Operative Management of Lisfranc and Fifth Metatarsal Fractures: A Masterclass in Midfoot Trauma
Key Takeaway
The operative management of tarsometatarsal (Lisfranc) fracture-dislocations and fifth metatarsal base fractures requires meticulous surgical technique and rigid fixation. This guide details the anatomic approaches, neurovascular protection, and step-by-step reduction strategies for Lisfranc injuries, alongside evidence-based intramedullary screw fixation protocols for Jones fractures. Mastery of these techniques ensures optimal biomechanical restoration, minimizes post-traumatic arthrosis, and accelerates return to function in both standard and high-demand athletic populations.
Introduction to Midfoot Trauma
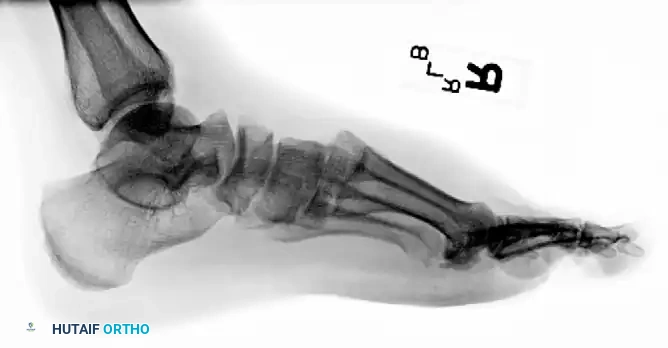
The midfoot serves as the critical biomechanical transition zone between the rigid hindfoot and the flexible forefoot. Injuries to this region, particularly tarsometatarsal (Lisfranc) fracture-dislocations and proximal fifth metatarsal fractures, present significant challenges to the orthopaedic surgeon. Missed diagnoses or inadequate reductions inevitably lead to post-traumatic arthrosis, midfoot collapse, and profound functional disability.
This comprehensive guide delineates the textbook-level, evidence-based operative management of these complex injuries. It provides a step-by-step architectural blueprint for surgical approaches, neurovascular protection, reduction sequencing, and rigid internal fixation, tailored for orthopaedic residents, fellows, and practicing consultants.
Part I: Lisfranc (Tarsometatarsal) Fracture-Dislocations
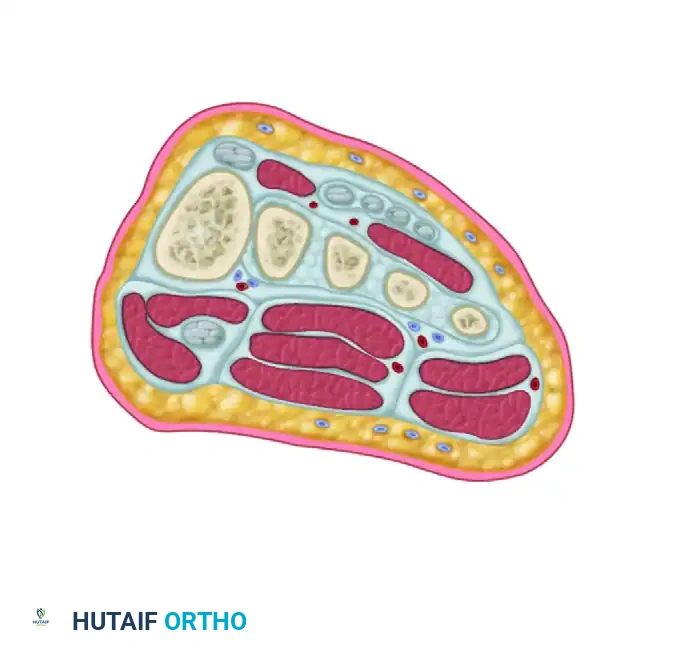
Anatomy and Biomechanics
The stability of the tarsometatarsal (TMT) joint complex relies on both its intrinsic bony architecture and a robust ligamentous network. The base of the second metatarsal is recessed proximally between the medial and lateral cuneiforms, creating a "keystone" configuration that locks the midfoot.
Crucially, there is no transverse ligament connecting the bases of the first and second metatarsals. The primary stabilizing structure is the Lisfranc ligament, a thick, oblique interosseous band originating from the lateral aspect of the medial cuneiform and inserting onto the medial base of the second metatarsal. Disruption of this ligament, either through direct crush injuries or indirect axial loading on a plantarflexed foot, leads to catastrophic destabilization of the medial column.
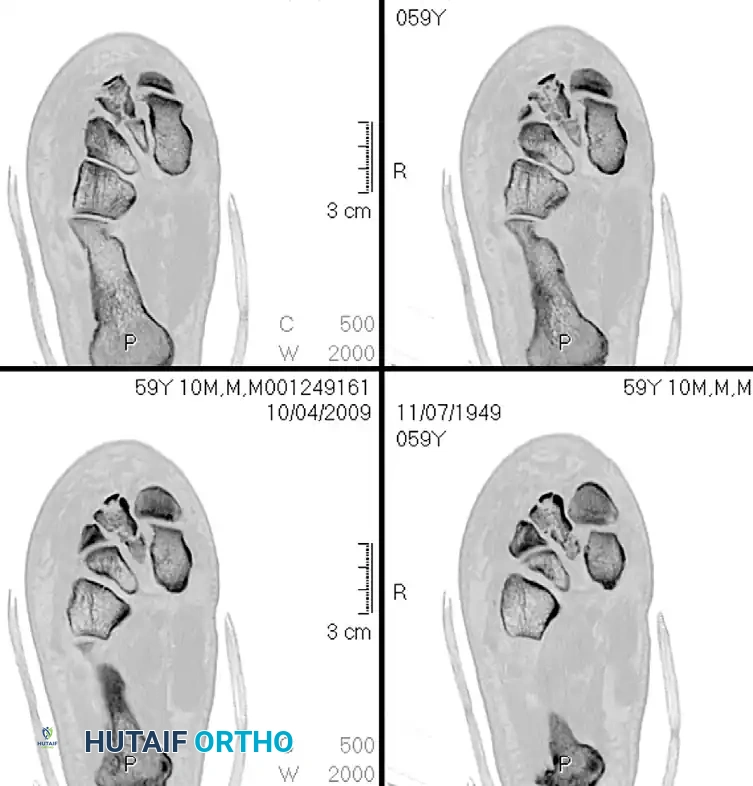
Clinical Pearl: Up to 20% of Lisfranc injuries are missed on initial emergency department evaluation. Always maintain a high index of suspicion in patients presenting with midfoot pain, plantar ecchymosis, and inability to bear weight following a twisting injury or axial load. Weight-bearing radiographs or stress fluoroscopy are mandatory if the clinical suspicion is high but static non-weight-bearing films are negative.
Classification of Tarsometatarsal Injuries
The Myerson modification of the Quenu and Kuss classification system remains the standard for categorizing Lisfranc fracture-dislocations. While it does not strictly dictate the surgical approach, it provides a vital framework for understanding the energy of the injury and the pattern of displacement.
- Type A (Total Incongruity): Displacement of all five metatarsals in a single direction (usually lateral or dorsolateral).
- Type B (Partial Incongruity):
- Type B1: Medial displacement of the first metatarsal, with the lesser metatarsals remaining anatomically aligned.
- Type B2: Lateral displacement of one or more of the lesser metatarsals, with the first metatarsal remaining intact.
- Type C (Divergent):
- Type C1 (Partial): Divergent displacement of the first metatarsal medially and some of the lesser metatarsals laterally.
- Type C2 (Total): Divergent displacement of the first metatarsal medially and all four lesser metatarsals laterally.









Indications for Operative Intervention
Non-operative management is strictly reserved for truly non-displaced injuries (less than 2 mm of displacement on weight-bearing views) with no evidence of dynamic instability.
Absolute indications for Open Reduction and Internal Fixation (ORIF) include:
* Any displacement > 2 mm at any TMT joint.
* Talar-first metatarsal angle > 15 degrees.
* Evidence of bony avulsion of the Lisfranc ligament (fleck sign).
* Open fractures or impending compartment syndrome of the foot.
Surgical Approach and Neurovascular Protection
Proper exposure is paramount. Closed reduction and percutaneous pinning are generally discouraged due to the high likelihood of interposed soft tissue (e.g., anterior tibial tendon, peroneus longus tendon, or fracture fragments) blocking anatomic reduction.
The Dual Incision Technique
A two-incision approach is the gold standard for comprehensive visualization of the TMT complex.
- Dorsomedial Incision: Centered over the first intermetatarsal space. This provides access to the first and second TMT joints, as well as the medial intercuneiform joint.
- Neurovascular Warning: At the distal extent of the excision, meticulously preserve the most medial branch of the dorsal medial cutaneous nerve (superficial peroneal nerve).
- Dorsolateral Incision: A second incision is frequently required if open reduction of the third, fourth, and fifth TMT joints is necessary. This is placed over the third intermetatarsal space.
- Surgical Pitfall: Ensure an adequate skin bridge (minimum 5-7 cm) between the two incisions to prevent catastrophic skin necrosis.




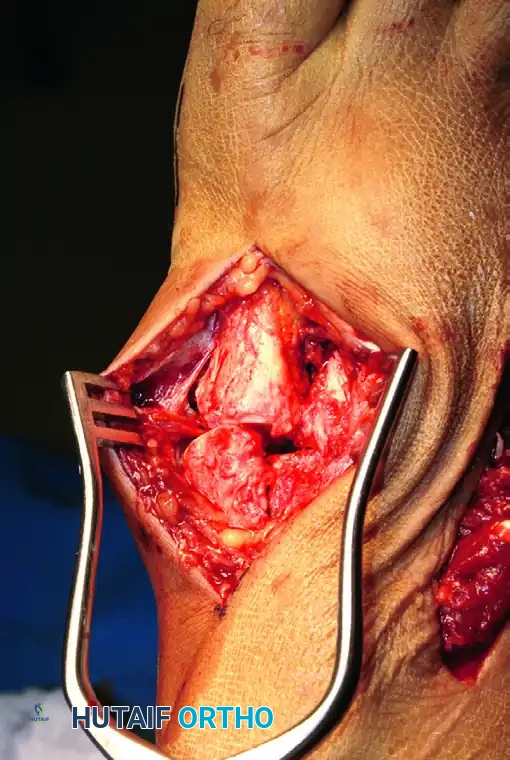
Deep Dissection and Compartment Release
- Locate and incise the inferior extensor retinaculum.
- Critical Step: Isolate the dorsalis pedis artery and the deep peroneal nerve. These structures run directly over the second TMT joint. Use a vessel loop to gently retract these structures medially or laterally. This allows safe, unhindered inspection of the Lisfranc interval.
- In cases of high-energy crush injuries, prophylactic release of the fascial compartments of the forefoot may be necessary to prevent compartment syndrome.







Step-by-Step Reduction and Fixation
The sequence of reduction is critical. The midfoot must be rebuilt from medial to lateral, establishing a stable medial column before addressing the lateral rays.
1. Debridement and Preparation
Remove any osteochondral debris, hematoma, or interposed soft tissue from the Lisfranc region between the base of the second metatarsal and the medial cuneiform. Failure to clear this space will preclude an anatomic reduction.
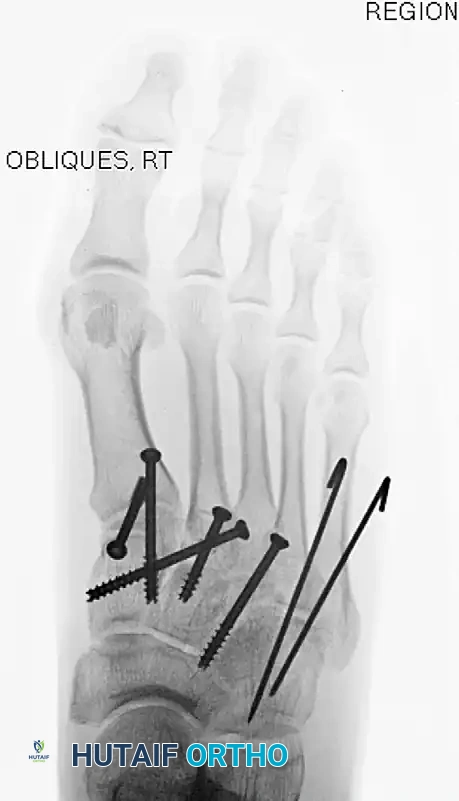
2. Medial Column Reduction (1st TMT)
- Reduce the first tarsometatarsal joint anatomically.
- Hold the reduction provisionally with K-wires or a pointed reduction clamp.
- Place a 4.0-mm cannulated or solid cortical screw from the dorsal aspect of the first metatarsal base into the medial cuneiform. A second screw can be placed from proximal to distal across the joint for rotational stability.
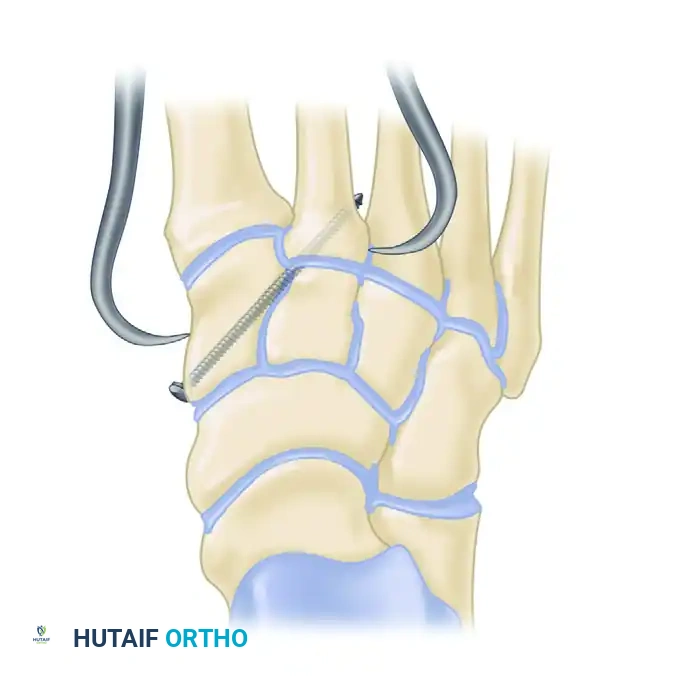
3. The "Homerun" Screw (Lisfranc Articulation)
- Under fluoroscopic guidance, reduce the second metatarsal base into its keystone slot between the cuneiforms. Hold this with a towel clip or reduction forceps.
- Pass a guidewire from the medial aspect of the medial cuneiform, aiming laterally and distally into the base of the second metatarsal. This trajectory mimics the native Lisfranc ligament.
- Overdrill and place an appropriate 4.0-mm or 4.5-mm cannulated screw over the guidewire to compress the interval.


4. Central Column Fixation (2nd and 3rd TMT)
- The second and third metatarsal-cuneiform joints are reduced and fixed similarly, typically with a single screw across each joint from dorsal-distal to plantar-proximal.
- If an intercuneiform screw is needed to stabilize the cuneiform complex, insert it under fluoroscopic guidance from the medial side of the medial cuneiform into the middle cuneiform.
5. Managing Comminution: The Role of Dorsal Plating
Occasionally, severe bony comminution at the TMT joints precludes the use of transarticular screws, as compression would lead to shortening and deformity. Furthermore, transarticular screws inherently damage the articular cartilage.
* In cases of comminution or purely ligamentous injuries, fixation is best accomplished with dorsal bridge plates.
* These plates span the joint, maintaining length and alignment without violating the articular surface.



6. Lateral Column Stabilization (4th and 5th TMT)
The fourth and fifth TMT joints are highly mobile and essential for accommodating uneven terrain. Rigid screw fixation here is contraindicated as it leads to stiffness and hardware failure.
* Reduce lateral metatarsocuboid disruptions either closed or open through the dorsolateral incision.
* Fix provisionally with smooth K-wires (Steinmann pins) driven from the metatarsals into the cuboid. These are left protruding or buried just under the skin for easy removal at 6 weeks.



Subtle Lisfranc Injuries
Subtle, purely ligamentous injuries can be deceptive. Diastasis of >2mm between the 1st and 2nd metatarsal bases on weight-bearing views demands fixation. Dorsal plating is increasingly favored for these subtle injuries to avoid iatrogenic cartilage damage.




Postoperative Care and Hardware Removal
- Immediate Post-op: Close the dorsal skin with interrupted nylon sutures. Apply a bulky Jones dressing and a posterior splint.
- 7 to 10 Days: Convert to a short-leg, strictly non-weight-bearing cast.
- 6 to 8 Weeks: Remove laterally placed Steinmann pins in the clinic. Weight-bearing in a CAM boot may be initiated depending on radiographic healing.
- 4 to 5 Months: Medial transarticular screws are typically removed prior to full, unrestricted athletic activity to prevent hardware breakage, though dorsal plates may be left in place unless symptomatic.
**
You Might Also Like

