Fifth Metatarsal Osteotomies for Bunionette Deformity
Key Takeaway
Bunionette deformity, or tailor's bunion, often requires surgical intervention when conservative measures fail. This comprehensive guide details the transverse medial slide osteotomy and the oblique diaphyseal osteotomy (Coughlin technique) of the fifth metatarsal. It covers precise indications, biomechanical principles, step-by-step surgical approaches, fixation strategies, and postoperative rehabilitation protocols to optimize clinical outcomes and minimize complications in forefoot reconstruction.
INTRODUCTION TO BUNIONETTE DEFORMITY AND SURGICAL RATIONALE
Bunionette deformity, historically referred to as a "tailor's bunion," is a painful lateral prominence of the fifth metatarsal head. The pathoanatomy of this condition is multifactorial, often involving a combination of an enlarged fifth metatarsal head, lateral bowing of the fifth metatarsal shaft, or an abnormally widened fourth-to-fifth intermetatarsal angle (IMA). Patients typically present with intractable pain, localized erythema, bursitis, and hyperkeratotic lesions (callosities) over the lateral or plantar-lateral aspect of the fifth metatarsophalangeal (MTP) joint.
When conservative management—such as shoe modification, orthotics, and padding—fails to alleviate symptoms, surgical intervention is indicated. The selection of the appropriate surgical procedure is dictated by the specific anatomical variant of the deformity, which is traditionally classified into three types:
* Type I: Enlarged fifth metatarsal head (hypertrophy of the lateral condyle).
* Type II: Lateral bowing of the distal fifth metatarsal diaphysis.
* Type III: Increased 4-5 intermetatarsal angle (normal is typically less than 8 degrees).
This masterclass details two highly effective, evidence-based osteotomy techniques for the correction of bunionette deformities: the Transverse Medial Slide Osteotomy (ideal for mild-to-moderate deformities) and the Oblique Diaphyseal Osteotomy (the Coughlin technique, reserved for severe splay foot or metatarsus quintus valgus).
TRANSVERSE MEDIAL SLIDE OSTEOTOMY FOR BUNIONETTE DEFORMITY
The transverse medial slide osteotomy is a distal metatarsal osteotomy primarily indicated for Type I and mild Type III bunionette deformities. It is a powerful technique that allows for medial translation of the metatarsal head, effectively reducing the lateral prominence while offering the versatility to alter the sagittal and axial alignment of the fifth ray based on the angle of the osteotomy cut.
Preoperative Planning and Indications
Careful clinical and radiographic evaluation is paramount. Weight-bearing anteroposterior (AP) and lateral radiographs of the foot are required to assess the 4-5 IMA, the fifth MTP angle, and the presence of any degenerative changes within the MTP joint. The transverse medial slide is contraindicated in patients with severe diaphyseal bowing (Type II) or a massively widened 4-5 IMA (severe Type III), where a proximal or diaphyseal osteotomy would be biomechanically superior.
Anesthesia and Patient Positioning
- Anesthesia: The procedure can be performed under general anesthesia, regional anesthesia (popliteal block), or a highly specific local ankle block in carefully selected, compliant patients.
- Positioning: Place the patient in the supine position. A bump may be placed under the ipsilateral hip to internally rotate the lower extremity, bringing the lateral border of the foot into a direct, orthogonal view for the surgeon.
- Hemostasis: Apply a well-padded calf or thigh tourniquet to ensure a bloodless surgical field, facilitating meticulous dissection and precise osteotomy execution.
Surgical Approach
- Incision: Make a longitudinal lateral approach centered over the fifth metatarsal neck, extending from the mid-diaphysis to the proximal phalanx.
- Dissection: Deepen the incision through the subcutaneous tissues. Meticulous care must be taken to identify and retract the dorsal and plantar branches of the dorsolateral cutaneous nerve (a branch of the sural nerve).
- Capsulotomy: Perform a longitudinal or L-shaped capsulotomy to expose the lateral eminence of the fifth metatarsal head and the surgical neck.
🔪 Surgical Warning: Vascular Preservation
The blood supply to the fifth metatarsal head relies heavily on the capsular attachments and the nutrient artery entering the medial diaphysis. Avoid aggressive stripping of the medial soft tissues and periosteum to prevent avascular necrosis (AVN) of the capital fragment.
Osteotomy Execution and Biomechanics
The geometry of the osteotomy dictates the three-dimensional correction of the metatarsal head.
1. Instrumentation: Utilize a standard pneumatic or electric sagittal saw equipped with a fine-toothed blade (specifically, a 9.5 × 25 × 0.4-mm blade is recommended to minimize bone loss from the kerf).
2. Length Preservation: If the length of the fifth metatarsal bone is to be maintained, incline the osteotomy in a strictly lateral-to-medial direction so that the blade is perfectly perpendicular to the longitudinal axis of the fourth ray.
3. Shortening and Decompression: If shortening of the metatarsal or decompression of the MTP joint is necessary (frequently indicated in patients with mild concurrent osteoarthritis or a rigid joint), incline the osteotomy in a distal-proximal direction up to 25 degrees. This allows the capital fragment to slide proximally as it translates medially.
4. Lengthening (Rare): In the rare event that lengthening of the fifth metatarsal is required to restore the lateral column parabola, incline the osteotomy in a proximal-distal direction up to 15 degrees.
Fixation Strategy
- Translate the distal capital fragment medially by approximately 30% to 50% of the shaft width.
- K-wire Buttress: Insert a 1.6-mm (0.062-inch) Kirschner wire retrograde through the lateral soft tissues of the fifth toe. Pass it across the MTP joint, through the medullary canal of the translated metatarsal head, and drive it into the base of the fifth metatarsal.
- This intramedullary K-wire acts as an internal splint and buttress, preventing the loss of position of the distal fragment and stabilizing the MTP joint.
- Cut the wire, leaving it protruding distally through the skin for easy removal in the clinic.
Postoperative Care Protocol
- Immobilization: The patient is placed in a bulky compressive dressing and a hard-soled postoperative shoe.
- Weight-Bearing: Heel-touch or flat-foot protective weight-bearing is permitted.
- Hardware Removal: The protruding K-wire is removed in the outpatient surgery department at exactly 6 weeks postoperatively, coinciding with radiographic evidence of clinical union.
- Rehabilitation: Following wire removal, transition to a wide-toe-box shoe and commence active and passive range-of-motion (ROM) exercises of the fifth MTP joint.
OBLIQUE DIAPHYSEAL OSTEOTOMY OF THE FIFTH METATARSAL (COUGHLIN TECHNIQUE)
For patients presenting with severe splay foot, metatarsus quintus valgus, or a profoundly widened 4-5 IMA (severe Type III deformity), distal osteotomies are biomechanically insufficient. The Oblique Diaphyseal Osteotomy, popularized by Coughlin, provides a powerful correction by utilizing the diaphyseal bone stock to achieve significant medial rotation and translation, effectively narrowing the forefoot.
Indications and Preoperative Considerations
This technique is the gold standard for severe deformities where the 4-5 IMA exceeds 10 to 12 degrees. It is particularly adept at addressing concurrent plantar keratoses, as the obliquity of the cut can be manipulated to elevate the metatarsal head in the sagittal plane.
💡 Clinical Pearl: Rotation vs. Translation
A critical biomechanical principle of the Coughlin diaphyseal osteotomy is that the distal fragment is rotated medially rather than simply translated. Rotation ensures maximal cortical bony contact at the osteotomy site (promoting reliable osteosynthesis) and inherently maintains metatarsal length, preventing transfer metatarsalgia to the fourth ray.
Surgical Approach and Soft Tissue Release
- Incision: Make a longitudinal incision centered on the dorsolateral aspect of the fifth metatarsal, extending from the base of the fifth metatarsal proximally to the middle of the proximal phalanx distally.
- Nerve Protection: Carefully dissect the subcutaneous tissue. It is imperative to identify and protect the dorsolateral cutaneous nerve throughout the procedure. Retraction should be gentle to avoid neuropraxia.
- Muscle Reflection: Reflect the abductor digiti quinti muscle plantarward to expose the lateral aspect of the fifth metatarsal diaphysis. Crucially, leave the soft tissue and periosteal attachments to the medial aspect of the metatarsal intact. This preserves the vital medial vascular hinge.
- Capsular Exposure: Expose the MTP joint capsule. Make an L-shaped incision along the dorsal and proximal aspects of the capsule to expose the lateral eminence of the metatarsal head.
- Condylectomy: After the capsule is detached, use a sagittal saw to resect the hypertrophic lateral condyle of the metatarsal head, ensuring the cut is flush with the lateral cortex of the diaphysis.
- Medial Release: Distract the MTP joint by applying distal traction to the fifth toe. Release the medial capsule of the MTP joint. This release is mandatory; without it, the toe cannot be properly realigned on the newly positioned metatarsal head after the osteotomy is completed.
Osteotomy Execution and Multi-Planar Correction
The orientation of the saw blade during the diaphyseal cut is the most critical step of the procedure, as it dictates the final position of the metatarsal head.
Scenario A: Pure Lateral Keratosis
For a deformity presenting with only a lateral prominence and no plantar callosity, the goal is pure transverse plane correction. Direct the saw cut from lateral to medial, with the obliquity oriented from a dorsal-proximal to a plantar-distal direction.
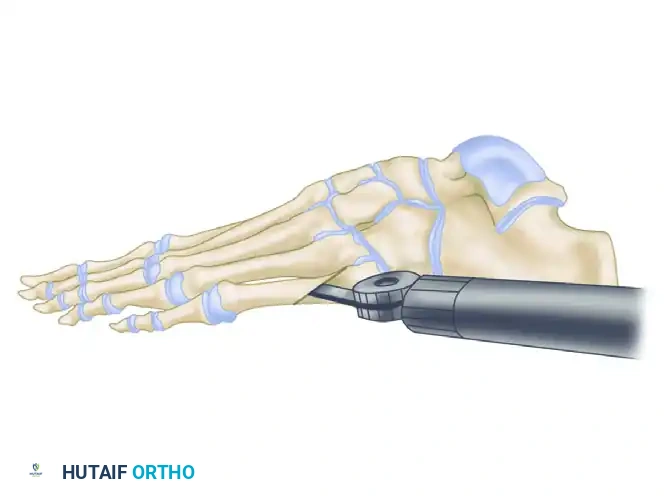
Figure A: Saw cut directed from lateral to medial with obliquity oriented from dorsal-proximal to plantar-distal for pure lateral keratosis.
Scenario B: Plantar and Lateral Keratoses
If the patient presents with both a lateral bunionette and a painful plantar callosity beneath the fifth metatarsal head, sagittal plane elevation is required. Angle the saw blade slightly upward (cephalad) as you make the cut. This geometry ensures that as the distal fragment is rotated medially, it simultaneously elevates, decompressing the plantar aspect of the foot. For a pure plantar keratosis where maximum elevation is desired, the obliquity of the osteotomy should be increased.
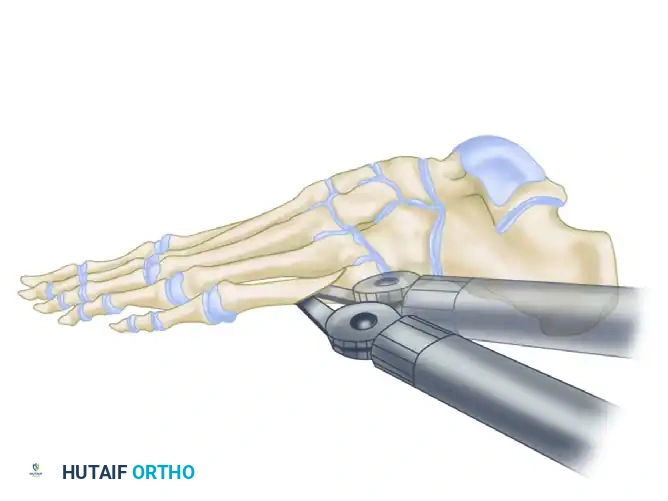
Figure B: In the presence of a plantar callosity, the saw blade is directed cephalad so that the fifth metatarsal head is elevated when the osteotomy site is rotated.
Pre-Drilling and Completion of the Osteotomy
- Pre-Drilling: Before completely finishing the saw cut through the medial cortex, drill the planned fixation holes in the proximal and distal fragments. Because the fifth metatarsal diaphysis is exceptionally narrow, attempting to drill these holes after the osteotomy is complete and the bone is mobile can be highly difficult and risks cortical blowout.
- Completion and Rotation: Complete the osteotomy through the medial cortex. Gently rotate the distal fragment medially so that its longitudinal axis becomes parallel with the fourth metatarsal. Use the pre-drilled fixation hole as the central axis for this rotation.

Figure C: The osteotomy is rotated in the diaphyseal region until the distal fragment is parallel with the fourth metatarsal, maximizing bony contact and maintaining length.
Fixation and Capsulorrhaphy
- Osteosynthesis: Fix the osteotomy rigidly. Options include a single small fragment lag screw, a combination of a screw and a K-wire for rotational stability, or multiple K-wires. Alternatively, one or two dorsoplantar 2.4-mm or 2.7-mm titanium compression screws provide excellent biomechanical stability.
- Soft Tissue Realignment: Realign the fifth toe by reefing (plicating) the lateral capsule to the fifth metatarsal metaphyseal periosteum and the abductor digiti quinti.
- Bone Anchoring: If the local soft tissue is insufficient or too friable to securely attach the MTP capsule, place interrupted non-absorbable sutures through small drill holes made directly in the metaphysis. This robust capsular plication is essential; it allows for significant correction of any residual axial malalignment or malrotation of the digit.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the subcutaneous tissues and skin in the usual manner. Apply a sterile, mildly compressive gauze and tape dressing.
Postoperative Care Protocol
- Dressing Changes: The surgical dressing is changed weekly for the first 6 weeks to monitor wound healing and maintain the toe in the corrected alignment using specialized taping techniques.
- Weight-Bearing: Ambulation is allowed immediately in a rigid, wooden-soled postoperative shoe, bearing weight primarily on the heel and medial column.
- Casting: For unreliable patients, those with neuropathy, or patients who are unsteady when walking, a short-leg walking cast is highly recommended to prevent catastrophic hardware failure or loss of reduction.
- Radiographic Follow-up: Serial radiographs are obtained at 2, 6, and 12 weeks to assess for callus formation and definitive bony union. Transition to normal footwear is typically permitted between 8 to 10 weeks, depending on radiographic consolidation.
COMPLICATIONS AND PITFALLS
While both the transverse medial slide and oblique diaphyseal osteotomies yield high satisfaction rates, surgeons must be vigilant regarding potential complications:
- Delayed Union and Nonunion: The fifth metatarsal diaphysis has a tenuous watershed blood supply. Excessive periosteal stripping, particularly on the medial side during the Coughlin procedure, can lead to delayed union or nonunion. Rigid internal fixation and strict adherence to postoperative weight-bearing restrictions are critical.
- Transfer Metatarsalgia: Excessive shortening of the fifth metatarsal or over-elevation of the capital fragment can transfer weight-bearing forces to the fourth metatarsal head, resulting in iatrogenic transfer metatarsalgia. Precise preoperative planning and intraoperative execution of the saw blade angle are required to prevent this.
- Nerve Injury: The dorsolateral cutaneous nerve is highly vulnerable during the surgical approach. Neuroma formation or chronic regional pain syndrome (CRPS) can result from aggressive retraction or direct laceration.
- Hardware Prominence: Due to the minimal soft tissue envelope on the lateral border of the foot, screw heads or K-wires may become prominent and painful, necessitating secondary hardware removal once the osteotomy has fully united.
By adhering to strict biomechanical principles, respecting the soft tissue envelope, and selecting the appropriate osteotomy based on the specific deformity type, orthopedic surgeons can achieve excellent, reproducible outcomes in the management of bunionette deformities.
You Might Also Like


