Operative Management of Intractable Interdigital and Plantar Corns
Key Takeaway
Intractable interdigital corns (heloma molle) and intractable plantar keratosis (IPK) often require surgical intervention when conservative measures fail. Partial syndactylization effectively addresses fourth web space lesions by resecting opposing bony prominences and fusing the web space. For IPK, careful radiographic evaluation dictates the approach, ranging from metatarsophalangeal arthroplasty for localized lesions to dorsiflexion or shortening osteotomies for diffuse callosities caused by an abnormal metatarsal parabola.
INTRODUCTION AND PATHOMECHANICS
Hyperkeratotic lesions of the foot, specifically intractable interdigital corns (heloma molle) and intractable plantar keratosis (IPK), represent a significant source of morbidity, pain, and altered gait mechanics in the adult population. These lesions are not merely dermatological anomalies; they are the cutaneous manifestations of underlying osseous pathology, altered foot biomechanics, and abnormal pressure distribution during the stance phase of gait.
An interdigital corn, most frequently located in the fourth web space, arises from the chronic friction and compression between the lateral condyle of the proximal phalanx of the fourth toe and the medial condyle of the proximal or middle phalanx of the fifth toe. The confined space of modern footwear exacerbates this "kissing" lesion, leading to a painful, macerated, and occasionally ulcerated hyperkeratosis.
Conversely, an intractable plantar keratosis (IPK) is a discrete, focused callus located beneath a metatarsal head. It is driven by localized mechanical overload. The etiology is multifactorial, often involving a prominent or plantarflexed metatarsal head, an abnormally long metatarsal (disrupting the normal metatarsal parabola), or retrograde buckling of the digit due to a hammer toe or claw toe deformity.
💡 Clinical Pearl
A plantar corn can usually be made asymptomatic by conservative care. Patient education and physician assiduity are essential for non-operative methods to succeed. Surgery should only be entertained after a lengthy and exhaustive course of conservative management has failed.
PREOPERATIVE EVALUATION AND CONSERVATIVE MANAGEMENT
Clinical Assessment
A meticulous physical examination is paramount. The surgeon must differentiate between a diffuse callosity and a discrete IPK.
* Interdigital Lesions: Inspect the web spaces for maceration, sinus tracts, or secondary fungal/bacterial infections. Palpate the opposing phalangeal condyles to identify the exact bony prominences responsible for the friction.
* Plantar Lesions: Palpate the plantar aspect of the metatarsal heads. Assess the mobility of the metatarsophalangeal (MTP) joints and the presence of associated lesser toe deformities. A localized IPK will often have a deep, nucleated center directly beneath a specific metatarsal condyle, whereas a diffuse callus suggests a broader biomechanical fault, such as a rigid equinus or a globally plantarflexed ray.
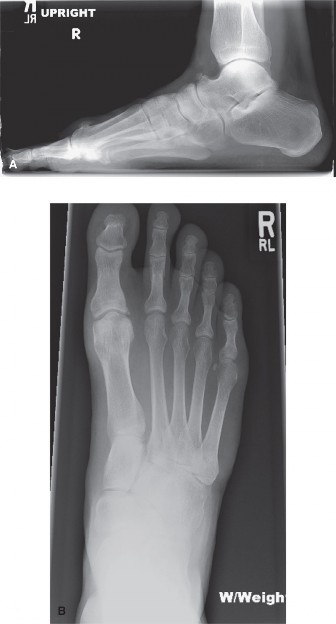
Radiographic Evaluation
Weight-bearing anteroposterior (AP), lateral, and sesamoid axial radiographs are mandatory.
* Evaluate the metatarsal parabola on the AP view to identify an abnormally long metatarsal.
* Assess the lateral view for a plantarflexed metatarsal relative to the adjacent rays.
* Examine the phalangeal heads and bases for hypertrophic condyles or osteophytes contributing to interdigital impingement.
Conservative Protocols
Regardless of the ultimate procedure chosen, recurrence or transfer of the lesion occurs in 10% to 15% of patients, emphasizing the absolute necessity of exhausting all conservative measures before proceeding to surgery.
1. Footwear Modification: Wide toe-box shoes to relieve medial-lateral compression.
2. Orthoses and Padding: Metatarsal pads placed proximal to the symptomatic metatarsal head to offload pressure. Custom orthotics with relief accommodations.
3. Local Care: Routine paring/shaving of the hyperkeratotic tissue, combined with lamb’s wool or silicone toe spacers for interdigital lesions.
PARTIAL SYNDACTYLIZATION FOR INTRACTABLE INTERDIGITAL CORN
When conservative measures fail to relieve a painful heloma molle, particularly in the fourth web space, partial syndactylization combined with targeted ostectomy provides a definitive, biomechanically sound solution. By resecting the offending bony prominences and fusing the web space, the procedure eliminates the friction interface entirely.
Indications
- Chronic, painful interdigital corn (heloma molle) refractory to conservative care.
- Recurrent ulceration of the web space without active deep infection.
- "Kissing" osteophytes or prominent condyles of the 4th and 5th toes confirmed on radiographs.
Contraindications
- Severe peripheral arterial disease (vascular compromise).
- Active, untreated web space infection or cellulitis.
- Inadequate skin envelope for tension-free closure.
Surgical Technique: Step-by-Step
1. Anesthesia and Positioning
The procedure is typically performed under a regional ankle block or local digital block with monitored anesthesia care. The patient is positioned supine. A calf or ankle tourniquet may be utilized to ensure a bloodless surgical field, though careful exsanguination is required to avoid tissue damage.
2. Incision Design
* Make a dorsal longitudinal incision centered over the affected interdigital space (usually the 4th web space).
* Extend this incision proximally to the level of the metatarsal heads and distally to the plantar portion of the interdigital space.
* Extend the two distal limbs of the incision into the adjacent sides of the plantar third of the opposing toes (the medial aspect of the 5th toe and the lateral aspect of the 4th toe).
3. Bony Resection (Ostectomy)
The success of the procedure relies on the adequate removal of the underlying bony prominences.
* Deepen the dissection to expose the proximal phalanges of the involved toes. Protect the dorsal and plantar neurovascular bundles.
* Fourth Toe: Identify the base of the proximal phalanx. Using a microsaw or a sharp rongeur, resect the lateral flare of the base of the proximal phalanx of the fourth toe.
* Fifth Toe: Identify the head of the proximal phalanx. Resect the medial portion of the head of the proximal phalanx of the fifth toe.
* Smooth all resected bony edges with a rasp to ensure no sharp spicules remain that could cause recurrent internal pressure.
⚠️ Surgical Warning
Do not resect the entire phalangeal head or base, as this will lead to profound instability of the digit. Only the prominent, offending condylar flares should be excised.
4. Soft Tissue Management and Closure
* Begin wound closure proximally and extend distally. Suture the dorsal limbs of the incision together using non-absorbable monofilament suture (e.g., 4-0 nylon).
* As the closure reaches the apex of the dorsal skin flaps, excise a small amount of redundant skin. If the web corn is present at this apex, it should be included in this elliptical excision to ensure healthy tissue approximation.
* Close the plantar limbs in a similar fashion, effectively creating a partial syndactylization (fusion of the skin) of the proximal aspect of the toes. This eliminates the deep web space where moisture and friction previously accumulated.
Postoperative Care for Syndactylization
- Dressings: A soft, mildly compressive dressing is applied immediately postoperatively.
- Medication: A broad-spectrum oral antibiotic is administered for 2 days prophylactically, given the historically high bacterial colonization of interdigital web spaces.
- Suture Removal: Sutures are left in place for a minimum of 2 weeks to ensure adequate healing of the syndactylized flaps.
- Immobilization: After suture removal, place lamb’s wool in the remaining distal interdigital space overlying the incision. The toes are then buddy-taped for an additional 2 weeks to protect the repair from sheer stress during ambulation. Weight-bearing is permitted in a stiff-soled postoperative shoe.
SURGICAL MANAGEMENT OF PLANTAR CORN (INTRACTABLE PLANTAR KERATOSIS)
The surgical approach to an IPK is dictated entirely by the specific pathoanatomy identified during the clinical and radiographic evaluation. The goal is to elevate or shorten the offending metatarsal to restore a harmonious weight-bearing distribution across the forefoot.
1. Arthroplasty of the Metatarsophalangeal Joint
For a small, highly localized intractable plantar keratosis situated directly beneath a prominent metatarsal condyle, an arthroplasty or condylectomy is usually preferred. This procedure directly addresses the focal osseous prominence without destabilizing the entire ray.
Surgical Approach:
* Make a dorsal longitudinal incision over the involved metatarsophalangeal joint (commonly the second or third MTP joint). The apex of the incision should be centered directly at the joint level.

FIGURE 83-35 Arthroplasty of metatarsophalangeal joint. A, Incision over second metatarsophalangeal joint with apex at joint level.
- Deepen the incision through the subcutaneous tissue, taking care to retract the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons laterally or medially.
- Perform a dorsal capsulotomy to expose the metatarsal head.
- To gain adequate exposure of the plantar aspect of the metatarsal head, the collateral ligaments must be sectioned. Once released, apply acute plantar flexion to the toe. This maneuver subluxates the joint and delivers the metatarsal head into the dorsal wound.
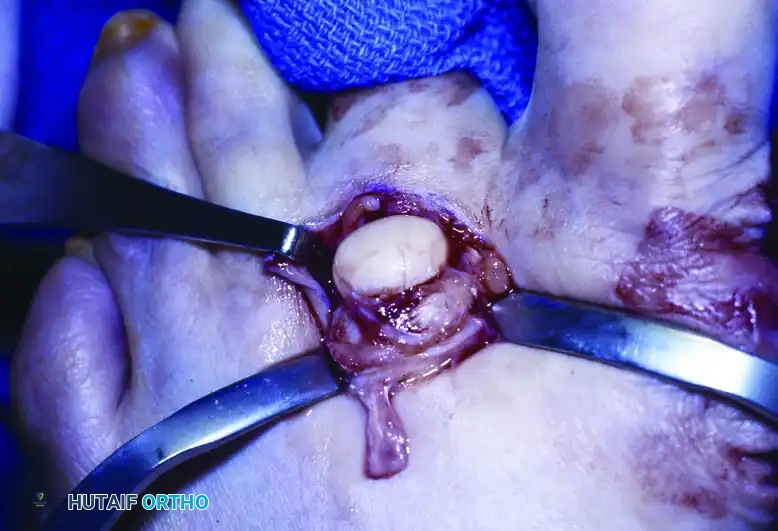
FIGURE 83-35 Arthroplasty of metatarsophalangeal joint. B, Acute flexion of second toe after sectioning of collateral ligaments.
- Inspect the plantar condyles. Using a rongeur or oscillating saw, resect the prominent plantar condyle (usually the fibular/lateral condyle) that corresponds to the location of the IPK.
- Rasp the remaining bone to a smooth contour. Flush the joint copiously to remove bone debris, and close the capsule and skin in layers.
2. Dorsiflexion Osteotomy
A diffuse callosity in which the involved metatarsal head is globally more prominent or plantarflexed relative to the adjacent metatarsal heads requires a structural elevation of the ray. A dorsiflexion osteotomy (often a dorsal closing wedge osteotomy) is indicated.
Technique Overview:
* The osteotomy is typically performed at the metatarsal surgical neck or base, depending on surgeon preference and the degree of elevation required.
* A dorsal wedge of bone (1 to 3 millimeters, depending on the required correction) is removed.
* The osteotomy is closed, effectively elevating the metatarsal head away from the plantar skin.
* Rigid internal fixation (using a K-wire, screw, or low-profile plate) is essential to prevent non-union or excessive dorsal displacement, which would lead to transfer metatarsalgia.
3. Shortening Osteotomy (Weil Osteotomy)
For a diffuse callosity in which the radiograph demonstrates an abnormally long metatarsal (disrupting the normal cascade where the 2nd metatarsal is longest, followed by the 1st/3rd, 4th, and 5th), a shortening osteotomy is indicated. The Weil osteotomy is the gold standard for this pathology.
Technique Overview:
* Through a dorsal approach, the MTP joint is exposed.
* An intra-articular osteotomy is performed starting at the dorsal aspect of the metatarsal head, aiming proximally and plantarly. The saw blade must be kept strictly parallel to the plantar weight-bearing surface of the foot.
* The capital fragment is translated proximally by the desired amount (usually 2 to 5 mm) to shorten the ray and relieve the plantar pressure.
* Because the cut is parallel to the ground, proximal translation does not significantly depress the metatarsal head.
* The osteotomy is secured with one or two small fragment screws (e.g., 2.0 mm or 2.7 mm) directed from dorsal to plantar. The overhanging dorsal bone of the proximal fragment is then resected flush with the articular cartilage.
💡 Clinical Pearl: Avoiding Transfer Lesions
The most dreaded complication of any metatarsal osteotomy is transfer metatarsalgia—the development of a new IPK under an adjacent metatarsal head. This occurs in up to 15% of cases and is usually the result of over-shortening or over-elevating the index metatarsal. Precise preoperative templating and intraoperative fluoroscopic assessment of the metatarsal parabola are critical to minimizing this risk.
POSTOPERATIVE PROTOCOL FOR METATARSAL PROCEDURES
The postoperative management following metatarsal arthroplasty or osteotomy requires strict adherence to offloading principles to ensure osseous union and soft tissue healing.
- Immediate Postoperative Phase (Weeks 0-2):
- The foot is placed in a bulky, soft compressive dressing.
- Weight-bearing is restricted to heel-touch only, utilizing a rigid postoperative shoe or a controlled ankle motion (CAM) boot.
- Elevation is strictly enforced to minimize edema, which can compromise wound healing.
- Sutures are removed at 10 to 14 days, provided the incision is fully coapted and dry.
- Intermediate Phase (Weeks 2-6):
- For osteotomies, protected weight-bearing continues until radiographic evidence of bridging callus is observed (typically 4 to 6 weeks).
- For arthroplasties, progressive weight-bearing as tolerated can begin earlier, though the toe should remain buddy-taped to prevent coronal plane deviation.
- Active and passive range of motion exercises of the MTP joint are initiated to prevent arthrofibrosis, particularly after a Weil osteotomy, which is notorious for causing postoperative joint stiffness.
- Long-Term Management:
- Transition to supportive, wide toe-box footwear.
- Custom orthotics with metatarsal relief may be prescribed to permanently support the transverse arch and prevent the recurrence of mechanical overload.
COMPLICATIONS AND MANAGEMENT
While surgical intervention for intractable corns and keratoses can be highly successful, the surgeon must be prepared to manage potential complications:
- Recurrence and Transfer Lesions: As noted, there is a 10% to 15% risk of recurrence or transfer of the lesion. Transfer metatarsalgia requires a return to conservative management (custom orthotics) and, rarely, revision surgery to address the newly overloaded ray.
- Infection: The plantar skin and interdigital web spaces are heavily colonized. Meticulous preoperative preparation, prophylactic antibiotics, and delayed suture removal mitigate this risk. Superficial infections are managed with oral antibiotics; deep infections may require surgical debridement and hardware removal.
- Non-union/Malunion: Osteotomies of the lesser metatarsals carry a risk of non-union, particularly in patients with compromised vascularity or those who are non-compliant with weight-bearing restrictions. Rigid internal fixation and strict postoperative protocols are preventative.
- Toe Deformity: Over-resection during arthroplasty or failure to repair the collateral ligaments/capsule can lead to a flail toe, dorsal subluxation, or a crossover toe deformity. Careful soft tissue balancing and buddy taping are essential.
- Web Creep: Following partial syndactylization, distal migration of the web space (web creep) can occur if the skin flaps are closed under tension or if the apex is not properly excised.
By adhering to strict indications, performing a comprehensive biomechanical evaluation, and executing precise surgical techniques, the orthopaedic surgeon can effectively manage these challenging hyperkeratotic lesions, restoring pain-free ambulation and improving the patient's quality of life.
📚 Medical References
You Might Also Like