Tarsal Tunnel Syndrome: Comprehensive Surgical Management and Decompression Techniques
Key Takeaway
Tarsal tunnel syndrome is a compressive neuropathy of the posterior tibial nerve within the fibro-osseous tunnel beneath the flexor retinaculum. Diagnosis relies on clinical examination, including the dorsiflexion-eversion test, corroborated by electromyography and MRI. Surgical decompression is indicated for space-occupying lesions or refractory cases, requiring meticulous release of the flexor retinaculum and deep fascia to prevent irreversible axonal damage and restore plantar sensation.
Introduction to Neurogenic Disorders of the Foot and Ankle
Neurogenic disorders of the lower extremity present a complex diagnostic and therapeutic challenge for the orthopedic surgeon. Among these, entrapment neuropathies require a profound understanding of regional anatomy, biomechanics, and peripheral nerve pathophysiology. First independently described by Keck and Lam in 1962, Tarsal Tunnel Syndrome (TTS) is the most prominent entrapment neuropathy of the foot and ankle.
Analogous to carpal tunnel syndrome in the upper extremity, TTS involves the constriction of the posterior tibial nerve. However, unlike the median nerve's entrapment beneath the transverse carpal ligament, the tibial nerve is compressed beneath the flexor retinaculum (laciniate ligament). It is critical to recognize that isolated release of the flexor retinaculum is historically less uniformly successful than carpal tunnel release, demanding meticulous patient selection, advanced diagnostic imaging, and precise surgical execution.
Surgical Anatomy and Biomechanics
A masterful surgical release requires an intimate knowledge of the tarsal tunnel's boundaries and contents. The tarsal tunnel is a fibro-osseous conduit situated posterior and inferior to the medial malleolus.
The Flexor Retinaculum (Laciniate Ligament)
The roof of the tarsal tunnel is formed by the flexor retinaculum, an unyielding fibrous band that is typically 2.5 to 3 cm wide. Its borders are anatomically continuous with adjacent fascial structures:
* Proximal Border: Continuous with the deep investing fascia of the posterior calf.
* Distal/Anterior Border: Continuous with the deep plantar fascia of the medial aspect of the sole.
* Attachments: Extends from the medial malleolus posteriorly and inferiorly to the medial aspect of the calcaneal tuberosity.
Tunnel Contents and Septal Architecture
Projecting from the deep surface of the flexor retinaculum to the underlying calcaneus are fibrous septa. These septa compartmentalize the structures passing through the tunnel. From anterior to posterior, the structures are:
1. Tibialis Posterior tendon.
2. Flexor Digitorum Longus (FDL) tendon.
3. Posterior Tibial Artery and accompanying venae comitantes.
4. Posterior Tibial Nerve.
5. Flexor Hallucis Longus (FHL) tendon.
The tibial nerve and posterior tibial vessels pass specifically between the FDL and FHL tendons.
Clinical Pearl: Havel et al. demonstrated that the posterior tibial nerve bifurcates into the medial and lateral plantar nerves beneath the laciniate ligament in 93% of cases. Furthermore, the medial calcaneal nerve exhibits high anatomical variability, occasionally penetrating directly through the retinaculum. Failure to identify and protect these branches during surgical release is a primary cause of iatrogenic neuromas and failed TTS surgery.
Biomechanical Considerations
Daniels et al. established that a fixed valgus hindfoot deformity significantly alters the biomechanics of the tarsal tunnel. Severe hindfoot valgus increases the tensile load on the posterior tibial nerve, leading to a chronic traction neuropathy that clinically mimics or exacerbates true compressive tarsal tunnel syndrome. Any patient presenting with a talocalcaneal coalition and marked hindfoot valgus must be rigorously evaluated for secondary TTS.
Etiology and Pathogenesis
Compression of the tibial nerve may originate from extrinsic pressure, intrinsic tunnel volume reduction, or systemic conditions.
Space-Occupying Lesions
The most favorable outcomes following surgical decompression occur in patients with identifiable space-occupying lesions. These include:
* Neurilemomas (Schwannomas): Benign nerve sheath tumors that expand within the tunnel.
* Ganglion Cysts: Often arising from the adjacent tendon sheaths (e.g., FHL or FDL tenosynovitis).
* Osteophytes and Fracture Fragments: Displaced distal tibial, talar, or calcaneal fractures can mechanically encroach on the tunnel.
* Anomalous Musculature: Sammarco and Conti identified anomalous muscles within the tunnel, such as the accessory flexor digitorum longus or the tibiocalcaneus internus, as rare but significant causes of compression.
Systemic and Inflammatory Causes
- Rheumatoid arthritis and ankylosing spondylitis (causing tenosynovitis and soft-tissue hypertrophy).
- Perineural fibrosis secondary to repetitive microtrauma.
- Severe varicosities of the posterior tibial veins.
Clinical Findings and Diagnosis
The clinical presentation of TTS is highly variable, necessitating a high index of suspicion whenever a patient reports unexplained paresthesias in the plantar aspect of the foot, the toes, or the medial distal calf.
Symptomatology
- Pain and Paresthesias: Often described as burning, tingling, or numbness. Symptoms may be confined to the specific distribution of the lateral plantar nerve, medial plantar nerve, or medial calcaneal nerve.
- Exacerbating Factors: Symptoms are classically exacerbated at night, following prolonged standing or exercise, or by extreme elevation or lowering of the extremity.
- Valleix Phenomenon: Proximal radiation of pain along the course of the sciatic nerve.
Physical Examination
A meticulous physical examination is paramount. The surgeon must compare the symptomatic foot to the contralateral asymptomatic foot.
* Sensory Deficits: Look for subtle differences in temperature, sweating patterns (sudomotor changes), and skin texture. Dryness and scaliness may be isolated to the medial or lateral plantar nerve distributions.
* Motor Atrophy: Inspect for atrophy of the abductor hallucis or abductor digiti minimi. This is best observed with the patient supine, comparing the medial arches of both feet.
* Tinel's Sign: Percussion over the tibial nerve at the ankle may elicit distal paresthesias.
* Differential Diagnosis Check: Any patient with tenderness over the tibial nerve at the ankle should also be examined for an interdigital (Morton's) neuroma in the second or third web space to rule out double-crush syndrome or misdiagnosis.
Surgical Warning: Kinoshita et al. described a highly sensitive provocative maneuver: the Dorsiflexion-Eversion Test. The ankle is passively and maximally everted and dorsiflexed, while all metatarsophalangeal (MTP) joints are simultaneously maximally dorsiflexed. This position is held for 5 to 10 seconds. This maneuver maximizes tension on the nerve and decreases tunnel volume, reliably exacerbating symptoms or intensifying a Tinel's sign in affected patients.
Electrodiagnostic Studies (EMG/NCS)
Electromyography and nerve conduction studies are mandatory for any patient suspected of having TTS. While the clinical outcome of surgical release correlates poorly with the severity of electrical changes, 90% of TTS patients exhibit at least minor abnormalities.
* Motor Latencies: Distal motor latencies exceeding 6.7 ms in the lateral plantar nerve and 6.1 ms in the medial plantar nerve are highly suggestive. Latencies >7.0 ms are definitively abnormal.
* Sensory Latencies: Prolonged sensory latencies (>3.2 ms) are considered highly diagnostic.
* Needle EMG: Fibrillations, positive sharp waves, and decreased amplitude of motor action potentials in the abductor hallucis and abductor digiti minimi confirm axonal loss.
Advanced Imaging
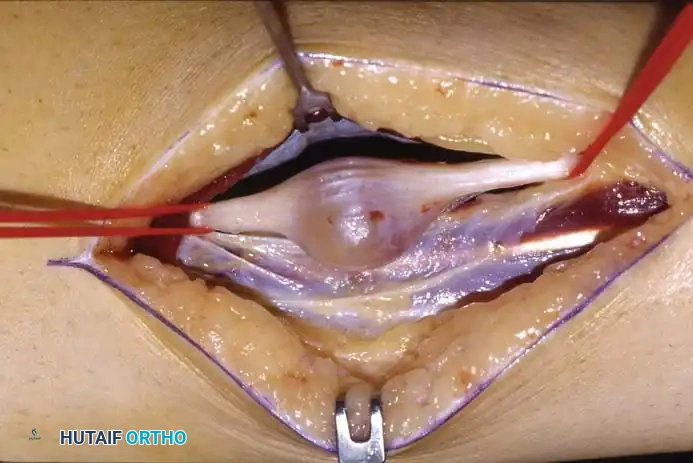
Fig 1: Axial CT scan demonstrating a well-circumscribed soft tissue mass (neurilemoma) in the posterior medial ankle.

Fig 2: Corresponding MRI clearly identifying the neurilemoma in a 40-year-old man presenting with a positive Tinel sign. Note the distinct fullness and displacement of posterior soft tissues.
Frey and Kerr demonstrated that while MRI may not always pinpoint the exact etiology of idiopathic TTS, it is invaluable for surgical planning. MRI is the gold standard for identifying space-occupying lesions, ensuring that all areas of impingement are addressed during surgical release.
Non-Operative Management
Initial management should be conservative for 6 to 12 weeks, particularly in idiopathic cases without a space-occupying lesion.
* Immobilization: Use of a rigid night splint or controlled ankle motion (CAM) boot to prevent extreme dorsiflexion and eversion.
* Pharmacotherapy: Nonsteroidal anti-inflammatory drugs (NSAIDs) and oral gabapentinoids.
* Footwear Modifications: Wide, cushioned, supportive shoes with medial arch support to correct flexible hindfoot valgus.
* Pregnancy: TTS presenting during pregnancy should be managed with rest and elevation. Symptoms frequently resolve spontaneously postpartum, mirroring the behavior of gestational carpal tunnel syndrome.
Surgical Indications and Patient Selection
Surgical decompression is indicated for patients who fail conservative management, exhibit progressive motor atrophy, or possess a confirmed space-occupying lesion.
Prognostic Factors:
Sammarco and Chang reported significant clinical improvement in patients undergoing tarsal tunnel release, noting that the highest postoperative scores occurred in patients who had symptoms for less than 1 year. Conversely, Pfeiffer and Cracchiolo cautioned that only 44% of feet benefited significantly if no distinct lesion was found.
Pitfall: Extreme caution is advised before offering surgery to:
1. Older patients (60–80 years) with idiopathic symptoms.
2. Patients with severe posttraumatic scarring within the tarsal canal.
3. Patients with systemic inflammatory disease or concomitant plantar fasciitis.
4. Patients requiring revision surgery. Schon and Myerson strongly caution against repeat release of the flexor retinaculum unless a new space-occupying lesion is definitively identified on MRI.
Surgical Technique: Tarsal Tunnel Release
Meticulous surgical technique utilizing loupe magnification and a pneumatic thigh tourniquet is essential to safely unroof the tibial nerve and its branches.
Step 1: Positioning and Incision
Place the patient supine with the hip externally rotated and the knee slightly flexed, allowing excellent access to the medial aspect of the ankle. Exsanguinate the limb and inflate the tourniquet.
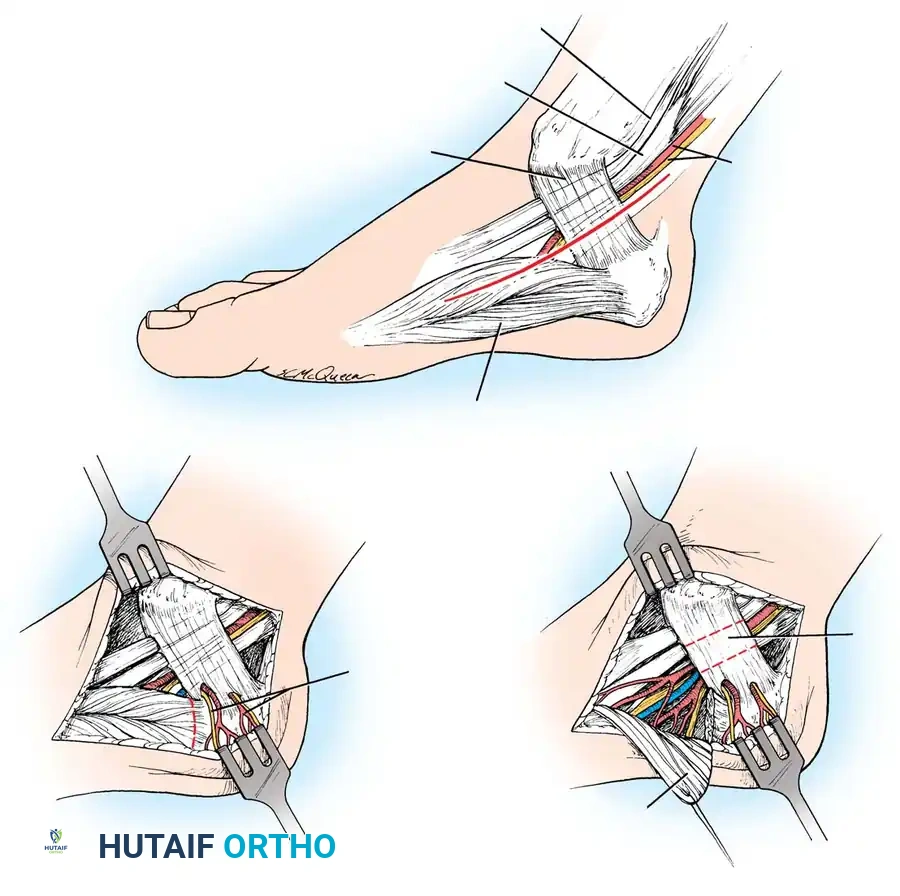
Fig 3: Surgical diagram of the Tarsal Tunnel Release. Note the trajectory of the incision and the critical relationship of the posterior tibial nerve bifurcating beneath the flexor retinaculum.
- Incision Trajectory: Begin the incision 1 cm plantar to the navicular tuberosity. Extend it proximally, bisecting the area between the medial malleolus and the medial aspect of the calcaneal tuberosity. Curve the incision gently to end 1 cm anterior to the Achilles tendon. With the foot held in gravity equinus, this forms an almost straight line.
- Tissue Handling: Do not undermine the skin edges to preserve the fragile subdermal vascular plexus.
Step 2: Superficial Dissection
- Carefully identify, coagulate, or ligate the superficial veins connecting the plantar and saphenous systems.
- Deepen the incision through the subcutaneous fat to expose the investing fascia of the calf proximally and the deep fascia of the medial foot distally.
- Identify the proximal (posterior) and distal (anterior) borders of the flexor retinaculum. Locate the neurovascular bundle proximally before it disappears beneath the retinaculum.
Step 3: Retinaculum Release and Nerve Decompression
- Proximal Release: Begin by incising 1 to 2 cm of the deep investing fascia of the calf proximal to the upper edge of the flexor retinaculum. The nerve is occasionally enlarged or pseudoneuromatous at this proximal entry point.
- Unroofing the Tunnel: Using small dissecting scissors and non-toothed forceps, release the flexor retinaculum from a proximal to a distal direction.
- Protecting the Medial Calcaneal Nerve: Exercise extreme vigilance for the medial calcaneal branch(es). These may arise from the main tibial nerve or the lateral plantar nerve and frequently penetrate directly through the retinaculum. Severing these branches will result in a debilitating, painful neuroma.
Step 4: Distal Dissection and Branch Tracking
- Continue the release distally until the muscle fibers of the abductor hallucis are reached.
- The tibial nerve will divide into the medial and lateral plantar branches. Follow both the medial and lateral plantar nerves beneath the deep fascia of the abductor hallucis muscle.
- Fascial Slings: One or both of these branches may pass through tight fascial slings as they dive into the plantar surface of the foot. These slings must be completely released to ensure total decompression.
- Manage the accompanying venae comitantes carefully; they are often numerous, engorged, and tightly intertwined with the nerve branches.
Step 5: Pathology Excision (If Applicable)

Fig 4: Gross unsectioned specimen of a neurilemoma excised from the tarsal tunnel.
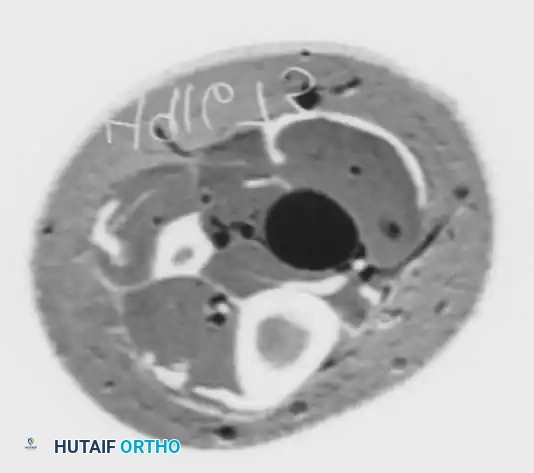
Fig 5: Intraoperative view and sectioned gross specimen. Note that while neurilemomas are nerve sheath tumors, they are intimately involved with the fascicles. Excision requires meticulous microsurgical dissection, and occasionally, a small non-functional nerve branch must be sacrificed to achieve complete removal.
If a space-occupying lesion such as a neurilemoma or ganglion is encountered, it must be carefully dissected free from the epineurium. Use microsurgical techniques to separate tumor capsules from functional nerve fascicles.
Step 6: Closure
- Deflate the tourniquet and achieve meticulous hemostasis. Hematoma formation within the unroofed tunnel is a primary cause of postoperative perineural fibrosis and failure.
- Do not repair the flexor retinaculum.
- Close the subcutaneous tissue with absorbable sutures and the skin with non-absorbable interrupted sutures or a subcuticular closure.
Postoperative Protocol
- Phase I (0-2 Weeks): The foot is placed in a bulky, compressive Jones dressing and a posterior splint in neutral dorsiflexion. The patient is strictly non-weight-bearing to allow for primary wound healing and to prevent hematoma formation.
- Phase II (2-4 Weeks): Sutures are removed at 14 days. The patient is transitioned to a CAM boot. Touch-down to partial weight-bearing is initiated. Gentle active range of motion (AROM) exercises for the ankle and toes are begun to encourage nerve gliding and prevent adherence to the surgical bed.
- Phase III (4-8 Weeks): Progressive weight-bearing as tolerated in supportive athletic footwear. Physical therapy focuses on intrinsic foot muscle strengthening, proprioception, and desensitization techniques.
- Return to Activity: Most patients can resume normal daily activities by 8 to 12 weeks, though maximal neurological recovery (especially in cases with preoperative motor atrophy) may take up to 12 to 18 months due to the slow rate of axonal regeneration (approximately 1 mm/day).
Summary
Tarsal tunnel syndrome remains a challenging clinical entity. Successful management hinges on a detailed history, precise clinical examination utilizing provocative maneuvers like the dorsiflexion-eversion test, and corroboration with EMG/NCS and MRI. Surgical intervention yields the most predictable and satisfying results in patients with identifiable space-occupying lesions or those with a short duration of symptoms. Meticulous surgical technique—ensuring complete release of the flexor retinaculum, proximal deep fascia, and distal fascial slings beneath the abductor hallucis, while rigorously protecting the medial calcaneal nerve—is the cornerstone of operative success.
You Might Also Like

