Total Nail Plate Removal: Surgical Technique & Outcomes
Key Takeaway
Total nail plate removal is a specialized orthopedic procedure primarily indicated for severe paronychia or abscesses circumducting the nail plate. This comprehensive guide details the step-by-step surgical technique, emphasizing atraumatic elevation to preserve the germinal matrix. It also covers essential postoperative protocols, biomechanical considerations, and the management of potential complications, such as the upward-turned pulp deformity associated with multiple avulsions.
INTRODUCTION TO TOTAL NAIL PLATE REMOVAL
Total nail plate removal—specifically without concomitant matrix removal (matrixectomy)—is a targeted orthopedic and podiatric surgical intervention. While partial nail avulsion is the gold standard for localized ingrown toenails (onychocryptosis), total nail plate avulsion is reserved for specific, severe pathologies where partial resection cannot provide adequate therapeutic drainage or mechanical relief.
As an isolated procedure, total nail plate removal is rarely indicated for routine ingrown toenails due to unacceptably high recurrence rates. However, in the presence of a circumferential abscess, severe fungal infections (onychomycosis) refractory to medical management, or acute trauma with subungual hematoma compromising the entire nail bed, total avulsion becomes a necessary and highly effective intervention. The primary benefits of total nail avulsion are the uniformly rapid relief of acute symptoms and the immediate resolution of underlying soft-tissue infection.
This comprehensive guide details the biomechanical considerations, precise surgical techniques, and postoperative protocols required to perform a total nail plate removal while minimizing iatrogenic trauma to the underlying sterile and germinal matrices.
SURGICAL ANATOMY AND BIOMECHANICS
To perform a total nail plate removal without causing permanent dystrophy to the future regenerating nail, the surgeon must possess a flawless understanding of the perionychial anatomy.
Anatomy of the Nail Unit
The nail unit (perionychium) consists of several distinct anatomical structures:
* Nail Plate: The hard, keratinized structure that provides dorsal protection to the distal phalanx.
* Germinal Matrix: Located proximally, extending beneath the eponychium (cuticle) to the lunula. It is responsible for 90% of nail plate generation. Iatrogenic damage here results in permanent nail deformity or absent growth.
* Sterile Matrix: Extends from the lunula to the hyponychium. It provides adherence for the nail plate and contributes slightly to its thickness. The sterile matrix features longitudinal ridges that interlock with the ventral surface of the nail plate.
* Eponychium and Paronychium: The proximal and lateral soft tissue folds that frame the nail plate.
* Hyponychium: The distal soft tissue boundary where the nail bed meets the glabrous skin of the toe pulp.
Biomechanics of the Hallux Nail
The nail plate is not merely a protective shield; it is a critical biomechanical buttress. During the toe-off phase of the gait cycle, ground reaction forces compress the plantar aspect of the distal toe pulp. The rigid dorsal nail plate provides a counter-force, preventing the soft tissues of the distal tuft from migrating dorsally.
When the nail plate is totally removed, this dorsal counter-force is lost. Consequently, the distal pulp tends to migrate dorsally over time. If this occurs before the new nail can fully regenerate, the regenerating nail will encounter a wall of hypertrophied soft tissue, leading to distal embedding and the classic "turned-up pulp deformity."
INDICATIONS AND CONTRAINDICATIONS
Primary Indications
Total nail plate removal without matrixectomy is strictly indicated in the following clinical scenarios:
1. Circumferential Abscess: The primary indication occurs when an abscess has circumducted the nail on both sides and extended proximally beneath the eponychium. In such cases, a partial nail plate removal would fail to provide adequate drainage for the trapped purulence.
2. Severe Onychomycosis: As an adjunct to topical or systemic antifungal therapy when the nail plate is severely thickened, dystrophic, and acting as a barrier to treatment.
3. Acute Trauma: Severe crush injuries resulting in a subungual hematoma involving >50% of the nail bed, or when the nail plate is partially avulsed and acting as a foreign body preventing nail bed repair.
Contraindications
- Ischemia: Severe peripheral arterial disease (PAD) where the healing capacity of the toe is compromised.
- Suspected Melanoma: Subungual melanomas or unexplained longitudinal melanonychia require biopsy, not simple avulsion.
- Routine Ingrown Toenails: Total avulsion is contraindicated as a primary treatment for simple onychocryptosis due to high recurrence rates.
💡 Clinical Pearl: The Limits of Total Avulsion
Never perform a total nail plate removal for a simple, unilateral ingrown toenail. The recurrence rate of ingrown toenails after total nail removal ranges from 32% to 78% in published reports. Furthermore, the recurrence rate after a second total avulsion skyrockets to 70% to 80%. Always opt for partial avulsion with chemical or surgical matrixectomy for localized disease.
PREOPERATIVE PREPARATION
Patient Counseling and Informed Consent
Informed consent is critical, as the aesthetic and functional recovery from this procedure is prolonged. The patient must be explicitly informed of the following before surgery:
* Regrowth Timeline: The nail takes 4 to 6 months to re-form completely, heavily dependent on the patient’s age, vascular status, and nutritional health.
* Risk of Deformity: Patients must be forewarned that an upward-turned deformity of the distal nail bed and pulp may develop. This risk increases exponentially if the patient has a history of multiple prior nail avulsions.
* Recurrence: If performed for an ingrown toenail, the high risk of recurrence must be documented.
Anesthesia and Positioning
- Positioning: The patient is placed in the supine position. The foot is prepped and draped in a standard sterile fashion.
- Anesthesia: A standard digital block of the hallux is performed using a 1:1 mixture of 1% Lidocaine and 0.5% Bupivacaine. Ensure complete anesthesia of the four digital nerves (two plantar, two dorsal) before proceeding.
- Hemostasis: A sterile digital tourniquet (e.g., a Penrose drain or a rolled surgical glove finger) is applied to the base of the hallux to provide a bloodless surgical field, which is essential for visualizing the matrix.
SURGICAL TECHNIQUE: STEP-BY-STEP
The overarching goal of this technique is the atraumatic separation of the nail plate from the underlying sterile and germinal matrices. Forceful avulsion will tear the matrix, leading to permanent scarring and a dystrophic regenerated nail.
Step 1: Midline Elevation
Once the great toe has been fully anesthetized and exsanguinated, the initial separation begins.
- Select a straight, thin hemostat, a Freer elevator, or a small, flat nasal elevator.
- Introduce the instrument beneath the distal free edge of the nail in the midline (at the hyponychium).
- Gently pass the elevator proximally, maintaining the instrument perfectly flat against the ventral surface of the nail plate to avoid gouging the sterile matrix below.
- Advance the instrument several millimeters proximal to the proximal nail fold, ensuring it reaches adjacent to the lunula where the germinal matrix resides.

Diagram A: Initial midline insertion of the flat elevator beneath the nail plate, advancing proximally toward the eponychium.
Step 2: Lateral Margin Release
The most common error during nail avulsion is sweeping the elevator side-to-side (medial to lateral) in an attempt to free the nail quickly.
⚠️ Surgical Warning: Avoid Transverse Sweeping
Do not shift the hemostat or elevator back and forth in a windshield-wiper motion. The sterile matrix features delicate longitudinal ridges. Transverse sweeping will lacerate these ridges, causing severe bleeding, matrix scarring, and subsequent split or deformed nail regrowth.
- Instead of sweeping, completely withdraw the elevator from the midline track.
- Re-insert the instrument in a similar, strictly longitudinal manner beneath each lateral margin of the nail, adjacent to the lateral nail folds.
- Repeat this longitudinal withdrawal and insertion across the entire width of the nail plate until the plate is completely separated from the sterile matrix.
Diagram B: Longitudinal release of the lateral margins. Note the strict adherence to proximal-distal movements to preserve the longitudinal ridges of the sterile matrix.
Step 3: Extraction of the Nail Plate
Once the nail plate is freed from the sterile matrix, it must be extracted from the proximal eponychial fold.
- Grasp the freed nail plate with a heavy hemostat or needle driver.
- Apply a firm, steady, distal pull. In most cases, the nail should become loose enough to extract smoothly.
- Managing Adhesions: If the nail root still adheres tightly to the eponychium, do not forcefully jerk the nail root loose. Forceful jerking will avulse the germinal matrix.
- Instead, utilize sharp dissection. Take a small blade (e.g., a #15 or #64 Beaver blade) and carefully dissect between the dorsal surface of the nail plate and the ventral surface of the eponychium.
- This sharp release allows the nail plate to be gently lifted from its bed with little chance of damage to the germinal matrix, significantly reducing bleeding from the nail bed.

Diagram C: Atraumatic distal extraction of the nail plate following complete longitudinal elevation and sharp release of eponychial adhesions.
Alternative Technique: Another choice to remove the last moorings of the nail root is the use of a wide, flat, nasal elevator to gently pry the proximal plate from the eponychial fold, provided it is done with minimal dorsal force.
POSTOPERATIVE CARE PROTOCOL
Meticulous postoperative care is essential to prevent infection, manage pain, and optimize the environment for the 4 to 6 months of nail regeneration.
Immediate Postoperative Phase (Days 0-7)
- Dressing Application: Immediately following the removal of the tourniquet, a nonadherent, single-layer dressing (e.g., Adaptic, Xeroform, or Mepitel) is applied directly to the exposed, raw nail bed.
- Compression: A gently wrapped compression bandage (using sterile gauze and cohesive wrap) is applied to control capillary oozing.
- Elevation: The patient is instructed to keep the foot strictly elevated above heart level for the first 24 hours to minimize throbbing pain and hematoma formation.
- Wound Care: After 24 to 48 hours, the initial dressing is removed. The patient is instructed to begin warm water and Epsom salt soaks for 10-15 minutes, twice daily. Following the soak, a thin layer of topical antibiotic ointment and a fresh, light bandage should be applied.
- Footwear: No constricting hosiery or tight-fitting shoes should be worn for at least 1 week. Open-toed sandals or a rigid postoperative shoe are recommended to prevent microtrauma to the exquisitely sensitive exposed matrix.
Long-Term Monitoring (Weeks to Months)
- The exposed nail bed will gradually desiccate and form a protective keratinized layer over the first 2 to 3 weeks. At this point, daily bandaging can be discontinued.
- The patient should be monitored periodically to ensure the new nail plate is tracking properly over the distal pulp without embedding.
COMPLICATIONS AND OUTCOMES
While total nail plate removal provides uniformly rapid relief of acute symptoms and resolution of infection, it is fraught with long-term biomechanical complications, particularly if misused for chronic ingrown toenails.
High Recurrence Rates
As previously noted, the recurrence rate of ingrown toenails after total nail removal is unacceptably high:
* Primary Total Avulsion: 32% to 78% recurrence.
* Secondary Total Avulsion: 70% to 80% recurrence.
Because the underlying pathology (a mismatch between the width of the nail plate and the width of the nail bed) is not addressed by simple avulsion, the regenerating nail will inevitably incurvate and re-penetrate the lateral folds.
The Upward-Turned Pulp Deformity
The most significant structural complication of total nail plate removal is the upward-turned deformity of the distal nail bed and pulp.
Pathophysiology:
When the rigid nail plate is removed, the distal toe pulp loses its dorsal restraint. During ambulation, the upward pressure from the ground forces the distal soft tissues to migrate dorsally. Over the 4 to 6 months it takes for the new nail to grow, this dorsally migrated tissue hypertrophies, creating a fleshy wall at the distal end of the toe.
When the new nail plate finally reaches the distal tuft, it collides with this hypertrophied tissue. Unable to ride over the pulp, the nail embeds directly into it, causing severe pain, distal onychocryptosis, and cessation of forward nail growth.
Risk Factors:
This deformity is exponentially more likely to occur if the patient has had multiple previous nail avulsions, as the soft tissues become increasingly lax and prone to dorsal migration with each subsequent procedure.
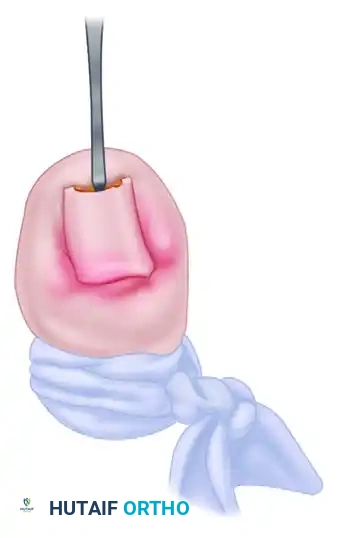
FIGURE 87-6: Clinical manifestations of the turned-up pulp deformity. (A and B) Turned up pulp deformity after multiple nail avulsions for the treatment of ingrown toenails. Note the hypertrophied distal tissue blocking the path of the regenerating nail. (C) Severe turned-up deformity after several historical nail avulsions, resulting in permanent distal embedding.
Management of the Deformity:
If an upward-turned pulp deformity develops and prevents normal nail growth, conservative measures (such as taping the pulp down) are rarely effective. Surgical intervention is often required, which may include:
* Distal Syme Amputation: Resection of the distal half of the terminal phalanx with the overlying nail bed to permanently remove the conflict.
* Soft Tissue Resection (Dubois or Super-U procedures): Excision of the hypertrophied distal pulp to clear a path for the advancing nail plate.
CONCLUSION
Total nail plate removal is a powerful, rapidly effective procedure for resolving severe, circumducting perionychial abscesses and acute subungual pathology. However, its utility is strictly limited by its high recurrence rates for standard onychocryptosis and the severe biomechanical consequence of the upward-turned pulp deformity.
Orthopedic surgeons and podiatric specialists must execute the procedure with meticulous, atraumatic, longitudinal elevation to preserve the delicate germinal and sterile matrices. Furthermore, exhaustive preoperative patient counseling regarding the 4 to 6 month regrowth period and the risks of distal pulp hypertrophy is mandatory to ensure appropriate clinical expectations and optimal long-term outcomes.
===```
You Might Also Like
