Comprehensive Surgical Management of Keratotic Foot Lesions
Key Takeaway
Keratotic foot lesions, including heloma durum and heloma molle, result from abnormal biomechanical pressure. Initial management is nonoperative, utilizing friction-absorbing pads and footwear modifications. When conservative measures fail, surgical intervention targeting the underlying osseous prominence—such as metatarsal condylectomy or corrective osteotomy—is indicated. This guide details the pathoanatomy, clinical evaluation, and step-by-step surgical management of intractable plantar keratoses and interdigital corns.
Introduction to Keratotic Foot Lesions
Keratotic lesions of the foot—encompassing hard corns (heloma durum), soft corns (heloma molle), and intractable plantar keratoses (IPK)—represent a hyperkeratotic physiological response to focal, repetitive biomechanical stress. While often dismissed as minor dermatological issues, these lesions are fundamentally orthopedic in nature, arising from underlying osseous prominences, structural deformities, or altered forefoot kinematics.
For the practicing orthopedic surgeon, successful management requires a paradigm shift from treating the cutaneous symptom to addressing the underlying structural pathology. Failure to recognize the biomechanical etiology inevitably leads to recurrence, patient dissatisfaction, and potential complications, particularly in immunocompromised or diabetic populations.
Principles of Nonoperative Management
Initial management of keratotic lesions must remain strictly nonoperative until the patient has exhausted a variety of conservative modalities. The primary goal of conservative care is the redistribution of mechanical forces and the reduction of focal friction.
First-Line Modalities
Patients should be directed to utilize self-help aids widely available in the foot care sections of retail stores. It is highly recommended that orthopedic clinics maintain a small variety of these aids in the office for direct patient instruction and immediate initial treatment.
- Friction-Absorbing Sleeves: We have observed significant clinical success using digital sleeves equipped with friction-absorbing pads consisting of medical-grade paraffin (e.g., Silipos). These devices effectively dissipate shear forces across the interphalangeal joints.
- Footwear Modifications: Transitioning to shoes with a wider toe box, deeper vamp, and rigid sole can dramatically reduce extrinsic pressure on the lesser toes.
- Routine Debridement: Paring down the hyperkeratotic tissue provides immediate, albeit temporary, symptomatic relief and helps prevent the formation of deep adventitial bursae.
Clinical Pearl: Nonoperative management is considered to have failed only if the patient remains highly symptomatic despite compliant use of offloading devices, or if the daily application of these aids becomes excessively time-consuming and detrimental to the patient's quality of life. At this juncture, surgical intervention is warranted.
Biomechanics and the Role of Hallux Valgus
The development of lesser metatarsal callosities is frequently a secondary manifestation of first ray pathology. Hallux valgus deformity compromises the weight-bearing capacity of the first metatarsophalangeal (MTP) joint, leading to transfer metatarsalgia and subsequent hyperkeratosis beneath the lesser metatarsal heads.
As demonstrated in landmark studies by Lee et al., over 90% of patients with lesser metatarsal callosities experience significant improvement of their pain following the anatomical correction of a concomitant hallux valgus deformity.
Surgical Warning: Although symptoms associated with lesser metatarsal callosities may improve following first ray realignment, any fixed deformity of the lesser toe at the MTP joint must be corrected concurrently at the time of hallux valgus correction to obtain complete, long-term symptomatic relief.
Interdigital Soft Corns (Heloma Molle)
Pathoanatomy and Clinical Presentation
Interdigital soft corns are highly troublesome lesions that occur within the web spaces of the toes. Occasionally, a dystrophic nail can produce the pressure necessary for an interdigital corn to develop. However, a slightly less common, but significantly more problematic soft corn occurs at the base of the web space, most frequently in the fourth web space.

These specific corns are biomechanically associated with an abnormally short fifth metatarsal. Furthermore, they are frequently exacerbated by hallux valgus, which causes lateral extrinsic shoe pressure, forcing the fifth toe into adduction against the fourth toe.
The lesion results directly from the focal pressure imposed by the lateral side of the base of the fourth proximal phalanx abutting against the medial condyle of the head of the fifth proximal phalanx (or a combination of both).

Complications and Diabetic Considerations
The confined, moist environment of the interdigital web space macerates and softens the hyperkeratotic area (hence the term "soft" corn).
If left untreated, the continuous friction and maceration can lead to tissue breakdown. Occasionally, a sinus tract develops between the central part of the corn and the deep web space. When this occurs, suppuration and deep space infection usually follow.
Surgical Warning: In a diabetic, neuropathic, or otherwise immunocompromised patient, this relatively minor lesion can rapidly escalate into catastrophic problems, including deep space abscesses, osteomyelitis of the proximal phalanges, and the potential need for digital or ray amputation.
Surgical Technique: Fourth Web Space Condylectomy
When conservative measures fail, surgical excision of the underlying bony prominence is required.
- Positioning and Anesthesia: The patient is placed supine. A regional ankle block or digital block is administered. A forefoot tourniquet may be utilized for hemostasis.
- Incision: A dorsal longitudinal incision is made over the fourth web space, slightly biased toward the toe containing the primary osseous prominence (usually the medial aspect of the fifth proximal phalanx or lateral aspect of the fourth).
- Dissection: Deepen the incision through the subcutaneous tissue, taking care to protect the dorsal cutaneous nerves and the interdigital neurovascular bundle located plantarly.
- Osseous Resection: Expose the prominent medial condyle of the fifth proximal phalanx head. Using a micro-sagittal saw or a sharp rongeur, perform a partial condylectomy. Resect enough bone to ensure that no impingement occurs when the toes are manually compressed together. If the lateral base of the fourth proximal phalanx is also prominent, a conservative resection of this flare is performed.
- Closure: The wound is irrigated copiously and closed with non-absorbable monofilament sutures. A bulky, compressive web-space dressing is applied to prevent hematoma formation.
Intractable Plantar Keratosis (Plantar Corns)
Pathoanatomy
The plantar corn is a severe manifestation of a hard corn (heloma durum and clavus durus). Patients frequently present with a highly localized, circumscribed plug of keratin that may have recently been plucked or debrided from the center of an isolated, hyperkeratotic plaque.

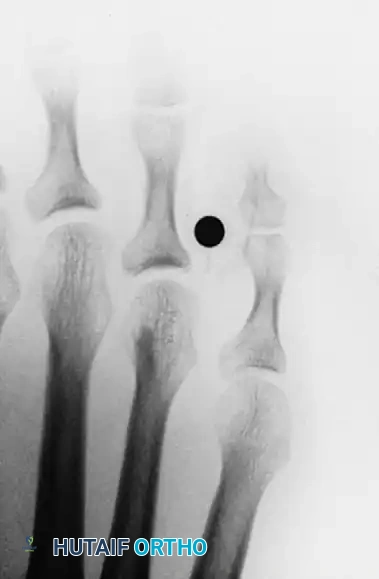
These lesions are almost exclusively located beneath the lesser metatarsal heads, most commonly the second or third. They are the direct result of a prominent plantar condyle of the metatarsal head driving into the plantar fat pad during the stance phase of gait.
As the prominent lateral or medial condyle of the metatarsal head creates focal pressure, the skin responds by forming a dense, conical keratotic wedge that points inward, causing severe sharp pain upon weight-bearing.

Surgical Technique: Plantar Condylectomy vs. Osteotomy
The surgical approach depends on whether the pathology is an isolated prominent condyle or a globally plantarflexed/long metatarsal.
Isolated Plantar Condylectomy (DuVries Approach)
- Incision: A dorsal longitudinal incision is made over the affected MTP joint. (Avoid plantar incisions if possible to prevent painful plantar scarring).
- Exposure: The extensor tendon is retracted, and a dorsal capsulotomy is performed. The collateral ligaments are released to allow acute plantarflexion of the toe, exposing the metatarsal head.
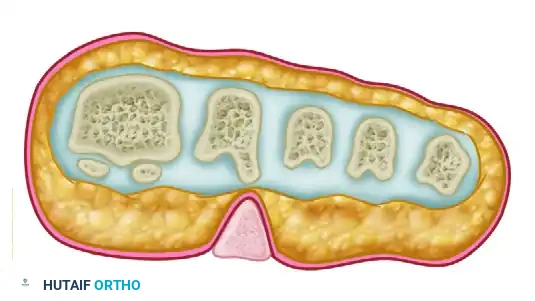
- Resection: Using a McGlamry elevator, the plantar plate is freed from the metatarsal head. A micro-sagittal saw is used to resect the prominent plantar condyle (usually the lateral condyle, as seen in the diagrams above) flush with the metatarsal shaft.
- Closure: The capsule is repaired, and the skin is closed.
Metatarsal Shortening/Elevating Osteotomy (Weil Osteotomy)
If the entire metatarsal is excessively long or plantarflexed, a Weil osteotomy is preferred to elevate and shorten the metatarsal head, thereby globally offloading the keratotic lesion.
Hard Corns (Heloma Durum) of the Lesser Toes
Pathoanatomy
The most common location for a classic hard corn is over the dorsolateral aspect of the proximal interphalangeal (PIP) joint of the fifth toe. This occurs due to the rigid hammer toe deformity of the fifth digit rubbing against the rigid toe box of the shoe.
Because this is the most frequent presentation, the procedure for this specific location is described below; however, the principles can be universally applied to hard corns on other lesser toes.
Surgical Technique: PIP Joint Arthroplasty (Resection Arthroplasty)
- Incision: An elliptical incision is made directly over the corn on the dorsolateral aspect of the fifth toe PIP joint. The hyperkeratotic tissue is excised en bloc with the skin ellipse.
- Dissection: The extensor tendon is transected or split longitudinally. The collateral ligaments of the PIP joint are sharply divided, allowing the joint to be "shotgunned" (hinged open).
- Bone Resection: The head and neck of the proximal phalanx are exposed. Using a bone-cutting forceps or a micro-sagittal saw, the distal portion of the proximal phalanx (the head and neck) is resected.
- Evaluation: Ensure adequate bone has been removed so that the toe is flaccid and no longer impinges against the shoe.
- Closure: The skin is closed with simple interrupted sutures. The toe is splinted in a corrected, straight position using cohesive bandages.
Postoperative Protocol and Rehabilitation
Regardless of the specific procedure performed for keratotic lesions, strict adherence to postoperative protocols is essential for optimal wound healing and prevention of recurrence.
- Weight-Bearing: Patients are typically allowed heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe immediately following surgery.
- Dressing Management: Dressings must remain clean, dry, and intact for the first 10 to 14 days. For web space procedures, a spacer (such as gauze or lamb's wool) should be maintained to prevent maceration and ensure the web space heals open.
- Suture Removal: Sutures are generally removed at 14 to 21 days, depending on the vascular status of the patient and the tension on the wound edges.
- Long-Term Care: Following complete healing, patients must be educated that surgery corrects the osseous prominence, but poor footwear can still cause recurrent skin irritation. Transitioning to wide toe-box shoes and custom orthotics (if transfer metatarsalgia was present) is highly recommended to ensure long-term success.
Conclusion
The successful management of keratotic foot lesions requires a comprehensive understanding of forefoot biomechanics. While conservative measures utilizing friction-absorbing pads and footwear modifications remain the cornerstone of initial treatment, surgical intervention is highly effective for recalcitrant cases. By accurately identifying and resecting the offending osseous prominences—whether through condylectomy, arthroplasty, or corrective osteotomy—the orthopedic surgeon can provide definitive relief for these debilitating lesions.
You Might Also Like

