Masterclass in Foot Amputations: Surgical Techniques and Biomechanics
Key Takeaway
Amputations of the foot and ankle are critical reconstructive procedures rather than treatment failures. Success depends on meticulous soft tissue handling, preoperative vascular assessment, and optimization of nutritional status. This guide details the biomechanical implications, indications, and step-by-step surgical techniques for toe amputations, ray resections, and metatarsophalangeal disarticulations, providing orthopedic surgeons with evidence-based protocols to maximize functional outcomes and limb salvage.
Introduction to Foot and Ankle Amputations
Amputations around the foot and ankle are becoming increasingly prevalent, driven largely by the rising global incidence of diabetic neuropathy and peripheral vascular disease. Historically viewed as a failure of medical management, ablation by amputation or disarticulation must instead be conceptualized as a definitive reconstructive procedure. The primary goal is to eradicate infection, remove ischemic or necrotic tissue, and create a stable, durable, and biomechanically sound residual limb that maximizes the patient's functional independence.
With advances in vascular perfusion assessment, orthotic design, and modern footwear modifications, the success rates of partial foot amputations have improved significantly. However, patients requiring distal amputations frequently present with complex, multi-systemic medical comorbidities. Consequently, the orthopedic surgeon must exercise exceptional judgment regarding the level of amputation, soft tissue handling, and postoperative wound management.
Clinical Pearl: Avoidance of excessive pressure on the skin edges is paramount. Never use toothed forceps (e.g., Adson forceps) on the skin edges of a dysvascular patient. Utilize skin hooks or stay sutures, employ thick fasciocutaneous flaps, refrain from tourniquet use when possible, and ensure meticulous hemostasis to prevent hematoma formation and subsequent flap necrosis.
Preoperative Assessment and Patient Optimization
The decision to proceed with a specific level of amputation relies heavily on predicting the healing potential of the residual soft tissue envelope.
Vascular Assessment
Clinical examination (palpable pulses, capillary refill, dependent rubor) is essential but insufficient in isolation. Objective non-invasive vascular testing is mandatory:
* Ankle-Brachial Index (ABI): While an ABI > 0.45 generally suggests adequate perfusion for healing, diabetic patients frequently exhibit medial arterial calcinosis (Mönckeberg's sclerosis), resulting in falsely elevated and incompressible vessels.
* Toe Pressures: A toe pressure greater than 45 mm Hg strongly correlates with successful wound healing.
* Transcutaneous Oximetry (tcPO2): A tcPO2 > 30 mm Hg indicates a high probability of healing. Conversely, a tcPO2 < 20 mm Hg indicates severe ischemia, making healing at that specific level highly unlikely and necessitating a more proximal amputation or preoperative vascular bypass/endovascular intervention.
Nutritional Optimization
The nutritional status of the patient is a critical, yet frequently overlooked, determinant of wound healing. According to landmark studies by Dickhaut et al., specific serologic markers are highly predictive of amputation success:
* Serum Albumin: Levels < 3.5 g/dL correlate with poor healing.
* Total Lymphocyte Count (TLC): A TLC < 1500/µL indicates malnutrition and immunocompromise, drastically increasing failure rates.
* Optimization: A healing rate of 82% can be achieved when TLC > 1500/µL and Albumin ≥ 3.5 g/dL. Patients falling below these thresholds require aggressive dietary supplementation or enteral feeding prior to elective amputation. If the clinical scenario (e.g., ascending gas gangrene, wet gangrene with sepsis) precludes delay, a higher-level amputation (e.g., Transtibial) may be required to ensure primary healing.
Biomechanics of Partial Foot Amputations
Understanding the biomechanical consequences of foot amputations is essential for predicting postoperative gait alterations and planning appropriate orthotic interventions.
Toe Amputations
Amputation of a single lesser toe generally causes minimal disturbance to stance or normal-paced gait.
* Great Toe (Hallux): Amputation of the hallux does not severely impair standing or slow walking. However, because the hallux provides the primary fulcrum for the windlass mechanism and terminal push-off, rapid walking or running will result in a noticeable limp.
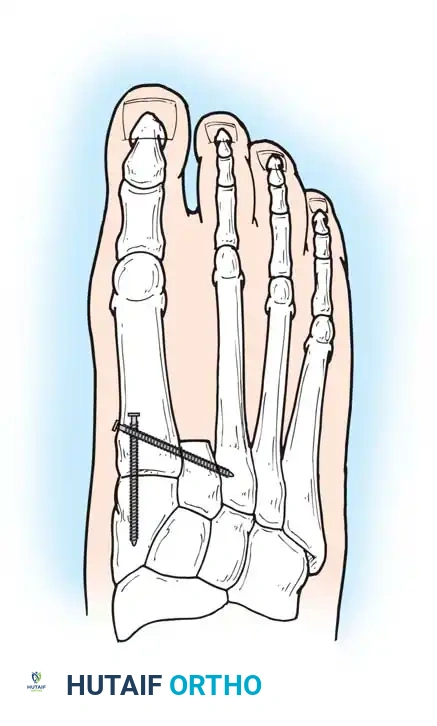
* Second Toe: Amputation of the second toe frequently results in severe hallux valgus. The great toe naturally drifts laterally into the void left by the resected second ray.
* Fifth Toe: The fifth toe is the most commonly amputated digit, usually indicated for a painful, overriding deformity where reconstructive procedures are deemed less reliable than definitive ablation.


Surgical Warning: To prevent severe hallux valgus following a second ray amputation, Smith recommended a complete second ray resection combined with surgical narrowing of the foot using transverse screw fixation between the first and third metatarsals.
Amputation of all toes eliminates the spring and resilience of the foot, interfering significantly with squatting, tiptoeing, and rapid gait. However, it requires no complex prosthesis other than a custom shoe filler.
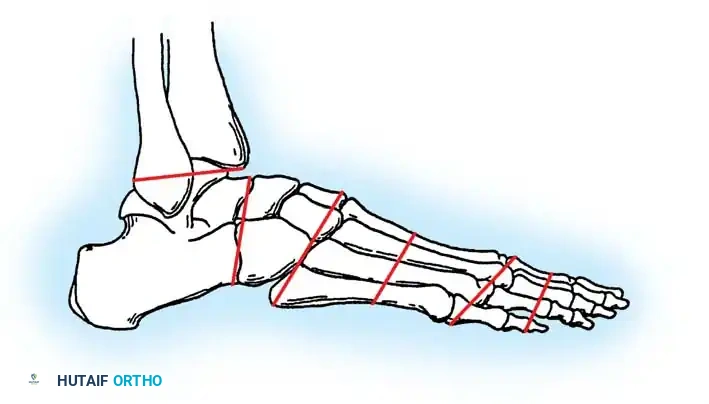
Transmetatarsal and Midfoot Amputations
Amputations proximal to the metatarsal heads become increasingly disabling. The loss of the anterior lever arm and the positive fulcrum in the ball of the foot severely impairs push-off.
Midfoot amputations (Lisfranc and Chopart levels) historically carried high failure rates due to severe biomechanical imbalances. Severing the insertions of the dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus) leaves the powerful plantarflexors (triceps surae) unopposed. This inevitably leads to a severe equinus deformity, resulting in distal stump breakdown and ulceration.

To prevent this, simultaneous percutaneous Tendo-Achilles Lengthening (TAL) or formal heel cord tenotomy is mandatory during midfoot amputations. Roach and McFarlane demonstrated that prophylactic heel cord tenotomies prevent fixed equinus deformities, allowing successful ambulation with simple prosthetic devices and drastically reducing the need for revision to a higher level.


Surgical Techniques
Technique 10-1: Standard Amputation of a Digit
This technique is utilized for definitive ablation of a severely infected, ischemic, or deformed digit where bone preservation is not viable.

Step-by-Step Approach:
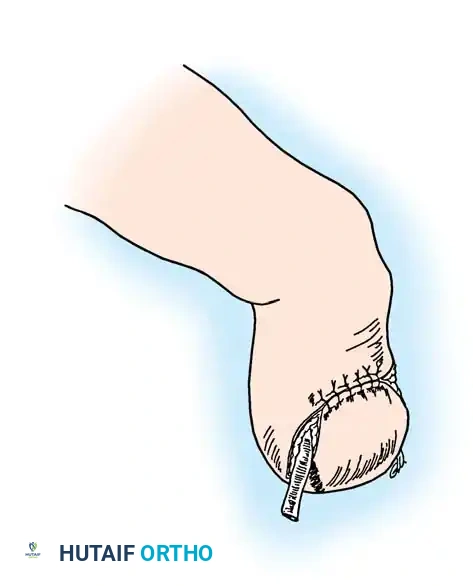
1. Flap Design: Fashion a long plantar and a short dorsal skin flap. The plantar skin is highly specialized for weight-bearing and provides superior durability. Begin the incision at the intended level of bone resection at the medial midpoint of the toe. Curve it dorsally to the lateral midpoint.
2. Plantar Flap: Create a corresponding plantar flap, ensuring it is slightly longer than the dorsoplantar diameter of the toe to allow tension-free closure over the bone stump.
3. Dissection: Elevate the skin flaps proximally to the level of the bone cut using a "no-touch" technique on the epidermal edges.
4. Tendon Management: Divide the flexor and extensor tendons under tension, allowing them to retract deep into the proximal soft tissues.
5. Neurovascular Bundle: Isolate the digital nerves. Apply gentle distal traction, section them sharply, and allow them to retract proximally to prevent painful neuroma formation at the stump. Ligate or cauterize the digital vessels.
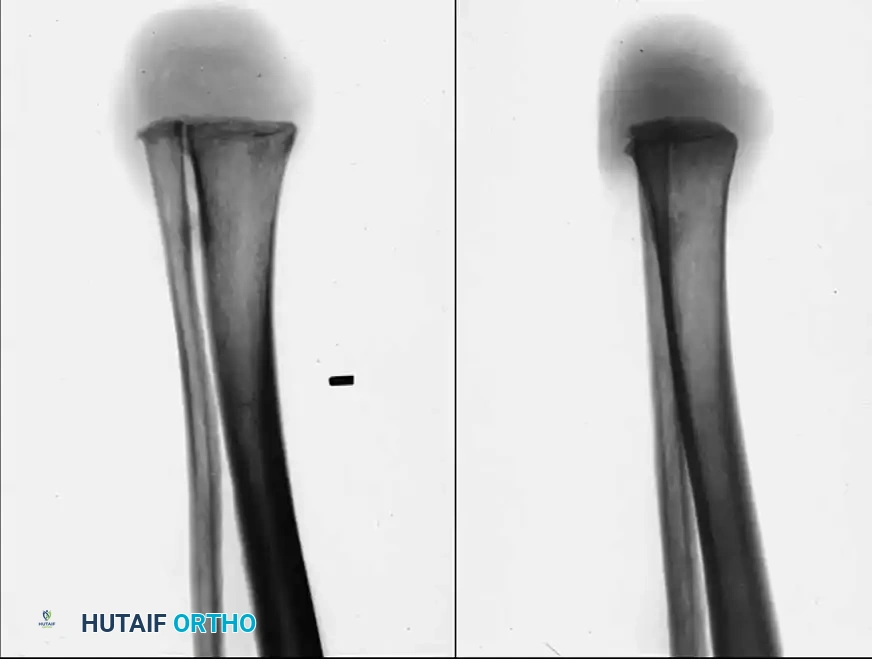
6. Bone Resection: Section the phalanx at the selected level using a microsaw or bone-cutting forceps. Crucially, smooth the distal bone end with a rasp to remove any sharp prominences that could cause internal pressure necrosis.
7. Closure: Irrigate the wound copiously. Close the flaps using interrupted nonabsorbable sutures (e.g., 3-0 or 4-0 nylon).
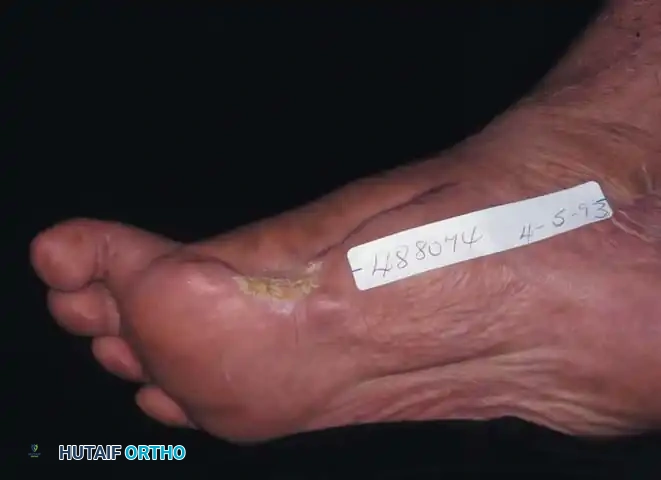
Postoperative Protocol:
Protect the amputation site with a sterile, non-adherent dressing for 12 to 16 days. In dysvascular or diabetic patients, suture removal must be delayed until 21 to 23 days to prevent wound dehiscence. The patient should mobilize in a rigid wooden-soled postoperative shoe or a specialized offloading boot.
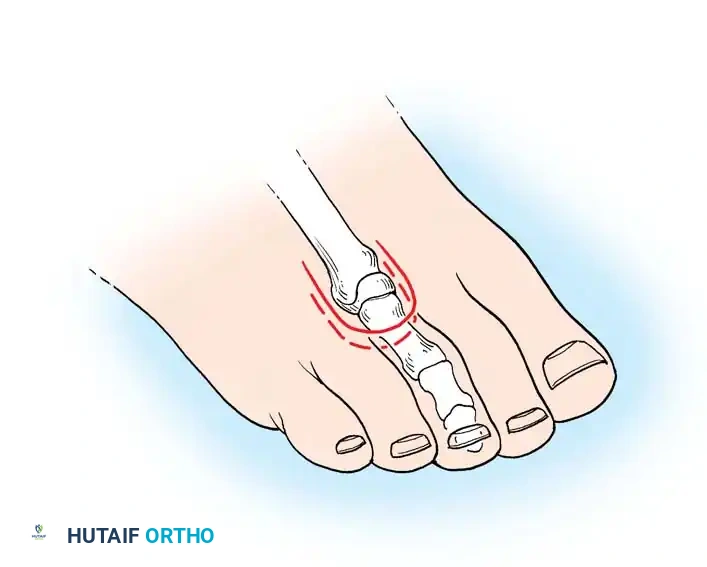
Technique 10-2: Amputation at the Base of the Proximal Phalanx
Whenever oncologically and physiologically possible, maintaining the base of the proximal phalanx is biomechanically superior to a complete metatarsophalangeal (MTP) joint disarticulation.
Rationale:
Retaining at least 1 cm of the proximal phalanx preserves the insertion of the plantar fascia and the intrinsic musculature (e.g., flexor hallucis brevis in the great toe). This maintains a degree of weight-bearing capacity and the windlass mechanism, while also acting as a physical buttress to slow the deviation of adjacent toes.
Step-by-Step Approach:
1. Great Toe Incision: Create a long posteromedial flap. Begin at the dorsal midline base of the toe, curve distally over the medial aspect (distance slightly greater than the AP diameter), and extend proximally across the plantar surface to the web space.
2. Lesser Toes Incision: Utilize a short dorsal racquet-shaped incision. Start 1 cm proximal to the MTP joint, extend distally to the base of the proximal phalanx, and bifurcate around the toe, crossing the plantar surface at the flexor crease.
3. Fifth Toe Incision: Fashion a lateral flap long enough to cover the lateral bony defect, closing the wound by approximating the flap to the medial web skin.
4. Deep Dissection: Reflect the flaps proximally. Draw tendons distally, transect, and allow retraction. Perform traction neurectomies on the digital nerves.
5. Bone Cut: Resect the proximal phalanx, ensuring at least 1 cm of the base remains. Rasp the edges meticulously.
6. Closure: Approximate the skin edges with interrupted nonabsorbable sutures.
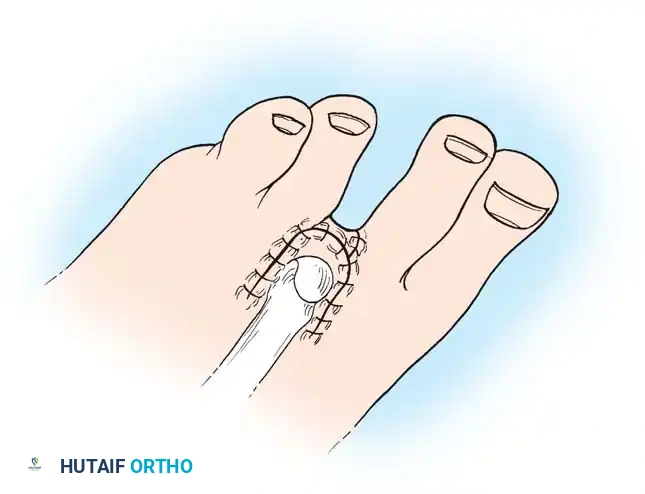
Technique 10-3: Metatarsophalangeal Joint Disarticulation
Disarticulation at the MTP joint is primarily indicated in the diabetic foot presenting with profound ischemia or osteomyelitis extending into the proximal phalanx, precluding bone preservation.


Step-by-Step Approach:
1. Flap Design: The approach mirrors the proximal phalanx amputation, but requires a significantly longer plantar flap to cover the bulky metatarsal head.
2. Joint Exposure: Elevate the flaps to the level of the MTP joint.
3. Capsulotomy: Plantarflex the toe acutely to place the dorsal capsule under tension. Incise the dorsal capsule first.
4. Disarticulation: Straighten the digit, divide the collateral ligaments, and expose the remainder of the joint. Transect the flexor tendons and neurovascular bundles as previously described, completing the disarticulation.
5. Cartilage and Sesamoid Management: In cases of infection, the avascular articular cartilage of the metatarsal head should be denuded to promote granulation. In diabetic patients undergoing hallux disarticulation, the sesamoids are frequently excised to remove plantar pressure points that could lead to future ulceration.
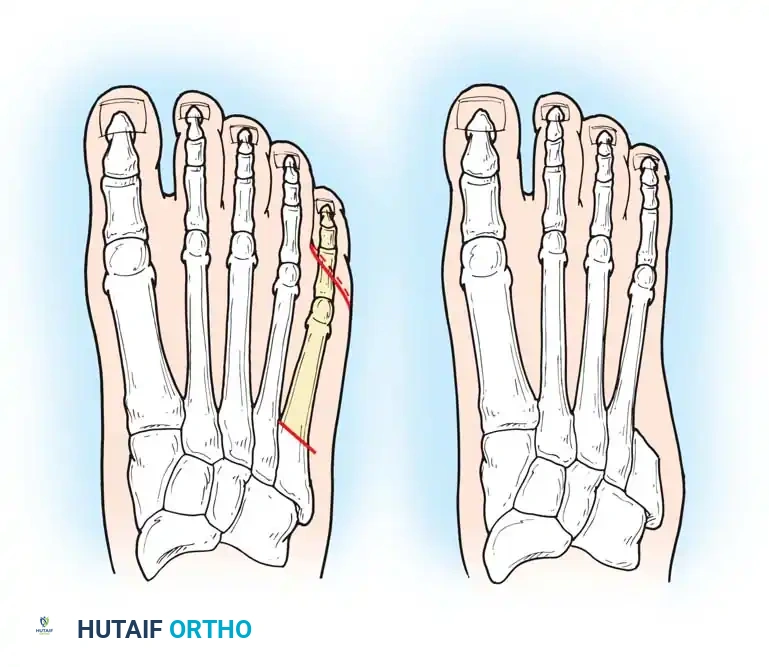
6. Metatarsal Resection (If needed): If skin tension is excessive, or if the metatarsal head is severely prominent/atrophic, the distal metatarsal may be resected (ray amputation) to allow tension-free closure.






You Might Also Like