Partial Nail Plate and Matrix Removal: The Winograd Technique
Key Takeaway
The Winograd technique is a highly effective surgical intervention for late stage II and stage III onychocryptosis (ingrown toenail). This procedure involves the partial removal of the offending nail plate followed by complete sharp excision or chemical ablation of the underlying germinal and sterile matrix. Meticulous surgical execution, including the removal of the adjacent phalangeal periosteum, is critical to minimizing recurrence rates and ensuring optimal functional outcomes.
Introduction to Onychocryptosis and Matrix Ablation
Onychocryptosis, commonly known as an ingrown toenail, is a pervasive and often debilitating condition encountered frequently in orthopedic and podiatric practice. It is characterized by the penetration of the lateral or medial edge of the nail plate into the adjacent soft tissue of the nail fold, inciting a robust foreign-body inflammatory response, secondary bacterial colonization, and the formation of hypertrophic granulation tissue.
While early-stage disease may be managed conservatively, refractory cases or advanced presentations necessitate surgical intervention. Probably the most frequently performed and historically validated operative procedure for an ingrown toenail is the partial nail plate and matrix removal described by Winograd. Although his original seminal report involved only five patients, numerous subsequent large-scale clinical reports have unequivocally affirmed the usefulness, reliability, and durability of the technique.
The Winograd technique is particularly useful in late stage II (characterized by active infection and purulent drainage) or stage III disorders (characterized by chronic hypertrophy of the lateral nail fold and granulation tissue). It is the procedure of choice, especially after a previous, unsuccessful partial or complete nail removal where recurrent spicules have formed.
Clinical Pearl: We have not found it strictly necessary to treat the wound with systemic or local antibiotics for several days before the procedure to reduce local infection. The removal of the offending foreign body (the nail plate) and the excision of the granulation tissue are usually curative. However, there is no contraindication to preoperative antibiotic optimization if profound cellulitis is present.
Surgical Anatomy and Biomechanics of the Nail Unit
A profound understanding of the perionychial anatomy is mandatory for successful matrix ablation. The nail unit consists of the nail plate, the nail bed (comprising the sterile and germinal matrices), the eponychium (proximal nail fold), the paronychium (lateral nail folds), and the hyponychium (distal nail bed).
The germinal matrix is the engine of nail production. It extends proximally 5 to 8 mm beneath the eponychium and terminates at the lunula (the visible, crescent-shaped whitish area at the base of the nail). The lateral horns of the germinal matrix curve deeply into the proximal-lateral corners of the nail fold.
Surgical Warning: The most common cause of recurrence following a Winograd procedure is the failure to completely identify and excise the proximal lateral horn of the germinal matrix. Because the matrix is intimately adherent to the periosteum of the distal phalanx, complete ablation often requires the excision of the underlying periosteum.
Preoperative Preparation and Positioning
Patient Positioning
The patient is placed in the supine position on the operating table. The affected foot is positioned at the edge of the table to allow the surgeon unobstructed 360-degree access to the digit.
Anesthesia and Hemostasis
A digital block is performed using a 50/50 mixture of 1% Lidocaine and 0.5% Bupivacaine (traditionally without epinephrine to avoid ischemic complications, though modern literature supports its safe use in healthy patients).
A bloodless surgical field is absolutely critical. The pearly white germinal matrix cannot be accurately differentiated from surrounding subcutaneous fat and fibrous tissue in a bloody field. A digital tourniquet (such as a sterile Penrose drain or a commercial digital ring tourniquet) is applied to the base of the toe.
Surgical Technique 87-3: Chemical Ablation (Phenol Matrixectomy)
While the classic Winograd procedure utilizes sharp dissection, chemical ablation using phenol is a highly effective alternative for partial matrix removal. Phenol acts as a caustic agent that denatures proteins, effectively destroying the germinal matrix cells.
Step 1: Nail Elevation
The offending lateral or medial nail edge is bluntly elevated longitudinally from the underlying sterile matrix using a small periosteal elevator or a straight hemostat.

Step 2: Tissue Protection
To prevent chemical burns to the surrounding healthy skin, a protective barrier of antibiotic gel or petroleum jelly is meticulously placed around the eponychial and paronychial nail folds.

Step 3: Phenol Application
An 88% phenol solution is utilized. A small cotton pledget or a specialized applicator dipped in the phenol solution is introduced deeply into the nail groove, ensuring it reaches the proximal extent of the germinal matrix under the eponychium.

The phenol is typically applied for three consecutive cycles of 30 to 60 seconds each. The area is then thoroughly lavaged with isopropyl alcohol or saline to neutralize the phenol and wash away any residual caustic agent.
Step 4: Dressing Application
The ablated nail groove is covered with a nonadherent gauze (e.g., Adaptic or Xeroform), and a bulky, nonconstricting toe dressing is applied.

The final appearance of the nail after successful phenol ablation demonstrates a clear, widened lateral gutter devoid of the offending nail plate, with the surrounding soft tissue preserved.

Surgical Technique 87-4: The Winograd Procedure (Sharp Matrixectomy)
For severe, recurrent, or hypertrophic cases, the sharp excision technique described by Winograd provides definitive mechanical removal of the matrix.
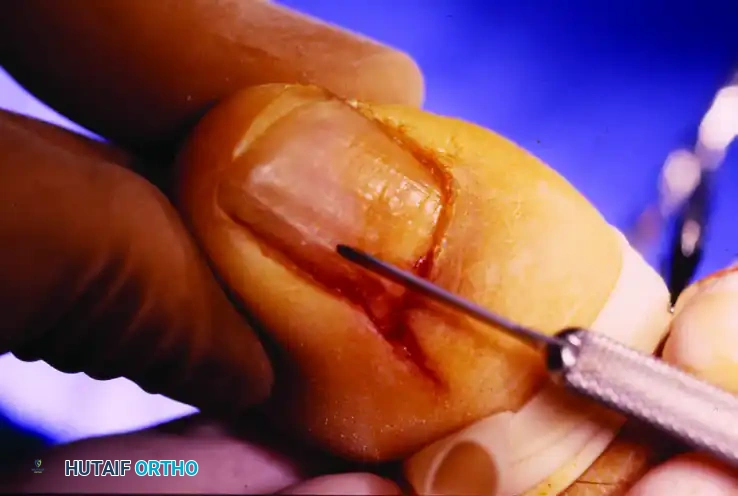
Phase 1: Incision and Exposure
The procedure begins with a precise longitudinal incision to expose the hidden proximal nail root.

- Beginning 5 to 8 mm proximal to the lunula, make a longitudinal incision in the eponychium extending distally to the distal edge of the nail plate.
- Lift the eponychial flap by sharp dissection to reveal the nail root overlying the lateral margin of the germinal matrix. The remainder of the eponychium should be left completely undisturbed to prevent unnecessary cosmetic deformity.
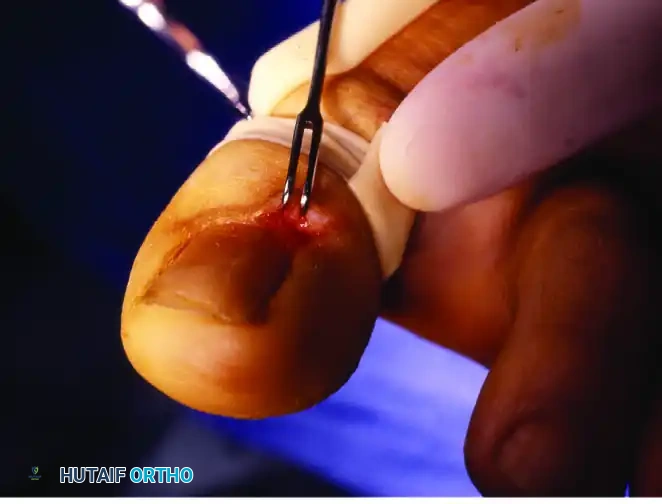
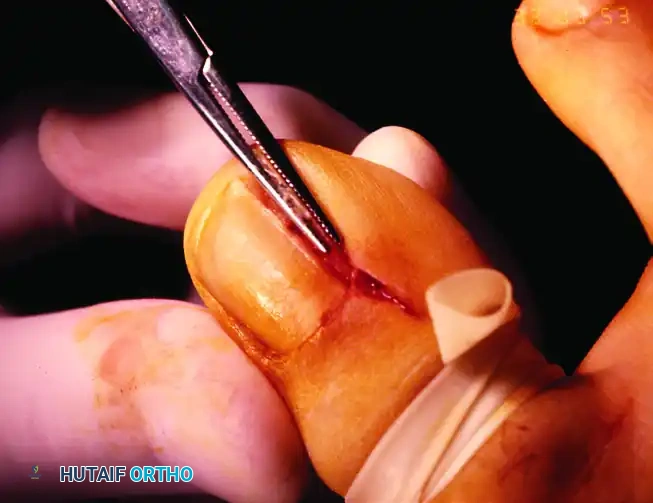
Phase 2: Nail Plate Mobilization and Splitting
Once the proximal root is exposed, the offending segment of the nail plate must be isolated and removed.
- Using a small nasal elevator or a small, straight hemostat, lift the lateral border of the nail out of the nail fold. Pass the instrument beneath the lateral fourth of the exposed nail, separating it from the underlying sterile matrix.

- Score the nail plate longitudinally to create a precise track for the splitter.
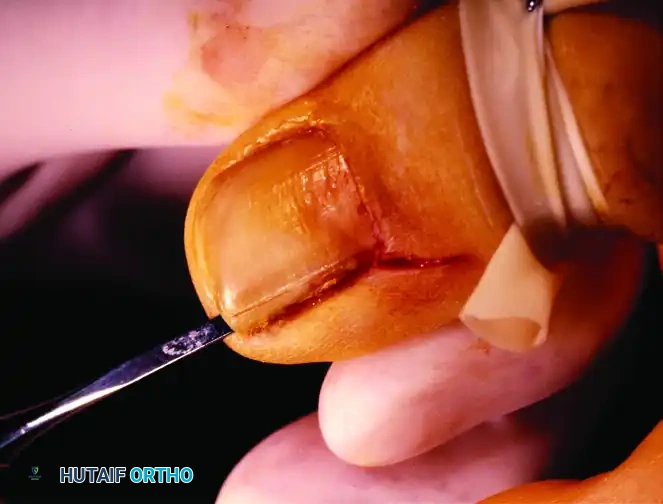
- Incise this nail margin with a heavy-duty nail splitter or English anvil along the previously scored mark. It is imperative to ensure the splitter reaches the most proximal edge of the nail plate beneath the eponychial flap.
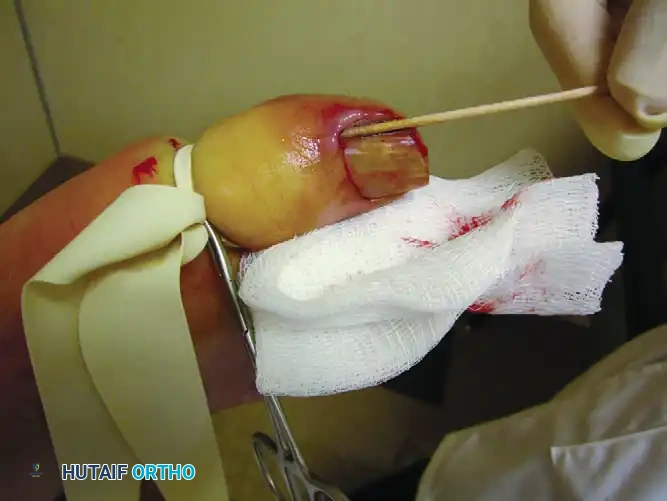
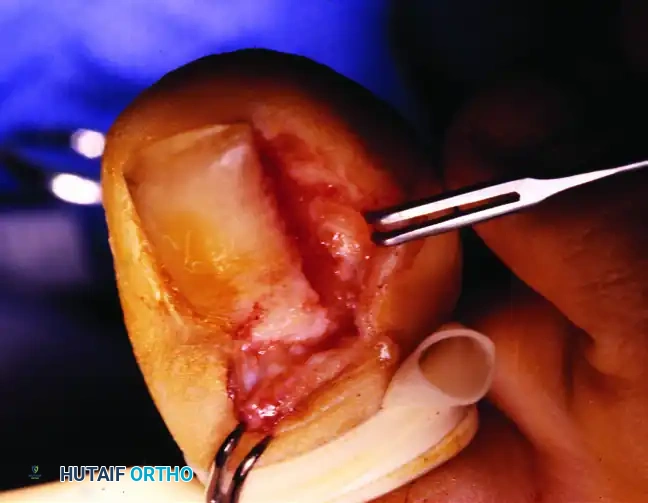
Phase 3: Extraction of the Nail Segment
With its eponychial cover already reflected and the undersurface of the nail plate lifted off its bed, the isolated segment is ready for extraction.

- Grasp the isolated lateral segment of the nail with a straight hemostat.
- Gently remove this entire portion of the plate by applying a rolling motion toward the midline of the toe. This prevents tearing of the proximal root.
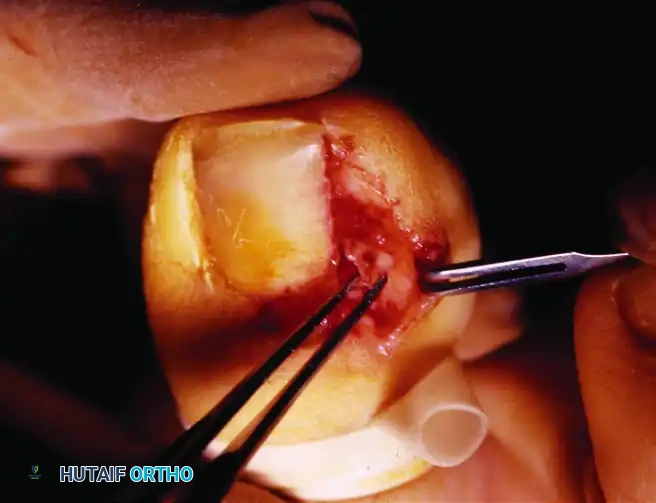
- Removal of the nail plate exposes the underlying matrix. The pearly colored germinal matrix will now be visible. Note that the matrix curves on the undersurfaces of the paronychium and eponychium.
Phase 4: Matrix Ablation (The Critical Step)
The success of the Winograd procedure hinges entirely on the complete eradication of the matrix in the affected gutter.

- Remove the exposed matrix by sharp dissection using a #15 or #64 Beaver scalpel blade.
- Retract the lateral nail fold to fully expose the lateral margin of the matrix.
- Remove the entire matrix—both the sterile and germinal portions. Take special care to remove the proximal portion of the germinal matrix folding on the eponychium and paronychium. This must be removed by sharp dissection from around the nail horns to reduce the likelihood of recurrent nail formation.
Surgical Pitfall: Even after great care, the patient occasionally develops a tiny nail remnant (spicule) that may or may not be symptomatic. The surgeon should be absolutely certain that the periosteum of the distal phalanx has been removed along with the matrix in this lateral gutter, because this is the most certain means of complete matrix ablation.
An attempt to bring the lateral margin of the nail fold to the remaining nail is optional. Historically, Heifetz recommended the excision of part of the hypertrophic lateral nail fold to reduce soft tissue impingement, which can be performed concurrently if severe granulation tissue is present.
Phase 5: Closure and Dressing
Once the nail plate and matrix have been completely removed, the surgical site is prepared for closure.
- Return the proximal eponychial flap to its original location. Sutures to hold it there are optional, but closing the wound generally shortens convalescence and improves immediate postoperative hemostasis. If suturing, use a fine non-absorbable suture (e.g., 4-0 or 5-0 Nylon).

- Apply a nonadherent dressing (such as Xeroform or Adaptic) directly over the exposed phalanx and surgical site.
- Follow this with a nonconstricting, bulky gauze wrap to absorb postoperative exudate and provide mechanical protection.

Postoperative Care and Rehabilitation
Meticulous postoperative care is essential to prevent infection and ensure secondary intention healing of the nail bed.
- Immediate Phase (0-48 Hours): The extremity is strictly elevated for the first 48 hours to minimize throbbing pain and edema. The initial surgical dressing remains in place during this time.
- Wound Care Phase (Days 3-14): At 48 hours, the bulky dressing is removed. Warm water or Epsom salt soaks are begun for 10 minutes, several times a day. This helps debride fibrinous exudate and prevents premature crusting. After soaking, the wound is covered with only a simple adhesive bandage.
- Footwear Modifications: No standard shoe or hosiery is worn for the first 5 to 7 days. The patient is restricted to a postoperative wooden-soled shoe or a rigid surgical sandal that has no toe box, preventing any pressure on the healing digit.
- Return to Activity: Later (typically after 1 to 2 weeks), a wide toe box shoe usually can be worn without discomfort. Full athletic activities are resumed once the wound is fully epithelialized and non-tender.
Outcomes and Complications
Recurrence rates for ingrown toenails vary wildly in the literature, ranging from 0% to 86%. This massive discrepancy is almost entirely technique-dependent.
This rate can be drastically lowered by ensuring full, unobstructed exposure of the germinal matrix, followed by its complete, aggressive sharp removal down to the bone. Recurrence rates are notably higher in patients with previous nail ablations. This is likely secondary to altered anatomy and dense scarring, which leads to incomplete exposure and subsequent failure to eradicate the residual germinal matrix horns.
Other potential complications include postoperative infection (which is minimized by thorough debridement of granulation tissue), epidermal inclusion cysts (if matrix cells are buried during closure), and cosmetic nail dystrophy. Adherence to the strict anatomical principles of the Winograd technique ensures that these complications remain exceedingly rare.
You Might Also Like
