Midfoot Arthritis and Arthrodesis: A Comprehensive Surgical Guide
Key Takeaway
Midfoot arthritis frequently develops as a sequela of Lisfranc injuries or primary degeneration. Successful management requires a deep understanding of midfoot biomechanics, precise clinical evaluation using provocative maneuvers like the piano key test, and targeted diagnostic injections. When conservative measures fail, midfoot arthrodesis with meticulous joint preparation, deformity correction, and rigid internal fixation provides reliable pain relief and functional restoration.
INTRODUCTION TO MIDFOOT ARTHRITIS
Arthritis of the midfoot is a frequently encountered clinical entity, yet high-level literature specific to its isolated management remains relatively limited. The vast majority of the existing literature relates to treating the sequelae of missed or inadequately treated Lisfranc fracture-dislocations. Posttraumatic arthritis in this region typically presents in a younger, more active demographic compared to atraumatic, primary osteoarthritis or inflammatory arthropathies.
The midfoot serves as a critical biomechanical transition zone. It is a fairly rigid segment that connects the highly mobile hindfoot (which accommodates uneven terrain) to the mobile forefoot (which facilitates propulsion). Disruption of this rigid segment, whether through trauma, neuropathic collapse (Charcot arthropathy), or progressive degeneration, leads to profound functional impairment, altered gait mechanics, and debilitating pain.
ANATOMY AND BIOMECHANICS
A profound understanding of midfoot anatomy is paramount for both accurate diagnosis and successful surgical reconstruction. The tarsometatarsal (TMT) joint complex is anatomically divided into three distinct columns:
* Medial Column: Comprises the first metatarsal and the medial cuneiform.
* Middle Column: Comprises the second and third metatarsals articulating with the middle and lateral cuneiforms, respectively.
* Lateral Column: Comprises the fourth and fifth metatarsals articulating with the cuboid.
The Roman Arch and the Lisfranc Complex
The osseous architecture of the midfoot is inherently stable due to the trapezoidal shape of the cuneiforms and metatarsal bases, which form a transverse "Roman arch." The keystone of this arch is the base of the second metatarsal, which is recessed proximally between the medial and lateral cuneiforms, locking the complex in place.
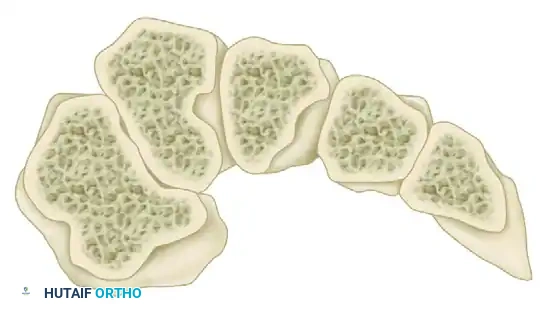
FIGURE 84-14: Coronal section through the metatarsal bases illustrating the Roman arch configuration.
Soft tissue stability is primarily conferred by the Lisfranc ligament complex. The true Lisfranc ligament consists of three components (dorsal, interosseous, and plantar bands) that course from the lateral aspect of the medial cuneiform to the medial base of the second metatarsal. The interosseous band is the thickest and strongest, providing significant stability to the medial and middle columns. Notably, there is no direct ligamentous connection between the bases of the first and second metatarsals.
Kinematics of the Lateral Column
Despite the relative lack of mobility in the medial and middle columns of the midfoot, the lateral column is highly dynamic. The arc of motion in the fourth and fifth TMT joints is approximately 20 degrees in the sagittal plane. This mobility is essential for proper biomechanics, allowing the foot to accommodate uneven ground during the stance phase of gait.
Clinical Pearl: Preservation of the fourth and fifth tarsometatarsal joints should be considered a surgical priority. Fusion of these joints results in a rigidly fixed lateral column, which alters normal gait kinematics and increases stress on adjacent joints. Even in the presence of severe radiographic arthritis, the lateral column is often asymptomatic.
CLINICAL EVALUATION
Examination of the arthritic midfoot is notoriously difficult. The joints are small, tightly packed, and possess limited physiological motion, making the differentiation of the exact pain generator a significant clinical challenge.
Patients typically present with vague, deep, aching midfoot pain that is exacerbated by weight-bearing and push-off. On physical examination, there may be a palpable dorsal exostosis (osteophyte formation) and localized tenderness. However, provocative maneuvers about the midfoot often cause diffuse pain rather than pinpointing a single joint.
The "Piano Key" Test
To isolate pathology within specific TMT rays, Keiserman et al. described the "piano key" test. In this maneuver, the examiner stabilizes the hindfoot and midfoot with one hand while grasping the individual metatarsal head with the other. Pushing the metatarsal head in a plantar and dorsal direction causes a cantilever stress at the corresponding tarsometatarsal joint. Reproduction of sharp, localized pain indicates pathology at that specific TMT articulation.

FIGURE 84-15: “Piano key” test for evaluation of midfoot.
Assessing Deformity
Midfoot arthritis, particularly posttraumatic or neuropathic, often leads to a predictable pattern of structural collapse. The examiner must evaluate for:
* Forefoot Abduction: Due to lateral subluxation of the TMT joints.
* Midfoot Pronation: Loss of the medial longitudinal arch.
* Dorsiflexion Deformity: Resulting in a rocker-bottom foot and potential plantar ulceration.
Hindfoot deformity (such as valgus collapse) frequently accompanies a midfoot pathological process. The hindfoot must be carefully evaluated; if a significant hindfoot deformity is present, it must be addressed surgically to prevent premature failure of the midfoot reconstruction.
RADIOGRAPHIC AND DIAGNOSTIC EVALUATION
Standard Radiography
Anteroposterior (AP), lateral, and oblique radiographs of the foot must be obtained in a strictly weight-bearing position. Non-weight-bearing films are inadequate for assessing joint space narrowing, dynamic instability, and the true extent of the deformity.
* AP View: Assesses the alignment of the medial border of the second metatarsal with the medial border of the middle cuneiform.
* Oblique View: Assesses the alignment of the medial border of the fourth metatarsal with the medial border of the cuboid.
* Lateral View: Evaluates the sagittal alignment (Meary's angle), dorsal osteophyte formation, and the presence of a flatfoot or rocker-bottom deformity.
Advanced Imaging and Diagnostic Injections
Computed Tomography (CT) is highly useful for delineating the exact joints involved, assessing bone stock, and planning deformity correction. While standard CT provides excellent bony detail, weight-bearing CT (if available) is the gold standard, as it simulates physiological load.
Because clinical examination and imaging may not definitively isolate the symptomatic joints, differential injections using a local anesthetic are an invaluable diagnostic tool. These injections should be performed under fluoroscopic or CT guidance to ensure precise intra-articular placement.
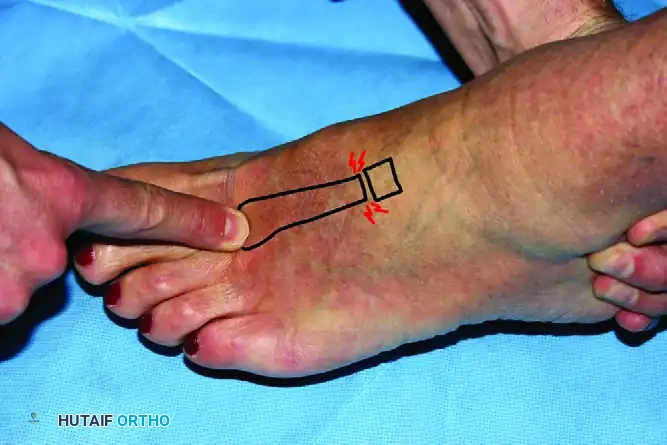
FIGURE 84-16: CT-guided differential injection can be helpful in the diagnosis of midfoot arthritis.
Surgical Warning: Adding a corticosteroid to the diagnostic injection may provide therapeutic relief, but surgery should be delayed for at least 3 months following a steroid injection to mitigate the risk of postoperative infection.
NON-OPERATIVE MANAGEMENT
Conservative treatment is the first-line approach for midfoot arthritis and can provide substantial relief, particularly in older, lower-demand patients. The goal is to restrict motion through the arthritic joints and offload the midfoot.
Orthoses and Shoe Modifications
Shoe modifications are highly effective. Rocker soles on extra-depth, stiff-soled shoes reduce the bending moment across the midfoot during the terminal stance phase of gait. Accommodative inserts can distribute plantar pressures evenly, which is especially critical if a plantar prominence has developed.

FIGURE 84-17: Extra-depth stiff shoes with rocker soles can be effective nonoperative treatment for midfoot arthritis.
For more advanced arthritis or significant deformity, an ankle-foot orthosis (AFO) can be utilized. A custom-molded solid AFO or a double-upright brace bypasses the midfoot entirely, transferring load from the proximal calf directly to the shoe, thereby supporting the longitudinal arch and eliminating midfoot stress.

FIGURE 84-18 A: For more advanced arthritis, an ankle-foot orthosis, such as this double-upright brace, can be used for support of the longitudinal arch.

FIGURE 84-18 B: Lateral view of the double-upright brace demonstrating rigid support.
Additional conservative measures include:
* Activity modification (avoiding high-impact activities).
* Nonsteroidal anti-inflammatory drugs (NSAIDs).
* Physical therapy focusing on Achilles tendon stretching, as a tight heel cord exacerbates midfoot loading.
SURGICAL INDICATIONS AND PREOPERATIVE PLANNING
Surgery is indicated for patients with debilitating pain and functional limitation in whom exhaustive conservative management has failed. Midfoot arthritis often progresses, and as deformity worsens, surgical intervention becomes necessary not only to relieve pain but to restore a plantigrade, braceable foot.
Joint Selection for Arthrodesis
Preoperative planning is heavily reliant on identifying the symptomatic joints via physical examination and differential injections.
* Medial and Middle Columns: These are the most frequently fused joints. If the first TMT joint is fused, the surgeon must evaluate the navicular-medial cuneiform joint. If it exhibits arthritic changes, it should be included in the fusion mass to prevent adjacent segment disease.
* Intercuneiform Joints: If both the first and second TMT joints are fused, the medial-middle intercuneiform joint must be included in the arthrodesis. Failure to do so leaves an isolated, unstable articulation that will inevitably become symptomatic.
* Lateral Column: As previously stated, preservation is desirable. However, in the setting of severe deformity, instability, or a neuropathic foot (Charcot), fusion of the fourth and fifth TMT joints may be required to achieve a stable, plantigrade foot.
Controversy in Lateral Column Management: In an attempt to avoid arthrodesis of a painful lateral column, techniques for arthroplasty have been devised, including tendon interposition arthroplasty and spherical ceramic interpositional arthroplasty. Despite reluctance to fuse the lateral midfoot, literature shows that good results can be achieved after arthrodesis of the fourth and fifth TMT joints. While most successful reports involve neuropathic patients, pain and AOFAS scores also improve significantly in patients with normal sensation following lateral column fusion.
Deformity Correction
A major area of historical controversy is whether to reduce midfoot deformity before fusion or simply fuse the foot in situ. Modern orthopedic consensus strongly dictates that deformity correction is a priority. Midfoot arthritis often leads to an abduction, pronation, and dorsiflexion deformity. Most contemporary studies suggest vastly superior functional results and lower nonunion rates with improved alignment and restoration of normal bony architecture.
SURGICAL TECHNIQUE: MIDFOOT ARTHRODESIS
Positioning and Approach
- Positioning: The patient is placed supine on the operating table with a bump under the ipsilateral hip to internally rotate the leg to a neutral position. A thigh tourniquet is applied.
- Incision Strategy: Access to the TMT joints is typically achieved via two longitudinal dorsal incisions.
- Medial Incision: Placed over the first intermetatarsal space, lateral to the extensor hallucis longus (EHL) tendon. This provides access to the 1st and 2nd TMT joints, as well as the medial-middle intercuneiform joint.
- Lateral Incision: Placed over the third metatarsal, providing access to the 3rd TMT joint (and 4th/5th if lateral column fusion is indicated).
- Neurovascular Protection: The deep peroneal nerve and dorsalis pedis artery course between the first and second metatarsals. Meticulous dissection is required to identify and retract this neurovascular bundle, usually laterally, to prevent catastrophic ischemic or neuropathic complications.
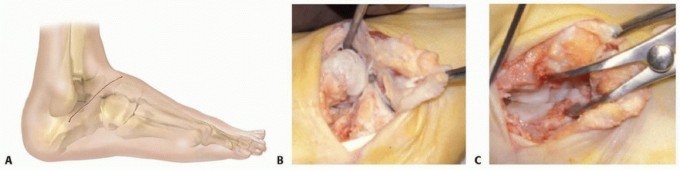
Joint Preparation
The success of any arthrodesis relies on meticulous joint preparation.
1. Exposure: The joint capsules are incised longitudinally and elevated via subperiosteal dissection.
2. Cartilage Removal: All articular cartilage is removed using curettes, osteotomes, and rongeurs. The subchondral bone plate must be completely denuded down to bleeding cancellous bone.
3. Deformity Correction: If a planovalgus or abduction deformity exists, the joint surfaces are contoured using a saw or sharp osteotomes. Plantar-flexion wedges may be removed from the dorsal aspect of the cuneiforms to correct a dorsiflexion (rocker-bottom) deformity.
4. Fenestration: The opposing bony surfaces are fenestrated with a 2.0mm drill bit or a small osteotome to stimulate osteogenesis and vascular ingrowth.
Fixation Strategies
Multiple methods of fixation have been utilized for tarsometatarsal arthrodesis. The choice depends on the specific joints involved, bone quality, and the presence of deformity.
- Crossed Solid Screws: The traditional gold standard. 3.5mm or 4.0mm fully threaded solid cortical screws are utilized. A "home run" screw is typically placed from the medial cuneiform into the base of the second metatarsal, recreating the biomechanical vector of the Lisfranc ligament.
- Plating:
- Plantar Plating: Biomechanically superior as it is applied to the tension side of the midfoot, preventing dorsal gapping. However, the surgical approach is highly demanding and carries a risk to the plantar neurovascular structures.
- Dorsal Plating: Frequently used in modern practice. Low-profile, pre-contoured locking plates provide excellent stability, especially when combined with an interfragmentary compression screw.
- External Fixation: Generally not recommended for routine midfoot arthrodesis due to pin tract infections and patient non-compliance. It is strictly reserved for cases complicated by active plantar ulceration, severe Charcot arthropathy, or active infection where internal hardware is contraindicated.
Bone Grafting
If structural defects exist following deformity correction, or if the patient has risk factors for nonunion (e.g., smoking, diabetes), autologous bone graft (typically harvested from the proximal tibia or iliac crest) or orthobiologics (demineralized bone matrix, bone morphogenetic proteins) should be packed into the arthrodesis sites prior to final compression.
POSTOPERATIVE PROTOCOL
Strict adherence to postoperative rehabilitation protocols is critical to prevent hardware failure and nonunion.
- Phase I (0-2 Weeks): The patient is placed in a well-padded short leg splint and remains strictly non-weight-bearing (NWB). Elevation is paramount to control edema and ensure wound healing.
- Phase II (2-6 Weeks): Sutures are removed at 2 weeks. The patient is transitioned to a short leg cast or a rigid fracture boot. Strict NWB status is maintained.
- Phase III (6-10 Weeks): Radiographs are obtained at 6 weeks. If there is evidence of early consolidation, the patient may begin progressive partial weight-bearing in a CAM boot.
- Phase IV (10-12+ Weeks): Transition to regular footwear, utilizing a stiff-soled shoe or a carbon fiber insert to protect the midfoot during the final stages of remodeling. Full unrestricted activity is generally not permitted until 4 to 6 months postoperatively, pending radiographic confirmation of solid fusion.
COMPLICATIONS
- Nonunion: The most common complication, occurring in 5% to 10% of cases. Risk factors include smoking, inadequate joint preparation, and failure to correct deformity. Asymptomatic nonunions may be observed; symptomatic nonunions require revision with bone grafting and robust fixation.
- Malunion: Failure to restore the longitudinal arch or correct forefoot abduction leads to altered plantar pressures, potentially resulting in transfer metatarsalgia or ulceration.
- Hardware Irritation: Due to the paucity of dorsal soft tissue coverage, dorsal plates and screw heads frequently become prominent and painful, necessitating hardware removal after solid fusion is achieved (typically after 1 year).
- Adjacent Segment Disease: Fusion of the midfoot increases stress on the naviculocuneiform and metatarsophalangeal joints, which may accelerate arthritic degeneration in these areas over time.
You Might Also Like