Supramalleolar Osteotomy: Surgical Techniques & Protocols
Key Takeaway
Supramalleolar osteotomy is a powerful joint-preserving procedure indicated for distal tibial and fibular malunions where tibiotalar congruity is maintained but the ankle axis is in varus or valgus. This guide details the biomechanical principles, surgical approaches, and step-by-step techniques for dome, opening wedge, and closing wedge osteotomies, ensuring optimal alignment restoration and long-term joint preservation.
Introduction to Supramalleolar Osteotomy
The management of distal tibia and fibula malunions presents a complex biomechanical challenge for the orthopedic surgeon. Occasionally, a malunion of the distal tibia and fibula occurs in which the normal tibiotalar relationships are retained, yet the ankle is driven into a pathological valgus or varus alignment. In these specific clinical scenarios, a supramalleolar osteotomy is the recommended joint-preserving intervention.
The primary goal of a supramalleolar osteotomy is to realign the mechanical axis of the lower extremity, thereby redistributing the weight-bearing forces evenly across the tibiotalar joint. By correcting the extra-articular deformity, the surgeon can prevent or delay the onset of post-traumatic osteoarthritis, alleviate pain, and restore normal gait kinematics. Depending on the specific geometry of the deformity, leg-length discrepancies, and soft-tissue constraints, the surgeon may elect to perform a dome osteotomy, an opening wedge osteotomy, a closing wedge osteotomy, or utilize gradual correction via distraction osteogenesis (the Ilizarov method).
Biomechanics and Preoperative Planning
Thorough preoperative planning is the cornerstone of a successful supramalleolar osteotomy. The surgeon must meticulously evaluate full-length, weight-bearing radiographs of the bilateral lower extremities to determine the mechanical axis deviation (MAD) and identify the Center of Rotation of Angulation (CORA).
Selecting the Osteotomy Type
The choice of osteotomy is dictated by the plane of the deformity, the presence of leg-length discrepancy, and the quality of the surrounding soft tissue envelope.
- Dome Osteotomies: Because dome osteotomies do not sacrifice length to gain correction of the deformity, they are highly preferred in malunions associated with preexisting shortening. They allow for rotation of the distal fragment around a central axis without inducing secondary translation. However, dome osteotomies are significantly more effective in correcting deformities in the frontal (varus-valgus) plane than in the sagittal (flexion-extension) plane.
- Closing Wedge Osteotomies: A properly positioned closing wedge osteotomy can be used to correct complex, multiplanar deformities. These osteotomies provide broad, highly vascularized cancellous bony surfaces that promote rapid healing. The primary disadvantage is that they inherently cause some shortening of the extremity.
- Opening Wedge Osteotomies: These osteotomies maintain or even restore limb length. However, they create a structural void that requires bone grafting (typically autogenous iliac crest) to fill the gap, and they rely heavily on the integrity of the medial or lateral soft tissue hinge.
- Gradual Correction: The Ilizarov method of gradual deformity correction with distraction osteogenesis can also be used, particularly in cases of severe multiplanar deformities, poor soft tissue envelopes, or active infection.
💡 Clinical Pearl: The CORA Principle
When planning a supramalleolar osteotomy, aligning the osteotomy cut as close to the CORA as possible minimizes the risk of creating a secondary translational deformity. If the osteotomy must be performed at a distance from the CORA due to poor bone quality or soft tissue constraints, the surgeon must plan for a translation of the distal fragment to restore the mechanical axis.
Surgical Approaches and Positioning
The patient is positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to correct natural external rotation, bringing the patella and ankle mortise into a true anteroposterior (AP) alignment. A sterile thigh tourniquet is applied. Intraoperative fluoroscopy is mandatory and must be positioned to allow unobstructed AP and lateral views of the ankle and the entire tibia.
The Anterolateral Henry Approach
For the exposure of the distal tibia, particularly when performing a dome osteotomy, the anterolateral Henry approach is highly recommended.
- Make a longitudinal incision lateral to the tibial crest, extending distally toward the ankle joint.
- Incise the deep fascia in line with the skin incision.
- Identify the interval between the tibialis anterior and the extensor hallucis longus (EHL).
- Carefully retract the neurovascular bundle (anterior tibial artery and deep peroneal nerve) laterally alongside the EHL and extensor digitorum longus (EDL).
- Elevate the periosteum to expose the distal tibial metaphysis.
Surgical Technique: Dome Osteotomy
The dome osteotomy is a technically demanding procedure that requires precise execution to ensure a congruent arc of rotation.
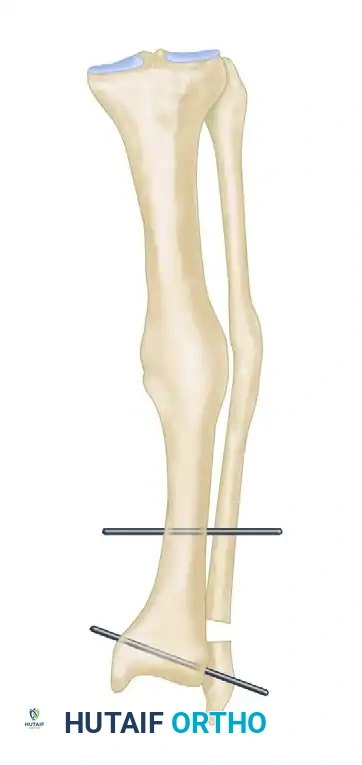
FIGURE 58-11A: Supramalleolar osteotomy. A dome osteotomy is created 1.0 to 1.5 cm proximal to the ankle joint. Threaded pins are inserted parallel to the ankle and knee joint lines.
Step-by-Step Execution
- Exposure: Expose the distal tibia through the anterolateral Henry approach as described above.
- Drilling the Arc: Use a 3.2-mm drill bit to create a series of bicortical holes in the distal tibial metaphysis in the shape of an arc, convex superiorly. The medial and lateral edges of the arc should be strictly 1.0 to 1.5 cm proximal to the ankle joint line. The height of the arc at its apex should also be 1.0 to 1.5 cm.
- Fibular Osteotomy: Through the same anterolateral incision (by retracting laterally) or via a separate lateral incision, expose the fibula. Make an osteotomy at the exact same level as the tibial osteotomy.
- For Varus Malunions: Resect 1 to 3 cm of the fibula to allow for adequate angular correction without impingement.
- For Valgus Malunions: Make a simple oblique osteotomy of the fibula to allow it to slide during correction.
- Completing the Tibial Cut: Use a narrow oscillating saw or a sharp osteotome to connect the holes drilled anteriorly, medially, and laterally in the tibia.
- Pin Placement for Correction: Under strict fluoroscopic control, insert a 4-mm or 5-mm threaded pin transversely from medial to lateral into the distal tibial fragment, perfectly parallel to the ankle joint line.
- Surgical Warning: Keep the pin out of the joint space, away from the osteotomy site, and strictly avoid the anterior neurovascular bundle.
- Proximal Pin Placement: Insert a second 4-mm or 5-mm bicortical threaded pin 6 to 10 cm proximal to the osteotomy, ensuring it is perfectly parallel to the knee joint line.
- Osteoclasis and Correction: With a broad osteotome, complete the tibial osteotomy through the posterior cortex. Correct the varus or valgus deformity by manipulating the distal fragment until the two threaded pins are perfectly parallel to one another.
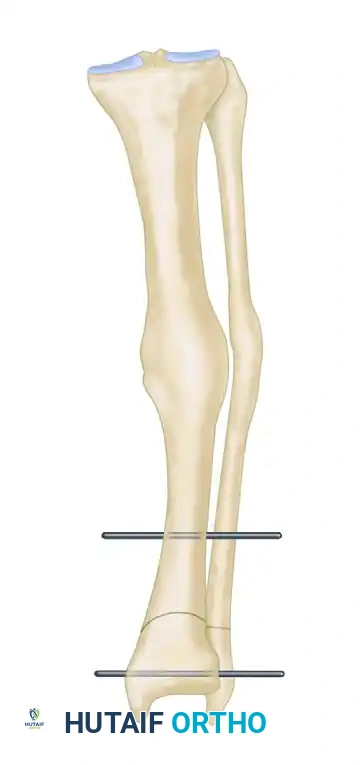
FIGURE 58-11B: Osteotomy is completed, and pins are brought parallel to correct the varus or valgus deformity.
🔪 Surgical Pitfall: Incomplete Correction
If complete reduction is not obtained after mobilizing the osteotomy, do not force the correction. It may be necessary to resect more of the fibula or to perform a more extensive soft tissue release, specifically targeting the interosseous membrane, which often tethers the distal fragment.
Fixation Strategies for Dome Osteotomy
Once the reduction is radiographically acceptable, the surgeon must choose the appropriate fixation construct:
- External Fixation: Connect the parallel pins with an external fixator bar and apply compression across the dome. Additional external fixation pins can be placed in the proximal tibia and the talus to increase construct rigidity.
- Internal Fixation: Alternatively, if the soft tissue coverage is adequate and there is no active infection, stabilize the osteotomy with a 3.5-mm dynamic compression plate (DCP) or a modern anatomical locking plate, and subsequently remove the two external fixation pins. The fibula can also be stabilized with a one-third tubular plate if desired. The use of bone grafting at the osteotomy site is left to the surgeon’s discretion based on the quality of bony contact.
Surgical Technique: Wedge Osteotomies
Wedge osteotomies are highly effective for single-plane deformities and can be tailored as either opening or closing wedges based on limb length requirements.
Opening Wedge Osteotomy
An opening wedge osteotomy is typically performed on the concave side of the deformity to restore length and correct angulation.
- Fibular Management: Through a lateral longitudinal incision, expose and osteotomize the fibula as previously described to permit correction of either the varus or valgus deformity.
- Tibial Exposure: Through the same incision (or a separate medial incision depending on the wedge location), expose the surface of the tibia approximately 1.3 cm proximal to the joint line.
- Osteotomy and Osteoclasis: Drive a wide osteotome transversely almost through the bone, intentionally leaving the opposite cortex intact to act as a soft-tissue/bony hinge. Carry out a manual osteoclasis to open the wedge to the preoperatively calculated angle.
- Bone Grafting: Insert cancellous iliac bone, or use a precisely contoured wedge-shaped structural graft taken from the shaft of the tibia or iliac crest, into the opened side of the osteotomy to pack it open and maintain the correction.
- Fixation: Stabilize the osteotomy with an external fixator applied in the standard fashion with pins through the tibia and talus, or utilize a robust locking plate construct.
Closing Wedge Osteotomy
If the fractures have healed in a varus position and limb length is not a primary concern, a closing wedge osteotomy of the tibia can be made in a similar fashion.
- Calculate the exact angle of the wedge to be removed based on the MAD.
- Perform the fibular osteotomy.
- Remove the predetermined wedge of bone from the convex side of the deformity.
- Close the osteotomy, ensuring broad cancellous contact.
- Internal fixation with a plate and screws is highly effective here and can be used in conjunction with autogenous iliac bone grafts to stimulate rapid union.
Closure and Postoperative Care
Meticulous soft tissue handling is critical during closure. Close the wound in anatomical layers. If an external fixator has been used, apply a sterile, bulky compressive dressing around the pin sites. If internal fixation was utilized, apply a well-padded cast from the tibial tuberosity to the toes to protect the soft tissues and the osteotomy.
Rehabilitation Protocol
- 0 to 2 Weeks: The limb is elevated strictly. At 2 weeks, any cast is changed, the wound is inspected, and the sutures are removed.
- 2 to 6 Weeks: Weight bearing is strictly not permitted for 6 weeks to prevent catastrophic failure of the osteotomy or subsidence of the bone graft.
- 6 to 8 Weeks: If an external fixation device was utilized, it is typically removed at 6 to 8 weeks in the clinic or under light sedation, and a short-leg walking cast or a rigid fracture boot is applied.
- 8 to 16 Weeks: Weight bearing is progressed gradually as tolerated based on radiographic evidence of bridging callus. The cast or boot is removed when the osteotomies have completely healed (typically 12 to 16 weeks after surgery).
- Long-term: Aggressive rehabilitation of the lower extremity is begun by physical therapy, focusing on restoring tibiotalar range of motion, peroneal and tibial tendon strength, and proprioception.
Salvage Procedures: Arthrodesis for Malunited Fractures
While supramalleolar osteotomy is the gold standard for joint preservation, it is contraindicated in cases where the malunion has already resulted in severe, irreversible post-traumatic osteoarthritis of the tibiotalar joint. In these scenarios, realigning the limb will not relieve the patient's articular pain.
Arthrodesis is indicated as a primary procedure in malunited fractures of the ankle where the articular cartilage is destroyed.

FIGURE 58-12A: Preoperative radiograph demonstrating a severe malunion of a bimalleolar ankle fracture with a preexisting malunion of the distal tibia.

FIGURE 58-12B: Correction of the malunion was initially achieved; however, progressive post-traumatic arthritis developed, causing intractable pain and severe disability.
When performing an arthrodesis for a malunion, the surgeon must not only fuse the joint but also correct the underlying deformity to ensure a plantigrade foot. This often requires complex intra-articular osteotomies, aggressive debridement of sclerotic bone, and robust fixation, often utilizing compression clamps, crossed lag screws, or anterior/lateral plating systems.

FIGURE 58-12C: Anteroposterior radiograph following a tibiotalar arthrodesis performed using compression clamps to achieve rigid stability and correct alignment.

FIGURE 58-12D: Lateral radiograph of the successful tibiotalar arthrodesis. The ankle is now painless, stable, and functionally plantigrade.
💡 Clinical Pearl: The Transition to Arthrodesis
Always counsel patients preoperatively that if intraoperative assessment reveals extensive full-thickness cartilage loss that was not fully appreciated on preoperative imaging, the surgical plan may need to be converted from a joint-sparing supramalleolar osteotomy to a tibiotalar arthrodesis. Informed consent for both procedures is mandatory.
By adhering to strict biomechanical principles, executing precise surgical techniques, and respecting the delicate soft tissue envelope of the distal tibia, orthopedic surgeons can successfully utilize the supramalleolar osteotomy to restore function, alleviate pain, and preserve the native ankle joint in the setting of complex malunions.
📚 Medical References
- Supramalleolar osteotomy for ankle valgus in myelomeningocele, J Pediatr Orthop 16:774, 1996.
- Abraham E, Verinder DGR, Sharrard WJW: The treatment of fl exion contracture of the knee in myelomeningocele, J Bone Joint Surg 59B:433, 1977.
- Allen BL, Ferguson RL: The operative treatment of myelomeningocele spinal deformity, Orthop Clin North Am 10:845, 1979.
- Altman R, Altman DA: Imaging of spinal dysraphism, AJNR Am J Neurol Radiol 8:533, 1987.
- American Academy of Orthopaedic Surgeons: Symposium on myelomeningocele, St Louis, 1972, Mosby. Aprin H, Kilfoyle RM: Extension contracture of the knees in patients with meningomyelocele, Clin Orthop Relat Res 144:260, 1979.
- Archibeck MJ, Smith JT, Carroll KL, et al: Surgical release of tethered spinal cord: survivorship analysis and orthopedic outcome, J Pediatr Orthop 17:773, 1997.
- Asher M, Olson J: Factors affecting the ambulatory status of patients with spina bifi da cystica, J Bone Joint Surg 65A:350, 1983.
- Banit DM, Iwinski HJ, Talwalkar V, et al: Posterior spinal fusion in paralytic scoliosis and myelomeningocele, J Pediatr Orthop 21:117, 2001.
- Banta JV, Becker G: The natural history of scoliosis in myelomeningocele, Orthop Trans 10:18, 1986.
- Banta JV, Park SM: Improvement in pulmonary function in patients having combined anterior and posterior spine fusion for myelomeningocele scoliosis, Spine 8:765, 1983.
- Banta JV, Sutherland DH, Wyatt M: Anterior tibial transfer to the os calcis with Achilles tenodesis for calcaneal deformity in myelomeningocele, J Pediatr Orthop 1:125, 1981.
- Barden GA, Meyer LC, Stelling FH III: Myelodysplastics: fate of those followed for 20 years or more, J Bone Joint Surg 57A:643, 1975.
- Baxter MP, D’Astous JL: Proximal femoral resection interposition arthroplasty: salvage hip surgery for the severely disabled child with cerebral palsy, J Pediatr Orthop 6:681, 1986.
- Bazih J, Gross RH: Hip surgery in the lumbar level myelomeningocele patient, J Pediatr Orthop 1:405, 1981.
- Beals RK: The treatment of ankle valgus by surface epiphysiodesis, Clin Orthop Relat Res 266:162, 1991.
- Beaty JH, Canale ST: Orthopaedic aspects of myelomeningocele, J Bone Joint Surg 72A:626, 1990.
- Benton LJ, Salvati EA, Root L: Reconstructive surgery in the myelomeningocele hip, Clin Orthop Relat Res 110:261, 1975.
- Birch R: Surgery of the knee in children with spina bifi da, Dev Med Child Neurol Suppl 37:111, 1976.
- Birmingham PK, Dsida RM, Grayhack JJ, et al: Do latex precautions in children with myelodysplasia reduce intraoperative allergic reactions? J Pediatr Orthop 16:799, 1996.
- Bliss HG, Menelaus MB: The results of transfer of the tibialis anterior to the heel in patients who have a myelomeningocele, J Bone Joint Surg 68A:1258, 1986.
- Blount WP: Unequal leg length in children, Surg Clin North Am 38:1107, 1958.
- Brinker MR, Rosenfeld SR, Feiwell E, et al: Myelomeningocele at the sacral level, J Bone Joint Surg 76A:1293, 1994.
- Brock DJH, Sutcliffe RG: Alpha-fetoprotein in the antenatal diagnosis of anencephaly and spina bifi da, Lancet 2:197, 1972.
- Brocklehurst G, ed: Spina bifi da for the clinician, Philadelphia, 1976, Lippincott. Broughton NS, Brougham DI, Cole WG, et al: Reliability of radiological measurements in the assessment of the child’s hip, J Bone Joint Surg 71B:6, 1989.
- Broughton NS, Graham G, Menelaus MB: The high incidence of foot deformity in patients with high-level spina bifi da, J Bone Joint Surg 76B:548, 1994.
- Broughton NS, Menelaus MB: General considerations. In Broughton NS, Menelaus MB, eds: Menelaus’ orthopaedic management of spina bifi da, 3rd ed, Philadelphia, 1998, Saunders. Broughton NS, Menelaus MB, Cole WG, et al: The natural history of hip deformity in myelomeningocele, J Bone Joint Surg 75B:760, 1993.
- Bunch WH, Cass AS, Bensman AS, et al: Modern management of myelomeningocele, St Louis, 1972, Warren H Green. Bunch WH, Hakala MW: Iliopsoas transfers in children with myelomeningocele, J Bone Joint Surg 66A:224, 1984.
- Bunch WH, Scarff TB, Dvonch VM: Progressive loss in myelomeningocele patients, Orthop Trans 7:185, 1983.
- Burkus JK, Moore DW, Raycroft JF: Valgus deformity of the ankle in myelodysplastic patients: correction by stapling of the medial part of the distal tibial physis, J Bone Joint Surg 65A:1157, 1983.
- Canale G, Scarsi M, Mastragostino S: Hip deformity and dislocation in spina bifi da, Ital J Orthop Traumatol 18:155, 1992.
- Canale ST, Hammond NL III, Cotler JM, et al: Pelvic displacement osteotomy for
You Might Also Like

