Comprehensive Surgical Management of Sports Injuries of the Ankle
Key Takeaway
Sports injuries of the ankle encompass a complex spectrum of ligamentous disruptions, syndesmotic injuries, and osteochondral lesions. Mastery of ankle biomechanics, precise clinical stress testing, and advanced imaging are paramount. This guide details the surgical anatomy of the lateral, medial, and syndesmotic complexes, outlining evidence-based operative interventions and postoperative protocols for acute ruptures and chronic instability in high-demand athletes.
INTRODUCTION TO ANKLE SPORTS INJURIES
Sports-related injuries to the ankle represent one of the most frequently encountered pathologies in both acute trauma and chronic orthopedic sports medicine. The ankle joint is a highly congruent, dynamically stabilized hinge joint that must withstand tremendous axial, sheer, and rotational forces during athletic activity. While many acute ligamentous sprains resolve with functional rehabilitation, high-energy trauma or repetitive microtrauma in the elite athlete often leads to chronic instability, syndesmotic disruption, or occult intra-articular derangements.
The successful management of these injuries requires a profound understanding of the intricate pathoanatomy, precise clinical and radiographic evaluation, and meticulous surgical execution. This comprehensive guide details the evidence-based approach to the diagnosis and operative management of acute and chronic sports injuries of the ankle.
SURGICAL ANATOMY AND BIOMECHANICS
A rigorous understanding of ankle ligamentous anatomy is the foundation of successful surgical reconstruction. The stabilizing structures of the ankle are divided into the distal tibiofibular syndesmosis, the medial collateral (deltoid) ligament complex, and the lateral ligamentous complex.
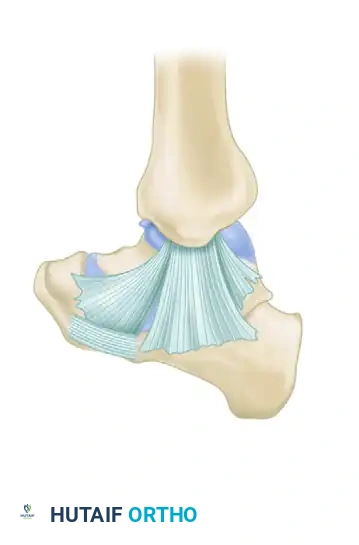
The Distal Tibiofibular Syndesmosis
Maintaining the critical relationship between the distal tibia and fibula is the syndesmosis, a complex consisting of four distinct components. This ligamentous complex is not merely a static tether; with dorsiflexion of the ankle, the syndesmosis allows the fibula to translate laterally, rotate externally, and migrate proximally. Furthermore, it allows the fibula to share approximately 16% of the axial load transmitted across the lower extremity.
- Anterior Inferior Tibiofibular Ligament (AITFL): Attaches medially to the anterior tibial tubercle (Chaput tubercle), extends inferiorly and laterally, and inserts on the anterior fibula (Wagstaffe tubercle).
> Clinical Pearl: Occasionally, an accessory distal slip of the AITFL, known as Baxter’s ligament, inserts distally on the fibula. Hypertrophy or scarring of this slip is a well-documented cause of anterolateral soft-tissue impingement against the talus. - Posterior Inferior Tibiofibular Ligament (PITFL): The strongest component of the syndesmosis. It runs in a similar oblique direction as the AITFL, connecting the posterior tibial tubercle (Volkmann tubercle) to the posterior fibula.
- Inferior Transverse Tibiofibular Ligament (ITFL): Situated deep and inferior to the PITFL. On its anterior surface, the ITFL forms a specialized labrum that articulates with the posterolateral talus, effectively deepening the tibiotalar joint and providing critical posterior stability.
- Interosseous Tibiofibular Ligament: Attaches to the contiguous rough surfaces of the tibia and fibula. It is continuous with the interosseous membrane proximally (note: the interosseous membrane itself is not considered part of the true syndesmosis).
The Medial Collateral (Deltoid) Ligament Complex
The deltoid ligament is a robust, multifascicular structure that provides the primary restraint against valgus tilting and anterolateral translation of the talus. It is anatomically divided into superficial and deep components.
Superficial Deltoid Ligament:
The superficial deltoid originates from the anterior colliculus of the medial malleolus and spans multiple joints. It comprises the tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments. The tibiocalcaneal component blends seamlessly with the spring ligament complex, providing vital support to the medial longitudinal arch.
Deep Deltoid Ligament:
The deep deltoid is the primary medial stabilizer of the ankle mortise. It originates from the intercollicular groove and posterior colliculus, inserting directly onto the medial surface of the talus. It consists of the anterior and posterior deep tibiotalar ligaments.

Surgical Warning: In the setting of a supination-eversion (Lauge-Hansen) fibular fracture with a reduced mortise, deltoid incompetence may be masked. External rotation stress radiographs are mandatory to accurately diagnose deep deltoid rupture, as direct clinical examination (tenderness, ecchymosis) is a notoriously poor predictor of medial instability.
The Lateral Ligamentous Complex
The lateral ligamentous complex is the most frequently injured structure in athletic trauma, typically failing under inversion and internal rotation forces.
- Anterior Talofibular Ligament (ATFL): Originates from the anterior margin of the lateral malleolus and courses anteriorly to the neck of the talus, blending with the anterolateral joint capsule. It is the weakest of the lateral ligaments and the most frequently injured. Its primary biomechanical function is to resist anterior translation of the talus when the ankle is in a relatively neutral or plantarflexed position.
- Calcaneofibular Ligament (CFL): A robust, cord-like structure measuring 20 to 25 mm in length, 6 to 8 mm in width, and 3 to 4 mm in thickness. It originates from the tip of the lateral malleolus, extends posteroinferiorly deep to the peroneal tendons, and inserts on the lateral surface of the calcaneus. Notably, it is the only lateral ligament that is strictly extracapsular.
- Posterior Talofibular Ligament (PTFL): The strongest of the lateral ligaments. It measures approximately 30 mm long, 5 mm wide, and 5 to 8 mm thick. It attaches anteriorly to the digital fossa of the fibula and courses horizontally to the lateral tubercle on the posterior aspect of the talus.

The Bifurcate Ligament
While not a primary stabilizer of the tibiotalar joint, the bifurcate ligament is frequently injured in conjunction with lateral ankle sprains. It originates from the anterior process of the calcaneus and divides in a Y-shaped configuration to insert on the dorsomedial aspect of the cuboid and the dorsolateral aspect of the navicular.
Pitfall: Injury to the bifurcate ligament is often misdiagnosed as an isolated ATFL tear due to the proximity of the pain and swelling. Point tenderness over the anterior process of the calcaneus should raise high clinical suspicion for a bifurcate ligament rupture or avulsion fracture.
CLINICAL EVALUATION AND DIAGNOSTICS
Physical Examination and Stress Testing
Accurate diagnosis dictates the treatment algorithm. The clinical examination must systematically evaluate for localized tenderness, effusion, and mechanical instability.
- Anteroposterior Stress Test (Anterior Drawer Sign): Evaluates the integrity of the ATFL. With the tibia stabilized and the ankle in 10 to 15 degrees of plantarflexion, an anterior force is applied to the heel. Excessive anterior translation or a "clunk" indicates ATFL incompetence.
- Inversion Stress Test (Talar Tilt): Evaluates the combined integrity of the ATFL and CFL. Inversion stress is best applied with the ankle slightly plantarflexed.
- Talar tilt of ~15 degrees: Indicates isolated rupture of the ATFL.
- Talar tilt of 15 to 30 degrees: Indicates combined rupture of the ATFL and CFL.
- Talar tilt > 30 degrees: Highly suggestive of complete disruption of all three lateral ligaments (ATFL, CFL, PTFL).
- Eversion Stress Test: Evaluates the deltoid ligament. Eversion stress radiographs of normal ankles typically reveal little to no talar shift or tilt. If the lateral ligaments are completely disrupted, or in the presence of a lateral malleolus fracture, the talus will shift laterally with eversion stress, confirming medial incompetence.
Advanced Imaging
Magnetic Resonance Imaging (MRI):
While acute ankle sprains rarely require immediate MRI, advanced imaging is indispensable for high-demand athletes, patients with chronic instability, or those with suspected intra-articular pathology. MRI provides unparalleled visualization of:
* Ligamentous continuity and chronicity of tears (thickened, heterogeneous ligaments vs. acute fluid-filled gaps).
* Osteochondral lesions of the talus (OLT).
* Peroneal tendon pathology (tears, subluxation, tenosynovitis).
* Syndesmotic integrity.
CLASSIFICATION OF ANKLE LIGAMENT INJURIES
The Clanton and McGarvey classification system provides a highly pragmatic, treatment-oriented framework for managing ankle ligament injuries, particularly in the athletic population.
Clanton and McGarvey Classification (Box 89-1)
- Type I: Stable ankle to clinical testing (with anesthesia, if necessary).
- Treatment: Symptomatic and functional rehabilitation.
- Type II: Unstable ankle with a positive anterior drawer test, positive talar tilt test, or both.
- Group 1: Nonathlete or older patient.
- Treatment: Functional treatment (bracing, physical therapy).
- Group 2: Athlete or high-demand patient.
- Type A: Negative radiographic stress test.
- Treatment: Functional treatment.
- Type B: Positive tibiotalar radiographic stress test.
- Treatment: Surgical repair.
- Type C: Subtalar instability.
- Treatment: Functional treatment (initially), with potential for delayed reconstruction if symptomatic.
- Type A: Negative radiographic stress test.
- Group 1: Nonathlete or older patient.
SURGICAL MANAGEMENT OF ACUTE LIGAMENTOUS INJURIES
While the vast majority of acute lateral ankle sprains are managed non-operatively with early functional rehabilitation, acute surgical intervention is indicated in specific scenarios: elite athletes with severe multi-ligamentous disruptions (Type II, Group 2B), massive syndesmotic tears with mortise widening, or acute deltoid ruptures associated with syndesmotic failure.
Repair of Acute Rupture of the Distal Tibiofibular Syndesmosis
Failure to anatomically reduce and stabilize the syndesmosis leads to rapid, catastrophic post-traumatic arthritis.
Surgical Technique:
1. Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg to neutral.
2. Approach: If associated with a fibular fracture, the standard lateral approach is utilized. For isolated syndesmotic injuries, a direct anterolateral approach over the distal tibiofibular joint allows direct visualization of the AITFL and the incisura fibularis.
3. Reduction: The joint is debrided of interposed hematoma or torn ligamentous stumps. The fibula is reduced into the incisura using a large reduction clamp. Crucial Step: The clamp must be placed in the neutral anatomical axis to avoid over-compression or malrotation of the fibula.
4. Fixation: Fixation can be achieved via trans-syndesmotic screws (typically two 3.5mm or 4.5mm cortical screws placed 2-3 cm proximal to the joint line, engaging 3 or 4 cortices) or dynamic suture-button constructs. Suture-button constructs allow for physiologic micromotion and eliminate the need for routine hardware removal.
5. Postoperative Protocol: Non-weight-bearing in a cast or rigid boot for 4 to 6 weeks, followed by progressive weight-bearing and physical therapy.
Repair of Acute Rupture of the Deltoid Ligament
Isolated acute ruptures of the deltoid ligament are exceedingly rare; they are almost universally associated with syndesmotic injuries or lateral malleolar fractures.
Surgical Technique:
1. Indications: Medial clear space widening that does not reduce with lateral/syndesmotic fixation, or interposition of the deltoid ligament blocking anatomic reduction of the talus.
2. Approach: A medial longitudinal incision centered over the medial malleolus.
3. Repair: The superficial and deep components are identified. Avulsions from the medial malleolus are repaired using suture anchors. Midsubstance tears are repaired with heavy non-absorbable sutures using a Krackow or locking core stitch technique.
4. Augmentation: In cases of severe tissue attenuation, augmentation with a local periosteal flap or allograft may be considered.
Repair of Acute Rupture of the Lateral Ligaments
Acute repair of the lateral ligaments is reserved for high-caliber athletes where the risk of chronic instability threatens their career, or in cases of massive soft-tissue avulsion (e.g., open dislocations).
Surgical Technique:
1. Approach: Anterolateral curvilinear incision, taking care to protect the superficial peroneal nerve dorsally and the sural nerve plantarly.
2. Identification: The extensor retinaculum is incised, and the joint capsule is opened. The torn ends of the ATFL and CFL are identified.
3. Anatomic Repair: If avulsed from the fibula, suture anchors are placed into the anatomic footprint at the anterior and distal tip of the lateral malleolus. The ligaments are tied with the ankle held in neutral dorsiflexion and slight eversion to restore appropriate resting tension.
MANAGEMENT OF CHRONIC INSTABILITY AFTER INJURY
Chronic lateral ankle instability is characterized by recurrent giving way, persistent pain, and apprehension. When conservative measures (peroneal strengthening, proprioceptive training, bracing) fail, surgical reconstruction is highly successful.
Lateral Repair of Chronic Instability (Modified Broström-Gould Technique)
The anatomic repair of the native ligaments (Broström) augmented by the inferior extensor retinaculum (Gould modification) remains the gold standard for chronic lateral instability.
Surgical Steps:
1. Positioning: Supine with a bump under the ipsilateral hip. A thigh tourniquet is applied.
2. Incision: A 4 to 5 cm curvilinear incision is made just anterior and distal to the lateral malleolus.
3. Dissection: The subcutaneous tissue is bluntly dissected. The superficial peroneal nerve branches must be identified and protected. The inferior extensor retinaculum is identified and mobilized.
4. Capsulotomy and Debridement: A vertical incision is made through the capsule and ATFL remnant, leaving a small cuff on the fibula. The joint is inspected for osteochondral lesions or loose bodies (often addressed via pre-reconstruction arthroscopy).
5. Ligament Imbrication/Repair: The fibular footprint is decorticated to bleeding bone. Suture anchors (typically 2.5mm to 3.0mm) are placed into the fibula. The sutures are passed through the ATFL and CFL remnants in a pants-over-vest or horizontal mattress fashion.
6. Tensioning: The sutures are tied with the ankle in neutral dorsiflexion and slight eversion.
7. Gould Modification: The mobilized lateral edge of the inferior extensor retinaculum is pulled proximally and posteriorly over the repaired ligaments and sutured to the fibular periosteum. This reinforces the repair and helps limit inversion.
8. Postoperative Protocol:
* Weeks 0-2: Non-weight-bearing in a short leg cast or rigid splint in neutral.
* Weeks 2-6: Transition to a CAM boot, begin protected weight-bearing. Initiate active dorsiflexion/plantarflexion. Avoid inversion.
* Weeks 6-12: Transition to a functional lace-up brace. Begin proprioceptive and peroneal strengthening.
* Months 3-4: Return to sport-specific activities.
ASSOCIATED INTRA-ARTICULAR AND OCCULT LESIONS
Chronic instability and acute trauma are frequently accompanied by secondary pathologies that must be addressed concurrently to ensure a successful outcome.
Osteochondral Lesions of the Talus (OLT)
Also known as osteochondral fractures or transchondral dome fractures, OLTs are a frequent cause of deep, aching ankle pain following a sprain. They occur due to the impaction of the talar dome against the tibial plafond during the injury mechanism.
* Anterolateral Lesions: Typically shallow, wafer-shaped, and caused by inversion/dorsiflexion trauma.
* Posteromedial Lesions: Typically deeper, cup-shaped, and caused by inversion/plantarflexion trauma.
* Arthroscopic Treatment: Symptomatic lesions failing conservative care are treated arthroscopically. Techniques include debridement and bone marrow stimulation (microfracture) for lesions < 1.5 cm², or osteochondral autograft transfer (OATS)/matrix-induced autologous chondrocyte implantation (MACI) for larger, cystic lesions.
Sinus Tarsi Syndrome
Sinus tarsi syndrome presents as localized pain and tenderness over the lateral aspect of the hindfoot, specifically in the sinus tarsi. It is often a sequela of an inversion sprain that damages the interosseous talocalcaneal ligament and the cervical ligament, leading to subtalar microinstability and subsequent synovitis.
* Diagnosis: Pain relief following a diagnostic injection of local anesthetic into the sinus tarsi confirms the diagnosis.
* Treatment: Initial management includes corticosteroid injections and orthotics. Refractory cases may require arthroscopic or open debridement of the sinus tarsi contents and reconstruction of the subtalar ligaments.
Peroneal Tendon Subluxation and Dislocation
Forced dorsiflexion with sudden reflex contraction of the peroneal muscles can rupture the superior peroneal retinaculum, leading to anterior subluxation or dislocation of the peroneal tendons over the lateral malleolus.
* Diagnosis: The patient often reports a snapping sensation. Subluxation can be reproduced by having the patient actively evert and dorsiflex the ankle against resistance.
* Surgical Management: Acute injuries may be repaired directly. Chronic cases require deepening of the retromalleolar fibular groove, repair/reconstruction of the superior peroneal retinaculum, or tissue transfer procedures to stabilize the tendons.
CONCLUSION
The surgical management of sports injuries of the ankle demands a comprehensive understanding of the complex interplay between the osseous mortise and its ligamentous restraints. From the critical load-sharing mechanics of the syndesmosis to the precise anatomic footprints of the lateral complex, surgical interventions must aim to restore native kinematics. By adhering to rigorous diagnostic protocols, utilizing advanced imaging judiciously, and executing meticulous, evidence-based surgical techniques, the orthopedic surgeon can reliably return high-demand athletes to their pre-injury level of function.
You Might Also Like
