Neurogenic Disorders of the Foot and Ankle: Comprehensive Surgical Management
Key Takeaway
Tarsal tunnel syndrome and neurogenic cavus foot deformities require meticulous clinical evaluation and precise surgical intervention. Diagnosis relies heavily on patient history, provocative maneuvers like the Kinoshita test, and specific electromyographic criteria. Surgical management ranges from targeted nerve decompression and excision of space-occupying lesions, such as neurilemomas, to complex multi-planar osteotomies and arthrodeses for rigid cavovarus deformities driven by neuromuscular pathologies like Charcot-Marie-Tooth disease.
Neurogenic Disorders of the Foot and Ankle
Neurogenic disorders of the foot and ankle encompass a broad spectrum of pathologies ranging from localized peripheral nerve entrapments to complex, progressive neuromuscular deformities. The successful management of these conditions demands a profound understanding of lower extremity biomechanics, peripheral neuroanatomy, and the intricate balance of dynamic tendon forces. This comprehensive guide details the evaluation, diagnosis, and surgical management of primary neurogenic disorders, including Tarsal Tunnel Syndrome, Anterior Tarsal Tunnel Syndrome, Interdigital Neuroma, and the Neurogenic Cavus Foot.
Tarsal Tunnel Syndrome (Posterior Tibial Nerve Entrapment)
Anatomy and Etiology
Tarsal tunnel syndrome is an entrapment neuropathy of the posterior tibial nerve or its branches (the medial plantar, lateral plantar, and medial calcaneal nerves) within the fibro-osseous tunnel beneath the flexor retinaculum on the medial aspect of the ankle. The roof of the tunnel is formed by the flexor retinaculum (laciniate ligament), while the floor is composed of the medial surface of the talus, the sustentaculum tali, and the medial calcaneal wall.
The etiology of tarsal tunnel syndrome is multifactorial. While many cases are idiopathic, identifiable causes include trauma (e.g., calcaneal or talar fractures causing osseous impingement), severe hindfoot valgus leading to traction neuropathy, inflammatory arthropathies, and space-occupying lesions. Space-occupying lesions account for a significant percentage of identifiable causes and include ganglion cysts, lipomas, varicosities, and peripheral nerve sheath tumors such as neurilemomas (schwannomas).
Clinical Pearl: Any patient presenting with tenderness over the tibial nerve at the ankle (that is not present contralaterally) should also be examined for an interdigital neuroma in the second or third web space. Occasionally, proximal nerve irritability can manifest as distal symptomatology, representing an "irritable" tibial nerve rather than a true double-crush syndrome.
Clinical Findings and Diagnosis
Despite meticulous attention to detail in the physical examination, the patient's history remains the most revealing diagnostic aid. Patients typically describe a burning, tingling, or aching pain radiating into the plantar aspect of the foot, often exacerbated by prolonged standing or walking and occasionally worsening at night.
Provocative Testing:
Kinoshita et al. described a highly sensitive provocative maneuver to elicit symptoms suggesting tarsal tunnel syndrome.
* The Dorsiflexion-Eversion Test: The ankle is passively and maximally everted and dorsiflexed, while all the metatarsophalangeal (MTP) joints are simultaneously maximally dorsiflexed. This position is held for 5 to 10 seconds.
* In a landmark comparison of 100 asymptomatic control feet with 44 symptomatic feet, this maneuver exacerbated symptoms in 36 of the 44 symptomatic feet. In all 44 symptomatic feet, local tenderness, a positive Tinel sign, or both were either intensified or produced when previously absent. None of the control feet exhibited symptoms during this maneuver.
Electrophysiological Evaluation:
Electromyography (EMG) and nerve conduction velocity (NCV) studies are critical for augmenting the clinical diagnosis.
* Needle Examination: May demonstrate fibrillations and positive sharp waves within the abductor hallucis, first dorsal interosseus, or abductor digiti minimi.
* Motor Latencies: Prolonged distal motor latencies exceeding 6.7 ms in the lateral plantar nerve and 6.1 ms in the medial plantar nerve are highly suggestive. Latencies greater than 7.0 ms are definitively abnormal. Decreased amplitude of motor action potentials in the abductor hallucis and abductor digiti minimi are standard diagnostic markers.
* Sensory Latencies: Prolonged sensory latencies (> 3.2 ms) are considered even more diagnostic than motor latencies.
Surgical Warning: Electrical studies may return normal results in a subset of patients who genuinely possess tarsal tunnel syndrome. Clinical judgment must supersede negative electrodiagnostic studies if the history and physical examination are overwhelmingly positive.
Diagnostic Imaging
While Magnetic Resonance Imaging (MRI) has not been shown to be universally beneficial in determining the functional cause of idiopathic tarsal tunnel syndrome, it is invaluable in surgical planning. MRI ensures the identification of all areas of impingement by delineating fibrofatty bonds, fibrous septa, and space-occupying lesions.
Below is an example of a 40-year-old man presenting with a strongly positive Tinel sign and fullness in the posterior soft tissues. Imaging clearly identifies a neurilemoma.
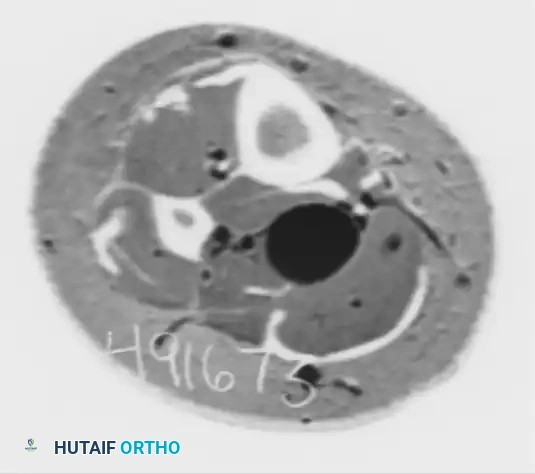
Figure 1: Axial CT scan demonstrating a well-circumscribed mass causing fullness in the posterior soft tissues of the medial ankle.

Figure 2: MRI clearly identifying the neurilemoma within the tarsal tunnel. MRI is critical for delineating the extent of the tumor and its relationship to the tibial nerve branches.
Surgical Treatment: Tarsal Tunnel Release
Surgical decompression is indicated for patients who fail conservative management (orthotics, NSAIDs, immobilization) or those with identified space-occupying lesions.
Patient Positioning and Preparation:
1. The patient is placed supine on the operating table.
2. A thigh tourniquet is applied to ensure a bloodless field, which is critical for identifying the delicate calcaneal nerve branches.
3. The lower extremity is prepped and draped in a standard sterile fashion. The hip may be externally rotated and the knee slightly flexed to expose the medial ankle.
Surgical Approach:
1. Incision: A curvilinear incision is made starting 2 cm proximal and 2 cm posterior to the medial malleolus, extending distally along the course of the tibial nerve, and curving gently toward the navicular tuberosity.
2. Superficial Dissection: The subcutaneous tissues are carefully divided. Extreme caution must be exercised to identify and protect the medial calcaneal nerve branches, which often pierce the flexor retinaculum directly.
3. Retinaculum Release: The proximal edge of the flexor retinaculum is identified and divided completely. The release must extend proximally into the deep fascia of the leg to ensure no proximal kinking of the nerve occurs.
4. Nerve Exploration: The posterior tibial nerve is identified and traced distally to its bifurcation into the medial and lateral plantar nerves.
5. Distal Release (Porta Pedis): The deep fascia of the abductor hallucis muscle must be released. The medial and lateral plantar nerves pass through separate fibro-osseous tunnels beneath the abductor hallucis. The investing fascia and the fibrous septa separating these nerves must be completely excised to prevent distal tethering.
Management of Space-Occupying Lesions:
If a neurilemoma is encountered, meticulous microsurgical dissection is required.
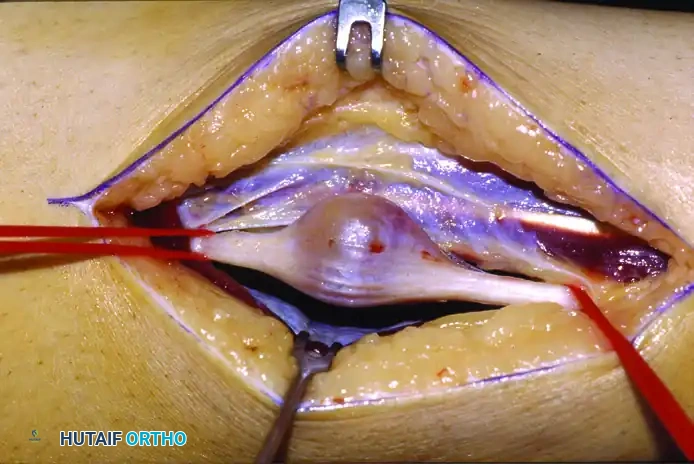
Figure 3: Intraoperative view of the neurilemoma. The nerve sheath tumor is carefully isolated from the surrounding healthy fascicles.

Figure 4: Gross specimen of the excised neurilemoma. Microscopically confirmed as a nerve sheath tumor. Although they are benign, some neurilemomas cannot be removed without the sacrifice of a small, involved nerve branch.
Postoperative Protocol:
* A bulky, non-weight-bearing splint is applied with the ankle in neutral dorsiflexion and slight inversion to minimize tension on the healing wound and nerve.
* Sutures are removed at 2 to 3 weeks.
* Progressive weight-bearing in a CAM boot is initiated at 3 weeks, followed by physical therapy focusing on nerve gliding exercises and posterior tibial tendon strengthening.
Anterior Tarsal Tunnel Syndrome (Deep Peroneal Nerve Entrapment)
Anterior tarsal tunnel syndrome involves the entrapment of the deep peroneal nerve beneath the inferior extensor retinaculum.
Etiology and Diagnosis
The deep peroneal nerve passes under the inferior extensor retinaculum alongside the dorsalis pedis artery. Entrapment is frequently caused by dorsal osteophytes at the talonavicular or metatarsocuneiform joints, tight footwear, or repetitive microtrauma.
Patients present with vague, aching pain over the dorsum of the midfoot and dysesthesia in the first web space. A positive Tinel sign over the deep peroneal nerve at the level of the inferior extensor retinaculum is pathognomonic. EMG/NCV studies may show delayed conduction in the deep peroneal nerve and denervation potentials in the extensor digitorum brevis.
Treatment
Conservative management includes shoe modification (avoiding tight laces) and corticosteroid injections. Surgical decompression involves a dorsal longitudinal incision lateral to the extensor hallucis longus (EHL) tendon. The inferior extensor retinaculum is divided, and any underlying dorsal osteophytes are resected using a rongeur or osteotome to create a flat, unencumbered bed for the nerve.
Interdigital Neuroma (Morton's Neuroma)
Historical Background and Pathology
First described by Thomas Morton in 1876, the interdigital neuroma is not a true neoplasm but rather a perineural fibrosis and nerve degeneration caused by repetitive mechanical irritation. It most commonly affects the third common digital nerve within the third web space, as this nerve often receives communicating branches from both the medial and lateral plantar nerves, making it thicker and more susceptible to tethering beneath the deep transverse metatarsal ligament.
Signs and Symptoms
Patients report a sensation of "walking on a marble" or a pebble in their shoe. Pain radiates into the affected toes and is exacerbated by narrow-toebox footwear.
* Mulder's Sign: A palpable click accompanied by a reproduction of pain when the metatarsal heads are compressed mediolaterally while simultaneously applying dorsal pressure to the plantar web space.
Surgical Treatment
When conservative measures (wide-toe shoes, metatarsal pads, corticosteroid/alcohol injections) fail, surgical excision is indicated.
* Dorsal Approach: A dorsal longitudinal incision is made over the affected web space. The deep transverse metatarsal ligament is identified and transected. The neuroma is pushed dorsally by applying plantar pressure. The nerve is transected as far proximally as possible (proximal to the weight-bearing pad of the metatarsal heads) to prevent a symptomatic stump neuroma.
* Plantar Approach: Reserved for recurrent neuromas. It provides direct access to the proximal nerve stump but carries the risk of a painful plantar scar.
The Cavus Foot: Neurogenic Deformity
The cavus foot is a complex, multi-planar deformity characterized by an abnormally high medial longitudinal arch. In the orthopedic setting, a cavus foot must be considered a manifestation of an underlying neurological disorder until proven otherwise.
Etiology
The most common neurogenic cause is Charcot-Marie-Tooth (CMT) disease, a hereditary sensorimotor neuropathy. Other causes include Friedreich's ataxia, tethered cord syndrome, poliomyelitis, and cerebral palsy.
Pathomechanics and Clinical Findings
The deformity is driven by muscle imbalances. In CMT, the intrinsic muscles of the foot and the anterior tibialis weaken early. The peroneus longus (which plantarflexes the first ray) remains strong, overpowering the weak anterior tibialis. The posterior tibialis remains strong, overpowering the weak peroneus brevis.
The resulting cascade:
1. Plantarflexed First Ray: The unopposed peroneus longus drives the first metatarsal into rigid plantarflexion.
2. Hindfoot Varus: To allow the lateral border of the foot to touch the ground during stance, the hindfoot must roll into varus (the "tripod effect").
3. Claw Toes: Weakness of the intrinsic muscles (lumbricals and interossei) leads to overpowering by the extrinsic extensors (EDL) and flexors (FDL), resulting in MTP hyperextension and IP flexion.
Clinical Evaluation:
* Coleman Block Test: Crucial for determining if the hindfoot varus is flexible or rigid. The patient stands with the lateral border of the foot and the heel on a 1-inch wooden block, allowing the plantarflexed first ray to drop off the medial edge. If the hindfoot corrects to neutral or valgus, the varus is driven entirely by the forefoot (flexible hindfoot). If the heel remains in varus, the hindfoot deformity is rigid and requires bony correction.
Radiographic Findings
Weight-bearing anteroposterior and lateral radiographs are essential.
* Meary's Angle: The angle between the longitudinal axis of the talus and the first metatarsal. In a cavus foot, this angle is increased (convex upward).
* Calcaneal Pitch: Increased (>30 degrees).
* Hibbs Angle: The angle between the calcaneus and the first metatarsal approaches 90 degrees in severe cavus.
Surgical Treatment Principles
Surgical reconstruction of the neurogenic cavus foot is highly individualized, based on the flexibility of the deformity and the specific muscle imbalances present. The goal is to create a plantigrade, stable, and braceable foot.
1. Soft Tissue Releases
- Plantar Fascia Release (Steindler Stripping): The plantar fascia and the origins of the short plantar muscles are released from the calcaneus to correct the midfoot cavus.
- Tendon Transfers:
- Jones Transfer: EHL transferred to the neck of the first metatarsal to elevate the first ray, with IP joint fusion of the hallux.
- Hibbs Transfer: EDL tendons transferred to the lateral cuneiform to assist in ankle dorsiflexion.
- Peroneus Longus to Peroneus Brevis Transfer: Decreases the plantarflexion force on the first ray and augments hindfoot eversion.
2. Cavovarus Driven By Plantarflexed First Ray (Flexible Hindfoot)
If the Coleman block test demonstrates a flexible hindfoot, the primary pathology is the plantarflexed first ray.
* Dorsiflexion Osteotomy of the First Metatarsal: A dorsal closing-wedge osteotomy is performed at the base of the first metatarsal. This elevates the first ray, eliminating the tripod effect and allowing the hindfoot to passively correct to neutral.
3. Calcaneocavovarus and Cavovarus Deformity (Rigid Hindfoot)
If the hindfoot is rigid, soft tissue releases and forefoot osteotomies are insufficient.
* Dwyer Osteotomy: A lateral closing-wedge osteotomy of the calcaneus. This physically translates and angulates the calcaneal tuberosity out of varus and into a neutral or slightly valgus position.
* Lateralizing Calcaneal Slide: The posterior tuberosity is osteotomized and translated laterally by 10 to 15 mm, fixed with large cannulated screws.
4. Midfoot Cavus
For severe midfoot apex deformities, midtarsal osteotomies are required.
* Cole Osteotomy: A dorsal closing-wedge osteotomy through the naviculocuneiform and cuboid joints. This powerfully corrects the arch but shortens the foot.
* Japas Osteotomy: A V-shaped osteotomy through the midfoot, allowing the distal segment to be elevated without shortening the foot.
5. Deformity Associated with Arthritic Changes (Salvage)
In older patients with long-standing, rigid deformities and secondary degenerative joint disease of the subtalar and midtarsal joints, joint-sparing osteotomies will fail to relieve pain.
* Triple Arthrodesis: Fusion of the subtalar, talonavicular, and calcaneocuboid joints. The articular surfaces are resected in a wedged fashion to correct the cavus, varus, and adduction deformities simultaneously. Rigid internal fixation with screws and staples is utilized.
Summary of Cavus Foot Postoperative Protocol
Following complex bony reconstruction, patients are placed in a well-padded short leg cast. Strict non-weight-bearing is enforced for 6 to 8 weeks to allow for osteotomy or fusion consolidation. Radiographic union is confirmed before transitioning to a CAM boot with progressive weight-bearing. Long-term management often requires custom ankle-foot orthoses (AFOs) to accommodate residual muscle weakness and prevent deformity recurrence, particularly in progressive neuropathies like Charcot-Marie-Tooth disease.
You Might Also Like
