Operative Management of Flexor Hallucis Longus and Flexor Digitorum Longus Tendon Injuries
Key Takeaway
The repair of a flexor hallucis longus (FHL) tear requires meticulous surgical technique to restore the critical push-off biomechanics of the hallux. Retrieval of the retracted proximal stump is facilitated by plantarflexing the ankle and tracking the hematoma. Due to the anatomical tethering at the Master Knot of Henry, the FHL rarely retracts proximal to the navicular. End-to-end tenorrhaphy using a nonabsorbable suture ensures robust fixation for postoperative rehabilitation.
INTRODUCTION AND BIOMECHANICAL SIGNIFICANCE
The flexor hallucis longus (FHL) is a powerful plantarflexor of the hallux and a critical dynamic stabilizer of the medial longitudinal arch. Often referred to as the "Achilles of the foot," the FHL plays an indispensable role during the push-off phase of the gait cycle. It generates significant force to propel the body forward while stabilizing the first metatarsophalangeal (MTP) joint against the ground reaction forces.
Lacerations or traumatic ruptures of the FHL tendon result in a profound loss of active interphalangeal (IP) joint flexion and a weakened push-off, leading to an apropulsive gait and secondary transfer metatarsalgia. Consequently, acute tears of the FHL generally warrant prompt surgical repair to restore normal foot biomechanics.
Conversely, injuries to the flexor digitorum longus (FDL) present a different clinical paradigm. Because of the complex interplay of the intrinsic foot musculature—specifically the lumbricals and the quadratus plantae—isolated injuries to the FDL often result in minimal functional deficit. The decision to repair the FDL is highly dependent on the anatomical zone of injury and the presence of concomitant structural damage.
This comprehensive guide details the surgical anatomy, indications, operative techniques, and postoperative rehabilitation protocols for managing injuries to both the FHL and FDL tendons.
SURGICAL ANATOMY
A profound understanding of the plantar anatomy is required to safely navigate the surgical repair of these tendons, particularly given their proximity to the medial and lateral plantar neurovascular bundles.
The Flexor Hallucis Longus (FHL)
The FHL muscle belly originates from the posterior aspect of the fibula and the interosseous membrane. The tendon forms proximal to the ankle joint and descends through a series of fibro-osseous tunnels:
1. Zone 1 (Retromalleolar): The tendon passes posterior to the medial malleolus, lying lateral to the flexor digitorum longus (FDL) and the posterior tibial neurovascular bundle.
2. Zone 2 (Sustentaculum Tali): It courses under the sustentaculum tali, where it is tightly constrained within a fibro-osseous sheath.
3. Zone 3 (Plantar Midfoot): In the plantar aspect of the foot, the FHL crosses superior (dorsal) to the FDL tendon. This crossing point is known as the Master Knot of Henry (chiasma plantare). At this junction, there are often strong tendinous slips connecting the FHL and FDL.
4. Zone 4 (First Metatarsal and Sesamoids): The tendon passes between the medial and lateral heads of the flexor hallucis brevis (FHB) and traverses the interval between the medial and lateral sesamoids.
5. Zone 5 (Insertion): The tendon inserts onto the plantar base of the distal phalanx of the hallux.
The Flexor Digitorum Longus (FDL)
The FDL originates from the posterior tibia, courses posterior to the medial malleolus (medial to the neurovascular bundle), and enters the plantar foot. After crossing the FHL at the Master Knot of Henry, it receives the insertion of the quadratus plantae muscle, which aligns the pull of the FDL tendons along the long axis of the lesser toes. It then divides into four slips that insert onto the bases of the distal phalanges of the second through fifth toes.
Clinical Pearl: The tendinous interconnections at the Master Knot of Henry serve as a critical anatomical tether. In the event of a distal FHL laceration, the proximal tendon stump will rarely retract proximal to the navicular bone due to this cross-connection with the FDL.
INDICATIONS AND CONTRAINDICATIONS
Flexor Hallucis Longus (FHL)
Indications for Repair:
* Acute lacerations of the FHL tendon at any level (midfoot, forefoot, or digit).
* Traumatic closed ruptures (often occurring at the level of the sesamoids or the Master Knot of Henry in athletes, such as dancers or gymnasts).
* Iatrogenic transection during forefoot reconstruction.
Contraindications:
* Chronic, neglected ruptures with severe muscle atrophy and fixed contractures (may require tendon transfer or IP joint arthrodesis instead).
* Severe soft tissue compromise or active plantar infection.
Flexor Digitorum Longus (FDL)
Indications for Repair:
* Deep plantar lacerations near the midfoot-hindfoot junction (proximal to the junction of the quadratus plantae and FDL) if the FHL is also lacerated, usually accompanied by concomitant medial or lateral plantar nerve injury. In these complex, multi-structure injuries, the FDL may be repaired alongside the primary structures to restore gross plantarflexion power.
Contraindications:
* Isolated injuries of the FDL in the toes or midfoot. Repair of an isolated FDL laceration is generally not indicated. The intrinsic muscles (lumbricals and interossei) provide sufficient flexion at the MTP joints, and the quadratus plantae assists in stabilizing the lesser digits. Attempting to repair the FDL within the narrow digital fibro-osseous sheaths frequently leads to severe adhesions, profound stiffness, and a rigid, non-functional toe that is more symptomatic than a toe with a neglected FDL tear.
PREOPERATIVE PREPARATION AND POSITIONING
- Anesthesia: General anesthesia or a regional block (spinal or popliteal sciatic nerve block) is preferred to ensure complete muscle relaxation, which is essential for retrieving retracted tendon stumps.
- Positioning: The patient is placed in the supine position. A bump may be placed under the ipsilateral hip to externally rotate the leg, providing optimal access to the medial and plantar aspects of the foot.
- Tourniquet: A thigh or calf tourniquet is applied and inflated to 250-300 mmHg after exsanguination to provide a bloodless surgical field.
- Equipment: Have tendon passers, fine hemostats, atraumatic tissue forceps, and appropriate nonabsorbable sutures (e.g., 2-0 or 3-0 Prolene, Ethibond, or FiberWire) available.
SURGICAL TECHNIQUE: REPAIR OF FLEXOR HALLUCIS TEAR
The primary challenge in repairing an FHL laceration is locating and retrieving the proximal stump, which is invariably pulled proximally by the resting tone of the muscle belly.
Step 1: Approach and Exposure
- Extend the traumatic laceration longitudinally, adhering to the principles of plantar incisions (avoiding weight-bearing prominences and crossing flexion creases at oblique angles).
- Carefully dissect through the plantar fat pad. Identify and protect the medial plantar nerve and its digital branches, which lie in close proximity to the FHL tendon in the forefoot.
- Identify the distal stump of the FHL tendon, which is usually easily found attached to the base of the distal phalanx or within the sesamoid apparatus.
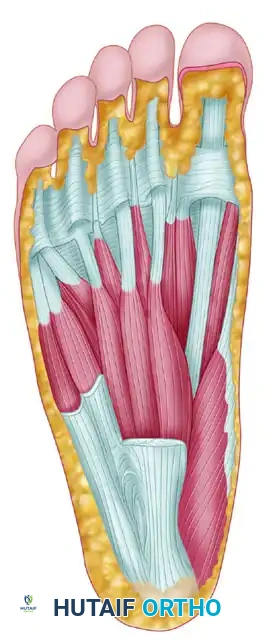
FIGURE 82-66: 1, Pulley of flexor hallucis longus at first metatarsophalangeal joint; 2, flexor hallucis longus; 3, lateral head of flexor hallucis brevis.
Step 2: Retrieval of the Proximal Stump
- Inspect the proximal aspect of the wound. Follow the proximal course of the retracted tendon, particularly utilizing any dark hematoma or organized scar tissue as a visual guide to direct the way.
- Place the ankle in maximal equinus (plantarflexion). This maneuver maximally relaxes the FHL muscle belly and advances the proximal stump distally.
- Use a smooth tendon passer or a fine, curved hemostat to probe proximally along the suspected anatomical path within the tendon sheath.
- Anatomical Limit of Retraction: The surgeon should be reassured that the tendon will not retract past the level of the navicular. This is due to the robust tethering provided by the cross-connections with the flexor digitorum longus at the Master Knot of Henry.
Surgical Warning: Do not blindly grasp deep into the plantar vault with heavy clamps, as this risks crushing the medial plantar nerve or artery. If the tendon cannot be retrieved with gentle probing, a separate small counter-incision may be made proximally over the medial midfoot to identify the tendon and pass it distally.
Step 3: Temporary Fixation
- Once the proximal tendon stump is located, grasp it gently with an atraumatic clamp and bring it into the primary wound.
- Maintain the ankle in a plantarflexed position to relieve tension.
- To prevent the tendon from retracting while you prepare for suturing, pass a straight Keith needle transversely through the plantar skin, directly through the substance of the FHL tendon, and out into the skin on the opposite side. This temporary transfixation acts as a "stay" and completely unloads the tendon ends, allowing for a meticulous, tension-free repair.
Step 4: Tenorrhaphy (Tendon Repair)
- Flex the MTP and IP joints of the hallux to approximate the distal stump to the proximal stump.
- Perform an end-to-end repair using a double right-angle stitch (or a modified Kessler/Krackow technique depending on tendon caliber).
- Utilize a 2-0 nonabsorbable suture material (e.g., braided polyester or ultra-high-molecular-weight polyethylene) swedged to a tapered, atraumatic needle.
- Avoid the "Accordion" Effect: When tying the core sutures, apply only enough tension to securely approximate the tendon ends. Do not overtighten or "accordion" the tendon. Bunching the tendon increases its cross-sectional area, creating a bulky repair site that will impinge within the fibro-osseous pulleys (especially between the sesamoids), leading to severe postoperative stiffness and loss of excursion.
- If necessary, a running epitendinous suture using 4-0 or 5-0 monofilament can be added to smooth the repair site and improve gliding.
Step 5: Closure and Immobilization
- Remove the temporary straight transfixation needle.
- Irrigate the wound copiously with sterile saline.
- Close the skin using 2-0 or 3-0 nylon. Simple interrupted sutures are generally desirable for plantar skin. However, vertical mattress sutures are highly acceptable and recommended if the skin edges are offset or under mild tension, as they provide superior eversion of the thick plantar epidermis.
- Apply a sterile, non-adherent dressing followed by a bulky soft tissue wrap.
- Apply a short-leg cast (or rigid posterior splint). The ankle must be immobilized in mild equinus (approximately 15-20 degrees of plantarflexion), and the hallux should be held in a neutral position. The cast or splint must extend distal to the toes to protect the repair from accidental dorsiflexion.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the healing tenorrhaphy while gradually introducing stress to promote organized collagen remodeling and prevent restrictive adhesions.
Phase 1: Protection (Weeks 0 to 3)
- The patient is kept strictly non-weight-bearing (NWB) for the first 3 weeks.
- The limb remains immobilized in the initial short-leg cast with the ankle in mild equinus and the toes protected.
- Elevation and strict adherence to NWB status are critical to prevent wound dehiscence and early repair failure.
Phase 2: Transition to Weight-Bearing (Weeks 3 to 6)
- At the 3-week mark, the initial cast is removed.
- Skin sutures are removed at this time.
- The foot is gently brought up to a neutral position at the ankle (0 degrees of dorsiflexion/plantarflexion).
- A new short-leg cast (or a rigid pneumatic walker boot locked in neutral) is applied. This immobilization must still extend past the toes to prevent passive dorsiflexion of the hallux.
- The patient is allowed to begin weight-bearing to tolerance (WBAT) in the cast.
Phase 3: Mobilization (Week 6 and Beyond)
- At 6 weeks postoperatively, the short-leg walking cast is discontinued.
- Active toe flexion is initiated. To maximize tendon excursion and break up early adhesions, targeted blocking exercises are employed:
- The examiner or physical therapist manually blocks the MTP joint in extension while the patient actively flexes the IP joint.
- The IP joint is then blocked while the patient actively flexes the MTP joint.
- Passive dorsiflexion stretching is introduced gradually to restore full extension of the first ray.
Prognostic Pearl: The anatomical location of the repair dictates the functional outcome of the IP joint. If the FHL repair is performed 2 cm or more proximal to the metatarsophalangeal joint, the tendon repair site remains proximal to the narrowest portion of the fibro-osseous sheath during excursion. In these cases, the interphalangeal joint should recover excellent independent active flexion. Repairs occurring directly within the sesamoid apparatus have a higher risk of localized scarring and reduced IP joint motion.
MANAGEMENT OF FLEXOR DIGITORUM LONGUS (FDL) INJURIES
As previously stated, the surgical management of FDL injuries is highly conservative compared to the FHL.
Isolated Distal Injuries
Repair of an isolated injury of the flexor digitorum longus in the toes or in the midfoot is not indicated. The functional deficit is negligible due to the compensatory actions of the intrinsic musculature. Surgical intervention in the lesser toes risks creating a fixed flexion contracture or a rigid, painful digit due to dense scar formation within the tight flexor sheaths. These patients are managed with local wound care, buddy taping, and early mobilization.
Complex Proximal Injuries
Surgical repair of the FDL is reserved for severe, deep plantar lacerations occurring near the midfoot-hindfoot junction. Specifically, if a laceration occurs proximal to the junction of the quadratus plantae and the FDL, and is accompanied by a laceration of the FHL and/or the medial or lateral plantar nerves, a comprehensive repair is indicated.
In these catastrophic injuries, the goal is to restore gross plantarflexion power to the forefoot and re-establish neural continuity. The FDL stumps are identified, and a standard core suture repair is performed concurrently with the FHL tenorrhaphy and epineural nerve repairs. Postoperative management follows the FHL protocol, prioritizing the protection of the FHL and nerve repairs.
COMPLICATIONS AND PITFALLS
- Tendon Adhesions: The most common complication following FHL repair. Adhesions limit tendon excursion, resulting in a lack of active IP joint flexion and a rigid hallux. Meticulous handling of the tendon, avoiding the "accordion" effect, and strict adherence to the 6-week mobilization protocol minimize this risk.
- Re-rupture: Usually occurs due to premature weight-bearing, accidental forced dorsiflexion, or poor suture technique. Re-rupture requires revision surgery, often necessitating a tendon graft if the ends have retracted and scarred.
- Nerve Injury: The medial plantar nerve is highly vulnerable during the retrieval of the proximal FHL stump. Iatrogenic injury can lead to painful neuromas and loss of plantar sensation.
- Infection and Wound Dehiscence: Plantar incisions are prone to delayed healing. Ensuring a tension-free skin closure with vertical mattress sutures and maintaining strict non-weight-bearing for the first 3 weeks are essential preventative measures.
CONCLUSION
The successful repair of a flexor hallucis longus tear requires a thorough understanding of plantar anatomy, precise surgical execution, and a disciplined postoperative rehabilitation protocol. By utilizing anatomical landmarks such as the Master Knot of Henry, employing temporary transfixation techniques to eliminate tension, and performing a low-profile tenorrhaphy, the orthopedic surgeon can reliably restore the critical push-off power of the first ray. Conversely, recognizing the indications for non-operative management of isolated FDL injuries prevents unnecessary surgical morbidity and optimizes patient outcomes.
You Might Also Like
