Management of the Painful Heel: A Comprehensive Surgical Guide
Key Takeaway
Painful heel syndrome, encompassing plantar fasciitis and Baxter’s nerve entrapment, remains a prevalent orthopedic challenge. While over 90% of cases resolve with conservative modalities such as orthoses, stretching, and extracorporeal shock wave therapy, recalcitrant cases may require surgical intervention. This guide details the biomechanical windlass mechanism, clinical evaluation, and step-by-step operative techniques, including partial plantar fasciotomy and neurolysis of the first branch of the lateral plantar nerve, ensuring optimal patient outcomes.
Introduction to the Painful Heel Syndrome
The "painful heel" represents one of the most ubiquitous yet historically enigmatic complaints encountered in orthopedic practice. In 1922, Stiell astutely observed that the painful heel "appears to be a condition which is seldom efficiently treated, for the simple reason that the causation is not exactly diagnosed." Decades later, Lapidus and Guidotti echoed this sentiment, noting that the term was used deliberately in preference to a precise etiological diagnosis because the exact cause remained elusive.
Today, while our understanding of specific pathologies—such as Achilles tendinopathy, retrocalcaneal bursitis, and posterior tibial or flexor hallucis longus tendinitis—has vastly improved, idiopathic pain beneath the anteromedial prominence of the calcaneal tuberosity remains a clinical challenge. The modern orthopedic surgeon must approach this syndrome with a comprehensive understanding of foot biomechanics, neuroanatomy, and evidence-based treatment algorithms, recognizing that "painful heel syndrome" is often a confluence of mechanical overload, degenerative changes, and occasionally, neurogenic entrapment.
Applied Anatomy and Biomechanics
A profound understanding of the plantar anatomy and the dynamic biomechanics of the longitudinal arch is prerequisite for diagnosing and treating heel pain.
The Plantar Aponeurosis and the Windlass Mechanism
The plantar fascia is a dense, fibrous connective tissue structure comprising medial, central, and lateral bands. The central component, which is the thickest and most clinically relevant, originates from the medial process of the calcaneal tuberosity.
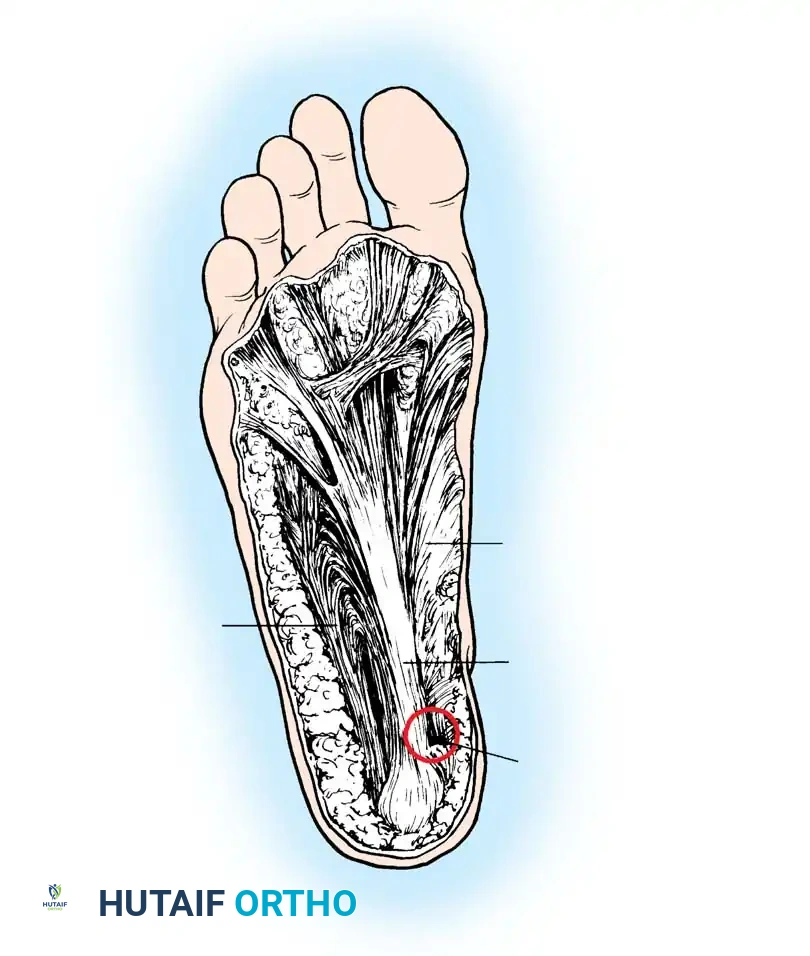
As described by the English anatomist Hicks, the plantar fascia functions via a "windlass mechanism." The fascia inserts distally through several slips into the plantar plates of the metatarsophalangeal (MTP) joints, the flexor tendon sheaths, and the bases of the proximal phalanges. During the terminal stance phase of gait, as the toes are dorsiflexed, the plantar fascia is pulled distally around the metatarsal heads (the drum of the windlass). This action tightens the fascia, elevates the longitudinal arch, and places immense traction on its calcaneal origin.
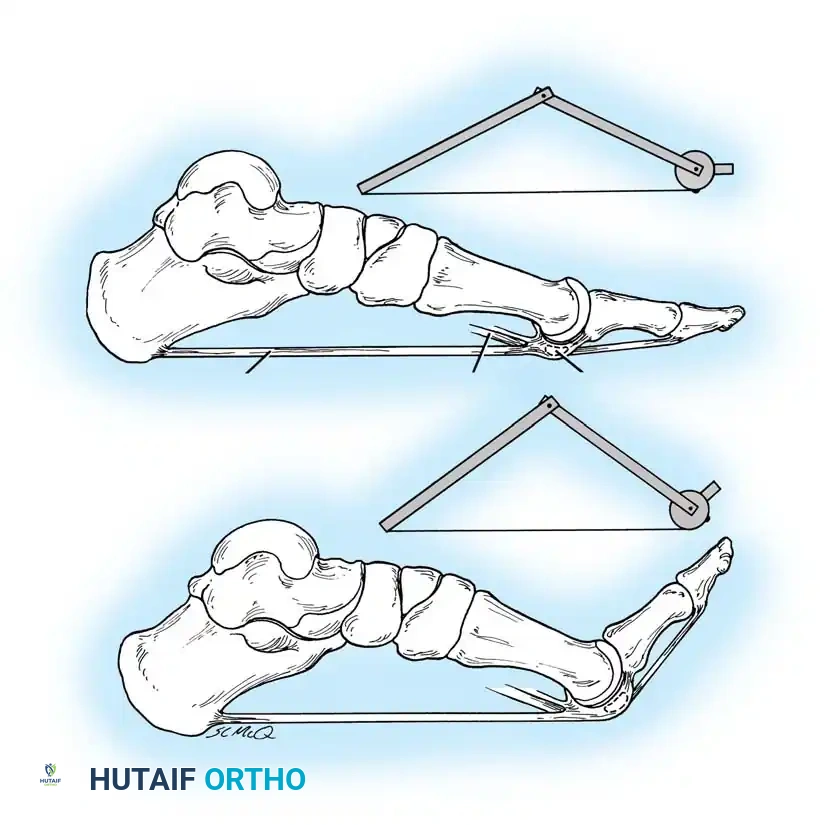
Extensive laboratory studies by Kitaoka et al. have established that the plantar fascia is the primary static supporting structure of the longitudinal arch. Furthermore, Murphy, Arangio, Chen, Salathe, and Kim have demonstrated that significant biomechanical collapse occurs in the longitudinal arch following complete sectioning of the plantar fascia, underscoring the necessity of preserving its integrity during surgical intervention.
The Calcaneal Heel Pad
With advancing age, the elastic adipose tissue of the heel pad undergoes constant degenerative changes. Aging precipitates a gradual reduction in collagen, water content, and elastic fibrous tissue. This atrophy diminishes the shock-absorbing capacity of the heel pad, directly contributing to mechanical soreness under the calcaneal tuberosity during weight-bearing.
Neuroanatomy: Baxter’s Nerve
A critical, yet historically underappreciated, cause of painful heel syndrome is the entrapment of the first branch of the lateral plantar nerve, commonly known as Baxter’s nerve.
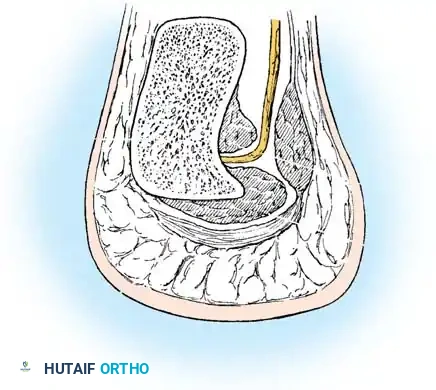
This small nerve branches from the lateral plantar nerve and courses inferiorly and laterally between the deep surface of the abductor hallucis muscle and the medial aspect of the quadratus plantae muscle. It then passes immediately anterior to the medial calcaneal tuberosity (often adjacent to a calcaneal spur) to innervate the abductor digiti minimi muscle. Schon and Baxter proposed that neurogenic entrapment of this nerve accounts for 1% to 2% of painful heel cases, necessitating specific diagnostic and surgical attention.
Etiology and Pathogenesis
The etiology of painful heel syndrome is multifactorial, broadly categorized into mechanical, degenerative, and neurogenic origins:
- Mechanical Traction (Plantar Fasciitis): Repetitive traction from the windlass mechanism leads to microscopic tears and subsequent cystic degeneration at the origin of the plantar fascia and the underlying flexor digitorum brevis. Woolnough aptly termed this "tennis heel," drawing a direct pathophysiological parallel to the tendinous degeneration seen in the extensor carpi radialis brevis in tennis elbow.
- Degenerative Changes: Age-related atrophy of the calcaneal fat pad reduces energy dissipation during heel strike.
- Neurogenic Entrapment: Compression of Baxter's nerve beneath the deep fascial edge of the abductor hallucis muscle or adjacent to a calcaneal spur.
- Systemic Arthropathies: In cases of bilateral or atypical heel pain, systemic conditions such as rheumatoid arthritis, ankylosing spondylitis, and Reiter syndrome must be considered.
Clinical Pearl: In diabetic patients presenting with acute, severe heel pain, maintain a high index of suspicion for a deep soft-tissue abscess, which can rapidly compromise the viability of the foot.
Clinical Evaluation
History and Physical Examination
The typical patient is between 40 and 70 years of age, active, and presents with unilateral symptoms. Obesity is a significant predisposing factor that exacerbates symptoms and complicates conservative management.
The pathognomonic complaint is severe, sharp pain beneath the heel upon taking the first steps in the morning or after a period of prolonged sitting ("start-up pain"). The pain typically diminishes after a few steps but evolves into a dull ache toward the end of the day, relieved only by non-weight-bearing.
Physical examination reveals localized, exquisite tenderness at the inferomedial aspect of the calcaneal tuberosity. Mild swelling and erythema may be present when compared to the contralateral asymptomatic heel.
To differentiate mechanical plantar fasciitis from neurogenic entrapment, careful palpation is required. Patients with isolated plantar fasciitis exhibit tenderness strictly at the medial tubercle. Conversely, patients with Baxter's nerve entrapment will demonstrate tenderness radiating proximally along the course of the lateral plantar nerve, inferior to the flexor retinaculum.
Diagnostic Imaging
- Radiographs: Weight-bearing lateral radiographs reveal a calcaneal traction spur in approximately 50% of patients. However, the presence of a spur is largely incidental. Tanz demonstrated that calcaneal spurs are frequently found in asymptomatic adults, and Lapidus and Guidotti noted that many patients with severe unilateral symptoms possess bilateral spurs. The spur itself is rarely the primary source of pain; rather, it is a radiographic marker of chronic traction at the origin of the flexor digitorum brevis.
- Bone Scans: Technetium-99m bone scanning is highly sensitive. Graham demonstrated increased isotope uptake at the anteroinferior medial aspect of the calcaneus in nearly all symptomatic patients. This modality is particularly useful for ruling out calcaneal stress fractures in recalcitrant cases.
- Electromyography (EMG): EMG of the abductor digiti minimi muscle can be a valuable adjunct if symptoms persist for several months and neurogenic entrapment of Baxter's nerve is suspected.
Non-Operative Management
Conservative management is the cornerstone of treatment. Over 90% of patients achieve symptom resolution within 6 to 9 months without surgical intervention.
- Mechanical Support: Rigid or semi-rigid orthoses, silicone heel cups, and arch supports distribute weight-bearing forces and reduce tension on the plantar fascia. Snook and Chrisman reported an 81% success rate using simple plastic heel cups.
- Pharmacotherapy: Oral nonsteroidal anti-inflammatory drugs (NSAIDs) provide symptomatic relief of the inflammatory component.
- Physical Therapy: Aggressive stretching of the Achilles tendon (to address equinus contractures) and the plantar fascia is critical. Night splints maintain the fascia in an elongated state during sleep, preventing morning start-up pain.
- Corticosteroid Injections: Local steroid injections can provide profound short-term relief but carry significant risks.
Surgical Warning: Acevedo and Beskin reported a high incidence of plantar fascia rupture following corticosteroid injections. Rupture often leads to a measurable drop in the calcaneal pitch angle and chronic lateral column pain. Patients must be explicitly warned of this complication prior to injection.
Extracorporeal Shock Wave Therapy (ESWT)
For chronic, insertional plantar fasciitis unresponsive to traditional conservative measures, ESWT has emerged as a highly effective, non-invasive alternative. ESWT delivers concentrated ultrasound energy to the localized area of collagen disruption, inducing microtrauma that stimulates neovascularization and tissue regeneration.
Extensive studies by Ogden et al. demonstrated a 95% success rate at 1-year follow-up in placebo-controlled trials. Similar efficacy has been corroborated by Chen, Hammer, Theodore, Alvarez, and Rompe. ESWT is now considered a safe and effective bridge between failed conservative therapy and surgical intervention.
Surgical Management of Chronic Heel Pain Syndrome
Surgery is indicated only for the rare patient (less than 5%) who experiences debilitating, recalcitrant pain despite 6 to 12 months of exhaustive conservative management, including orthoses, stretching, injections, and ESWT.
Historically, various procedures have been proposed, including horseshoe incisions for complete soft-tissue release (Griffith), calcaneal osteotomies (Steindler and Smith), and simple calcaneal drilling for "decompression" (Hassab and El-Sherif). However, the modern gold standard involves a targeted medial approach for partial plantar fasciotomy and neurolysis of Baxter's nerve.
Preoperative Planning and Patient Counseling
Patients must be extensively counseled that surgery is not universally successful. If the surgical plan does not include excision of an asymptomatic calcaneal spur, the patient must be informed preoperatively to prevent psychological dissatisfaction postoperatively, as patients often fixate on the radiographic spur as the source of their pain.
Surgical Technique: Medial Approach for Fasciotomy and Neurolysis
Positioning: The patient is placed in the supine position with a bump under the ipsilateral hip to externally rotate the leg, providing optimal access to the medial aspect of the hindfoot. A thigh tourniquet is applied.
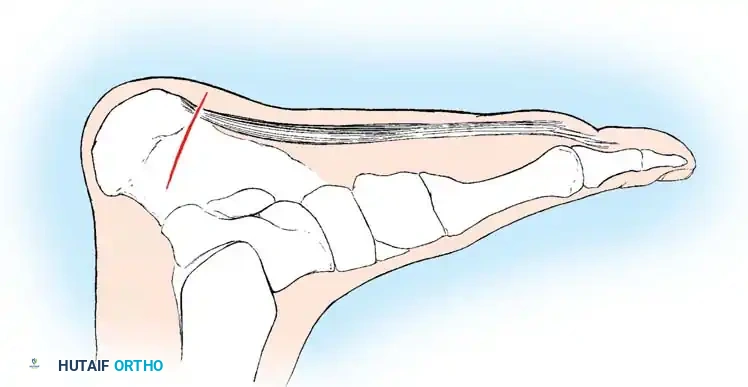
Step 1: Incision and Superficial Dissection
A 4- to 5-cm oblique incision is made over the medial aspect of the heel, centered over the point of maximal tenderness, typically just distal to the medial calcaneal tuberosity.
Careful blunt dissection is carried through the subcutaneous fat to avoid injury to the medial calcaneal sensory nerve branches, which arborize in this region.
Step 2: Identification of the Abductor Hallucis
The superficial fascia is incised, revealing the deep fascia overlying the abductor hallucis muscle. The superior and inferior margins of the abductor hallucis are identified.
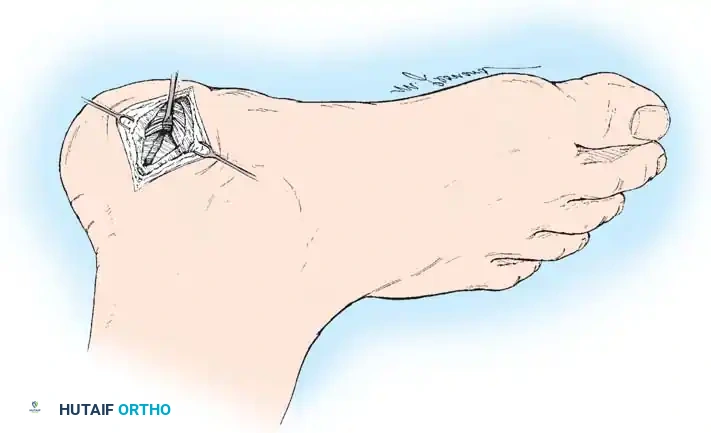
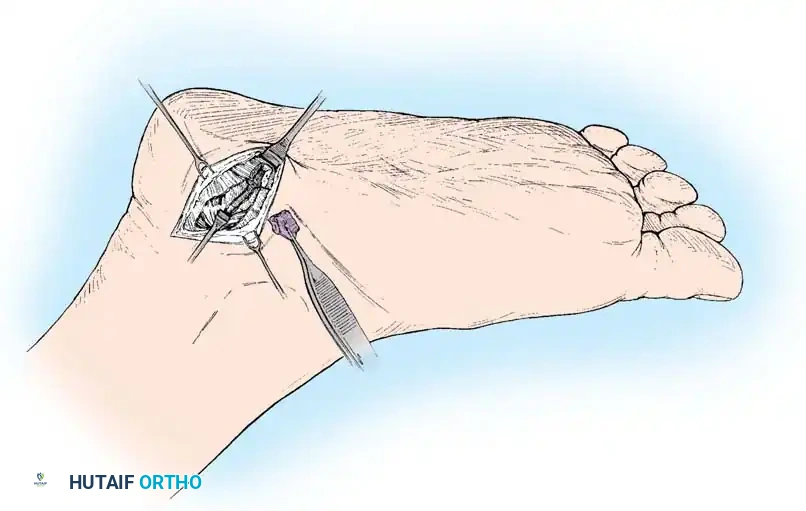
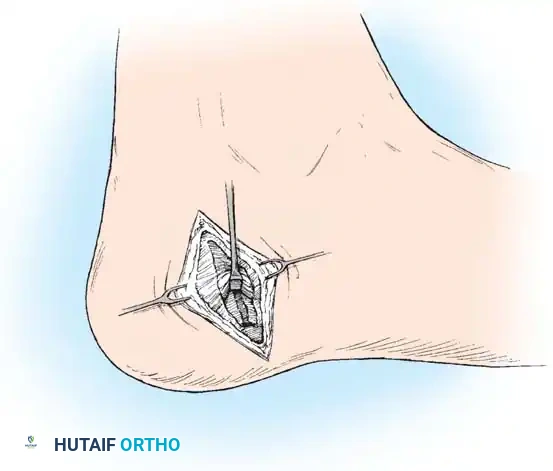
Step 3: Release of the Deep Fascia and Neurolysis
The deep fascial edge of the abductor hallucis muscle is sharply released. Retracting the muscle belly superiorly exposes the underlying quadratus plantae and the origin of the flexor digitorum brevis. At this juncture, the first branch of the lateral plantar nerve (Baxter's nerve) is identified as it courses vertically between these muscle bellies. Complete neurolysis is performed by releasing any tight fascial bands compressing the nerve.
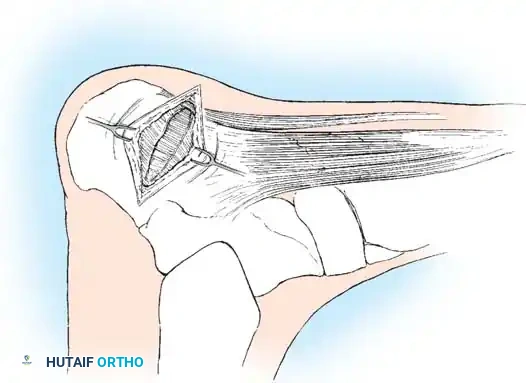
Step 4: Partial Plantar Fasciotomy
The medial band and the medial aspect of the central band of the plantar fascia are identified at their insertion onto the calcaneal tuberosity. A partial fasciotomy is performed, releasing only the medial one-third to one-half of the fascia.
Surgical Pitfall: Complete release of the plantar fascia must be strictly avoided. Complete sectioning eliminates the primary static support of the longitudinal arch, leading to arch collapse, midfoot pain, and lateral column overload.
Step 5: Management of the Calcaneal Spur (Optional)
If a large calcaneal spur is present and deemed a source of mechanical irritation, it may be excised. Snook and Chrisman advocate for excising the medial tubercle along with the spur to broaden the weight-bearing area and flatten the plantar surface of the calcaneus, thereby relieving focal pressure. This is performed using a sharp osteotome or rongeur, followed by smoothing with a rasp.
Step 6: Closure
The wound is irrigated copiously. The subcutaneous tissues are closed with absorbable sutures, and the skin is closed with non-absorbable interrupted sutures. A bulky, compressive soft dressing is applied.
Postoperative Protocol
- 0 to 2 Weeks: The patient is placed in a short-leg cast or rigid fracture boot and maintained strictly non-weight-bearing to allow for soft tissue healing and to prevent early catastrophic failure of the remaining plantar fascia.
- 2 to 4 Weeks: Sutures are removed. The patient transitions to progressive weight-bearing in a controlled ankle motion (CAM) boot.
- 4 to 8 Weeks: Transition to supportive athletic footwear with custom orthoses. Physical therapy is initiated, focusing on intrinsic foot muscle strengthening, Achilles stretching, and proprioceptive training.
- Return to Activity: Most patients can resume normal daily activities by 8 to 10 weeks, with a return to high-impact sports delayed until 4 to 6 months postoperatively.
Complications
While generally safe, surgical intervention for painful heel syndrome carries specific risks:
* Lateral Column Overload: The most common biomechanical complication following over-resection of the plantar fascia.
* Nerve Injury: Iatrogenic injury to the medial calcaneal nerve branches or the lateral plantar nerve can result in painful neuromas or chronic numbness.
* Infection and Wound Dehiscence: Particularly in diabetic or obese patients, the thick heel pad is susceptible to delayed healing.
* Persistent Pain: A subset of patients will experience no relief despite technically flawless surgery, highlighting the complex, multifactorial nature of this enigmatic condition.
You Might Also Like
