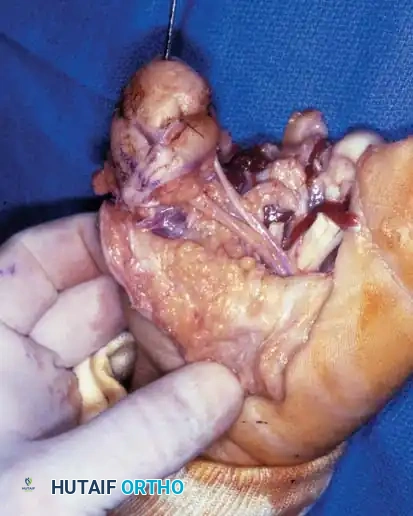
Figure 14-1B: Surgical dissection for the neurovascular island transfer. The necrotic tissue has been excised, and the recipient bed at the thumb MCP joint is prepared.
Step 2: Isolation of the Neurovascular Bundle
The success of an island transfer relies entirely on the meticulous dissection of the neurovascular pedicle. The digital artery and proper palmar digital nerve of the donor digit (middle finger stump) are carefully isolated into the palm.

Figure 14-1C: The neurovascular bundle is fully mobilized. The composite tissue from the middle finger is now tethered only by its vital vascular and neural supply, allowing it to be tunneled or transposed to the thumb position.
Step 3: Osseous Fixation and Soft Tissue Closure
The donor proximal phalanx is transposed to the thumb metacarpal. Rigid osseous fixation is achieved, typically utilizing longitudinal Kirschner wires (K-wires) or intraosseous wiring. The skin paddle is inset to provide durable, sensate coverage over the new thumb tip.
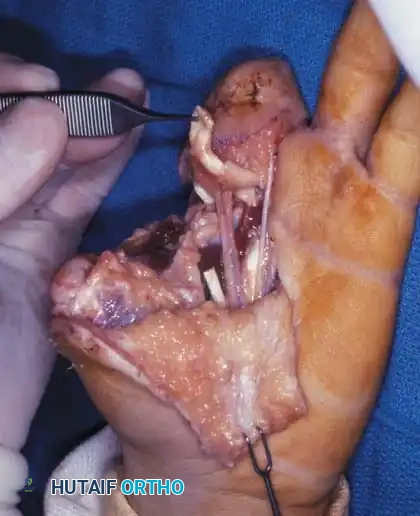
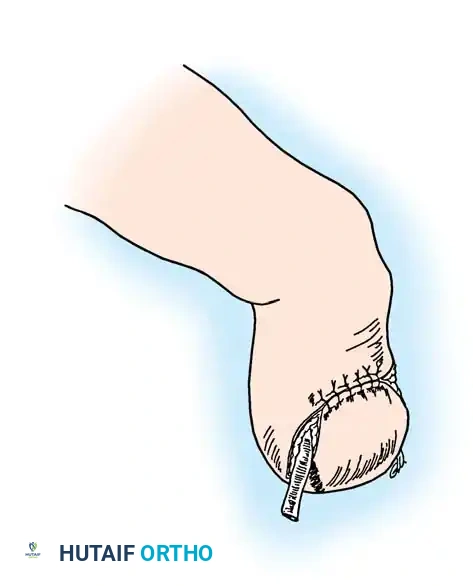
Figure 14-1D: Immediate postoperative appearance. The transferred middle finger segment is secured to the thumb metacarpal with a longitudinal K-wire (capped with a protective white sphere). The neurovascular island flap provides robust, sensate soft-tissue coverage.
Step 4: Radiographic Confirmation
Postoperative imaging is critical to ensure proper alignment and bony apposition between the transferred phalanx and the host metacarpal.

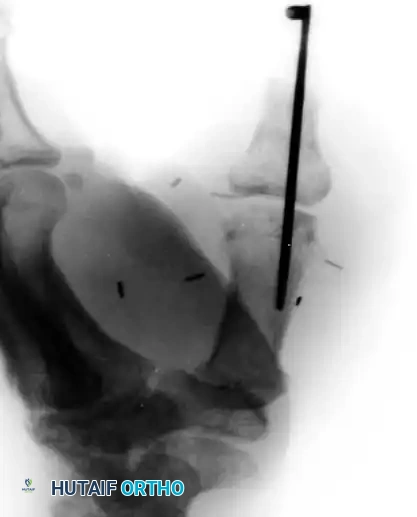
Figure 14-1E: Radiographic appearance demonstrating the transfer of the middle finger proximal phalanx to the thumb metacarpal, stabilized by a single longitudinal K-wire.
Step 5: Functional Rehabilitation
Following bony union (typically 6 to 8 weeks), the K-wire is removed, and aggressive occupational therapy commences. The ultimate goal is the restoration of power grasp and precision pinch. Because the transferred tissue retains its native nerve supply, cortical re-education is required for the patient to interpret sensory input from the new thumb correctly.

Figure 14-1F: Long-term functional outcome. The patient has successfully restored functional hand use, demonstrating the ability to perform power grip tasks, such as wielding a hammer, utilizing the sensory-innervated composite thumb reconstruction.
Management of the Painful Amputation Stump
A painful amputation stump is a devastating complication that severely limits hand function. The most common causes are inadequate soft-tissue coverage, adherent scars, and symptomatic neuromas.
Neuroma Management
Neuromas will inevitably form whenever a nerve is transected; the surgical goal is to ensure the neuroma forms in a protected, asymptomatic location.
* Traction Neurectomy: The nerve should be identified, placed under gentle distal traction, and transected sharply. It is then allowed to retract proximally into a healthy, well-cushioned soft-tissue bed, away from the incision line and areas of direct contact.
* Bone Implantation: In cases of recurrent symptomatic neuromas, the nerve end can be buried directly into the medullary canal of an adjacent bone.
Bone Contouring
The distal end of the amputated bone must be meticulously contoured. Prominent condyles at the phalangeal heads should be resected to prevent them from stretching the overlying skin, which can lead to ischemia, ulceration, and pain. If an amputation is performed through a joint (disarticulation), the articular cartilage should generally be removed, and the subchondral bone smoothed to promote adherence of the overlying soft-tissue flap.
Postoperative Protocols and Rehabilitation
Successful hand amputation surgery is only the first step; rigorous postoperative care is essential for optimal functional recovery.
- Immobilization: The hand is initially immobilized in a bulky, non-compressive dressing with a volar orthosis. The wrist is placed in 20-30 degrees of extension, MCP joints in 70-90 degrees of flexion, and PIP/DIP joints in full extension (the "intrinsic plus" or "safe" position) to prevent collateral ligament contracture.
- Elevation: Strict elevation above heart level is maintained for the first 48-72 hours to minimize edema, which can compromise flap perfusion and increase stiffness.
- Early Range of Motion (ROM): Active and passive ROM of all uninvolved digits and joints must begin immediately to prevent secondary stiffness.
- Desensitization: Once the wound is healed, a formal desensitization program (using varied textures, tapping, and fluidotherapy) is initiated to reduce stump hypersensitivity and facilitate early return to work and activities of daily living.
Clinical Pearl: The psychological impact of a hand amputation cannot be overstated. The surgeon must work closely with occupational therapists and psychologists to guide the patient through the process of cortical re-education, functional adaptation, and acceptance of their reconstructed hand.
You Might Also Like