Midfoot Fractures and Dislocations: A Masterclass in Surgical Management
Key Takeaway
Midfoot fractures and dislocations, including Lisfranc and Chopart joint injuries, represent complex orthopedic challenges requiring precise anatomical reduction. This comprehensive guide details the biomechanics, classification systems, and step-by-step surgical approaches for tarsal navicular, cuboid, cuneiform, and tarsometatarsal injuries. Emphasizing rigid internal fixation and column restoration, it provides orthopedic surgeons with evidence-based protocols to optimize functional outcomes and mitigate complications like compartment syndrome and post-traumatic arthritis.
INTRODUCTION TO MIDFOOT TRAUMA
Midfoot fractures and dislocations encompass a highly complex spectrum of injuries, ranging from subtle ligamentous sprains to devastating, widely displaced fracture-dislocations. The midfoot acts as the critical transition zone between the highly mobile hindfoot and the relatively rigid forefoot, serving as the apex of the longitudinal arch. Because a significant magnitude of stress passes through this region during the stance phase of gait, injuries here are notoriously difficult to heal and are highly prone to post-traumatic arthrosis if anatomical alignment is not meticulously restored.
Historically, the incidence of severe midfoot trauma has risen sharply, correlating with the introduction and routine use of airbags in motor vehicles. Patients who previously might not have survived high-speed collisions now sustain severe blunt-force axial loading to the plantarflexed foot, frequently resulting in combined dislocations of the Chopart and Lisfranc joints.
Clinical Pearl: Early operative intervention with anatomical or near-anatomical reduction of the midfoot joints is the single most significant prognostic factor for long-term functional success. Combined Chopart and Lisfranc fracture-dislocations historically yield the lowest functional scores and demand aggressive, precise surgical management.
FRACTURES OF THE TARSAL NAVICULAR
The tarsal navicular is the keystone of the medial column. Fractures here threaten the integrity of the talonavicular joint—the primary joint responsible for hindfoot circumduction. While minimally displaced fractures can theoretically be managed in a non-weight-bearing cast, true minimal displacement is exceedingly rare.
Sangeorzan Classification and Pathoanatomy
Fractures of the tarsal navicular body are classified into three distinct types based on the Sangeorzan classification system. The primary surgical goals for displaced fractures are the restoration of articular congruity and the maintenance of medial column length.
- Type I: The fracture line occurs in the coronal plane, creating a dorsal fragment that usually consists of less than 50% of the navicular body. Anteroposterior radiographs may only show a subtle double cortical shadow at the joint line.
- Type II: The primary fracture line is sagittal or oblique. The talonavicular joint is most often subluxated dorsally and medially, accompanied by adduction of the forefoot.
- Type III: Characterized by severe comminution of the navicular body. This is frequently associated with disruption of the cuneiform-navicular joint, lateral deviation of the forefoot, and concomitant injuries to the cuboid or the anterior process of the calcaneus.





Surgical Management of Navicular Fractures
Displaced fractures of the navicular body necessitate Open Reduction and Internal Fixation (ORIF).
Surgical Approach:
1. Positioning: Supine with a bump under the ipsilateral hip to allow neutral rotation of the foot.
2. Incision: A dorsomedial approach is standard, utilizing the interval between the extensor hallucis longus (EHL) and the tibialis anterior tendon. Care must be taken to protect the medial branch of the superficial peroneal nerve and the saphenous nerve.
3. Reduction: The fracture is debrided of hematoma. A femoral distractor or external fixator may be temporarily applied between the talus and the medial cuneiform to restore medial column length and allow visualization of the articular surface.
Surgical Warning: Do not strip the plantar soft tissue attachments of the navicular, as this provides the critical remaining blood supply to the frequently avascular central third of the bone.
Fixation Techniques:
For Type I and simple Type II fractures, lag screw fixation (3.5 mm or 4.0 mm partially threaded screws) directed from dorsal to plantar or lateral to medial is often sufficient.
For Type III comminuted fractures, maintaining medial column length is paramount. Temporary bridge plating or external fixation is highly recommended. A 2.7-mm or 3.5-mm reconstruction plate can be used to span the comminuted segment, extending from the talar neck to the medial cuneiform or first metatarsal.




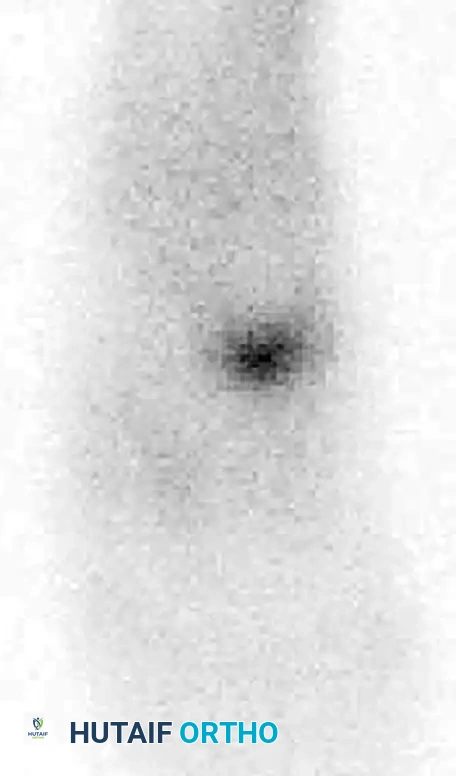
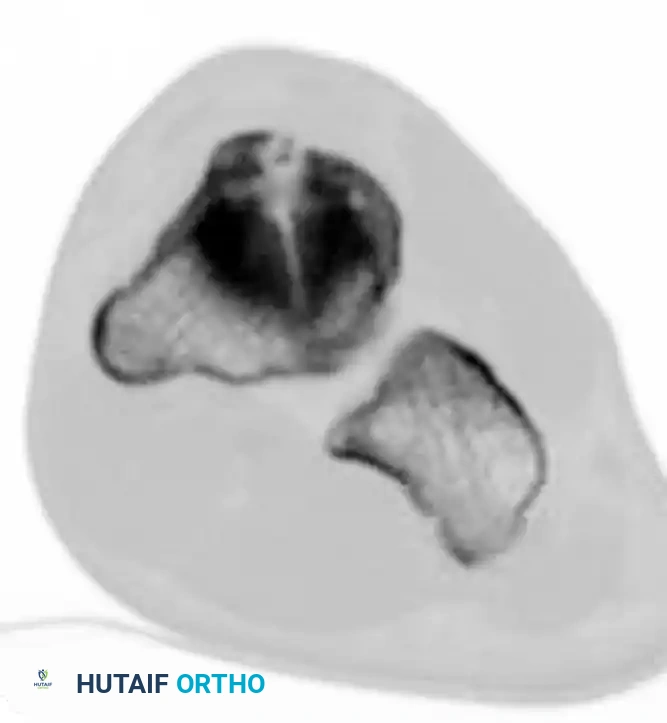
Navicular Stress Fractures
Navicular stress fractures are common in high-level running athletes. While initial radiographs may appear normal, a high index of clinical suspicion warrants advanced imaging. Bone scans and CT scans are highly sensitive for identifying these occult injuries.


CUBOID AND CUNEIFORM FRACTURES
Cuboid Fractures
Cuboid fractures are broadly classified into avulsion and compression types.
* Avulsion Fractures: Small avulsions frequently occur in conjunction with severe inversion-type ankle sprains. These generally respond well to conservative management (immobilization and protected weight-bearing).
* Compression ("Nutcracker") Fractures: These occur via forced abduction of the forefoot, crushing the cuboid between the calcaneus and the 4th/5th metatarsal bases. They are highly associated with Lisfranc and midtarsal disruptions.
Treatment Protocol:
Minimally displaced fractures can be treated in a non-weight-bearing cast for 4 weeks, followed by a weight-bearing cast for an additional 4 weeks, transitioning to a well-molded arch support.
For severe displacement resulting in shortening of the lateral column, ORIF is mandatory. Restoring lateral column length is critical to prevent a severe abduction deformity of the foot. External fixation or a femoral distractor may be necessary to pull the lateral column out to length before structural bone grafting and plate fixation can be applied.






Cuneiform Fractures
Isolated cuneiform fractures are exceedingly rare. Nonoperative treatment is reserved for strictly nondisplaced fractures. Displaced fractures require ORIF. If the cuneiform is highly comminuted, temporary bridge plating or external fixation is required to maintain the length and alignment of the medial column.
FRACTURE-DISLOCATIONS OF THE TARSOMETATARSAL (LISFRANC) JOINT
Injuries to the tarsometatarsal articulation represent a wide spectrum of pathology, ranging from subtle ligamentous sprains to widely displaced, debilitating fracture-dislocations.
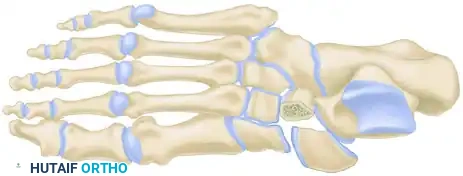
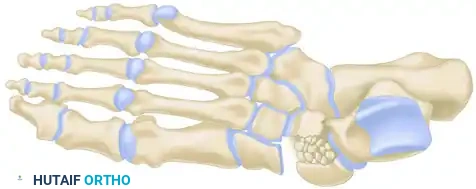
Biomechanics and Anatomy
The anatomy of the Lisfranc joint complex is unique and inherently stable due to its bony architecture. Transverse stability is provided by the Roman arch configuration of the wedge-shaped metatarsal bases and their corresponding cuneiform-cuboid articulations. The base of the second metatarsal is recessed proximally between the medial and lateral cuneiforms, acting as the "keystone" of the arch.
Longitudinal stability, however, is minimal and relies almost entirely on strong ligamentous support. Crucially, there is no intermetatarsal ligament between the first and second metatarsals. Stability in this specific interval is provided by the Lisfranc ligament, a robust oblique structure running from the plantar-lateral aspect of the medial cuneiform to the plantar-medial base of the second metatarsal.
Myerson Classification
Classification facilitates communication and helps determine the vector of displacement, though it is not strictly prognostic. Myerson’s modification of the original Quénu and Küss classification is the academic standard:
- Type A (Total Incongruity): Displacement of all five metatarsals, with or without a fracture of the second metatarsal base. Displacement is typically lateral or dorsolateral, moving as a single unit (homolateral).
- Type B (Partial Incongruity): One or more articulations remain intact.
- Type B1: Medial displacement, often involving the intercuneiform or naviculocuneiform joint.
- Type B2: Lateral displacement, which may involve the first metatarsal-cuneiform joint.
- Type C (Divergent): The first metatarsal displaces medially while the lesser metatarsals displace laterally.
- Type C1: Partial divergent.
- Type C2: Complete divergent. These are high-energy injuries associated with massive soft tissue swelling and a high risk of compartment syndrome.
Clinical Evaluation and Radiographic Parameters
Any injury resulting in midfoot tenderness, swelling, or an inability to bear weight merits rigorous evaluation.
Clinical Pearl: Careful observation of the plantar aspect of the foot is mandatory. The presence of plantar ecchymosis is highly pathognomonic for a significant Lisfranc injury until proven otherwise.
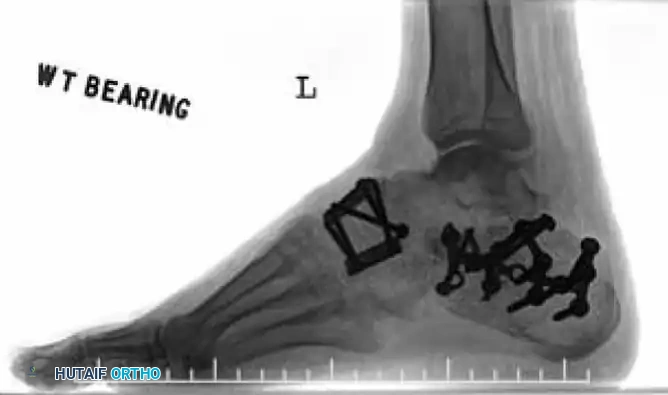
Radiographic Evaluation:
Standard non-weight-bearing radiographs often miss subtle instability. Weight-bearing radiographs are absolute requirements if the patient can tolerate them. If the patient cannot bear weight, a short-leg cast should be applied for 10-14 days, followed by repeat weight-bearing films.
Key radiographic parameters to evaluate:
1. The medial shaft of the 2nd metatarsal must align perfectly with the medial aspect of the middle cuneiform on the AP view.
2. The medial shaft of the 4th metatarsal must align perfectly with the medial aspect of the cuboid on the oblique view.
3. The 1st metatarsal-cuneiform articulation must show no incongruency.
4. The "Fleck Sign": Look for a small bony avulsion in the space between the medial cuneiform and the base of the 2nd metatarsal. This represents a bony avulsion of the Lisfranc ligament.
5. Evaluate the naviculocuneiform articulation for subtle subluxation.
If plain radiographs are equivocal but clinical suspicion remains high, CT imaging is excellent for identifying occult fractures, while MRI is the gold standard for evaluating the integrity of the Lisfranc ligament complex.
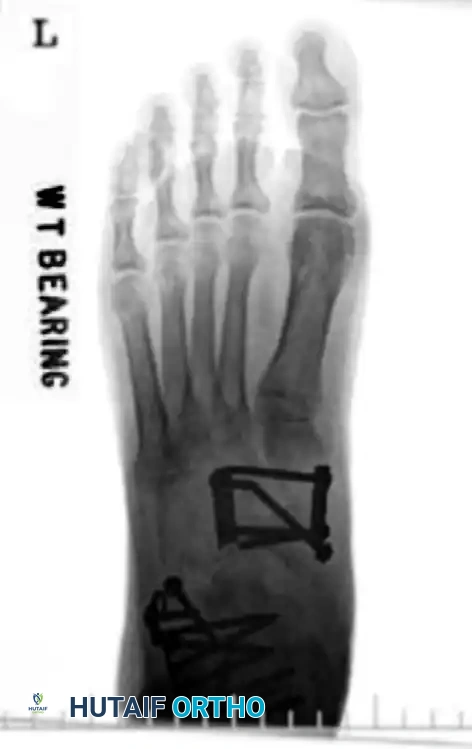
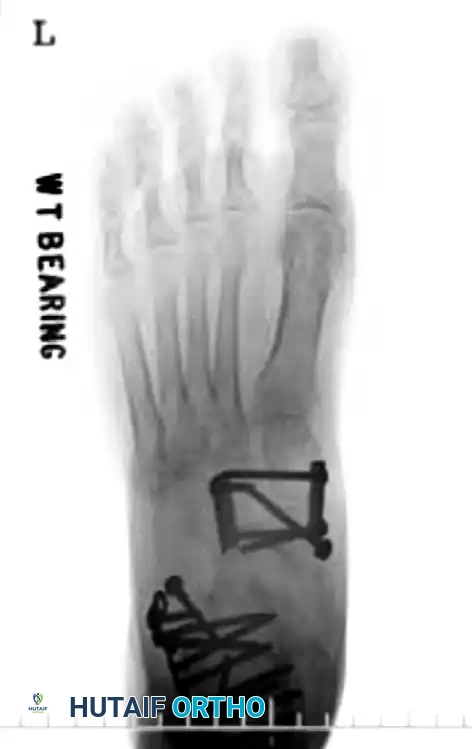
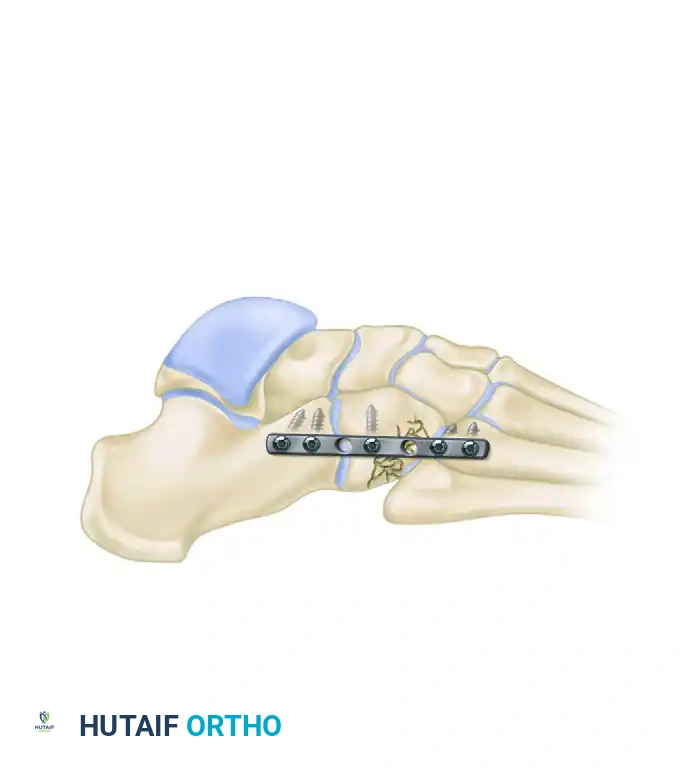
Surgical Management of Lisfranc Injuries
The absolute key to a successful outcome in Lisfranc injuries is the rigid, anatomical alignment of the involved joints.
- Nondisplaced Injuries (< 2 mm): Can be managed nonoperatively with a non-weight-bearing cast for 6 weeks, followed by a weight-bearing cast for 4 to 6 weeks. Serial radiographs are mandatory to ensure no late displacement occurs as swelling subsides.
- Displaced Injuries: Require urgent operative intervention. Closed reduction using finger traps and countertraction can be attempted to relieve soft tissue tension, but definitive ORIF is the standard of care.
Operative Technique (ORIF):
1. Incisions: A dual dorsal incision technique is standard.
* Medial Incision: Centered over the first intermetatarsal space, lateral to the EHL tendon. This exposes the 1st and 2nd TMT joints. Protect the deep peroneal nerve and dorsalis pedis artery.
* Lateral Incision: Centered over the third intermetatarsal space to access the 3rd, 4th, and 5th TMT joints.
2. Reduction Sequence: Reduction must proceed from medial to lateral. The 1st TMT joint is reduced and provisionally pinned. Next, the critical 2nd TMT joint is reduced.
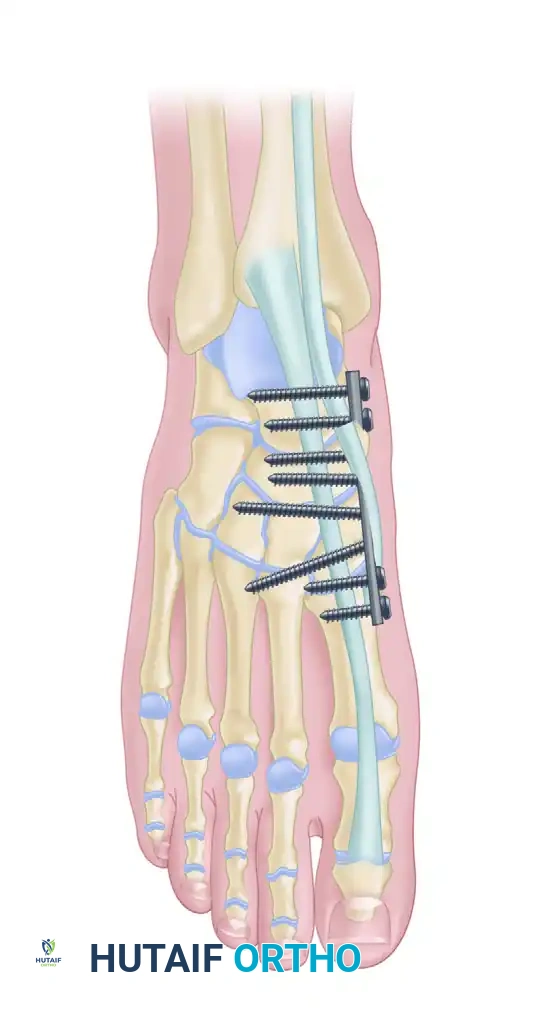
3. Fixation:
* The "Home Run Screw": A 3.5-mm or 4.0-mm solid cortical screw is placed from the medial cuneiform into the base of the second metatarsal, replicating the vector of the Lisfranc ligament.
* The 1st, 2nd, and 3rd TMT joints are typically rigidly fixed with transarticular screws or dorsal bridge plates.
* The 4th and 5th TMT joints are highly mobile. If unstable, they should be fixed with smooth Kirschner wires (K-wires) rather than rigid screws to preserve their essential sagittal plane motion. K-wires are typically removed at 6 weeks.

COMPLICATIONS: COMPARTMENT SYNDROME OF THE FOOT
Compartment syndrome of the foot is a devastating complication seen primarily with high-energy crush injuries and severe divergent (Type C) Lisfranc fracture-dislocations. Failure to recognize and decompress foot compartments leads to ischemic contracture, severe clawing of the toes, and chronic, debilitating neuropathic pain.
Pitfall: Do not rely solely on compartmental pressure monitoring in the foot. The foot contains 9 distinct anatomical compartments, making accurate pressure measurement of every compartment technically difficult and unreliable. Clinical suspicion (tense swelling, pain out of proportion, pain with passive toe stretch) is sufficient to warrant emergent fasciotomy.
Fasciotomy Technique:
We advocate for a combined medial and dorsal approach to ensure complete decompression:
1. Medial Incision: A long medial incision is utilized to decompress the abductor hallucis compartment and the deep compartments of the foot, including the calcaneal compartment.
2. Dorsal Incisions: Two dorsal longitudinal incisions are made—one between the 2nd and 3rd metatarsals, and one between the 4th and 5th metatarsals. These effectively decompress the dorsal intrinsic compartments (interossei).
Wounds are left open, managed with negative pressure wound therapy (NPWT), and closed via delayed primary closure or split-thickness skin grafting once swelling has adequately subsided.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of midfoot trauma requires strict adherence to biological healing timelines.
* 0-2 Weeks: The patient is placed in a bulky Jones splint, strictly non-weight-bearing, with strict elevation to manage edema.
* 2-6 Weeks: Sutures are removed. The patient is transitioned to a short-leg cast or rigid CAM boot. Strict non-weight-bearing is maintained. K-wires (if used for the lateral column) are removed at the 6-week mark in the clinic.
* 6-12 Weeks: Progressive weight-bearing is initiated in a CAM boot. Physical therapy begins, focusing on active range of motion of the ankle, hindfoot, and forefoot.
* 3-6 Months: Transition to supportive athletic footwear with a custom-molded rigid orthotic or carbon fiber insert to support the longitudinal arch and limit stress across the midfoot joints.
Patients must be extensively counseled regarding the long-term prognosis. Even with perfect anatomical reduction, post-traumatic arthritis of the midfoot joints is common. Furthermore, studies indicate that a significant percentage of patients with severe midfoot fracture-dislocations may not return to their pre-injury levels of athletic activity or heavy labor for up to 2 years post-injury. If severe post-traumatic arthritis develops, midfoot arthrodesis remains a highly effective salvage procedure.
===```
You Might Also Like
