Mastering the Surgical Management of Haglund Deformity and Retrocalcaneal Bursitis
Key Takeaway
Haglund deformity, often termed a "pump bump," involves an osseous prominence of the posterosuperior calcaneal tuberosity complicated by retrocalcaneal and superficial pretendinous bursitis. When conservative measures fail, surgical intervention via calcaneal exostectomy and bursectomy is indicated. In cases with extensive Achilles tendon degeneration requiring greater than 50% detachment, flexor hallucis longus (FHL) tendon transfer is recommended to restore plantar flexion strength and prevent postoperative rupture.
PATHOPHYSIOLOGY AND CLINICAL BIOMECHANICS
Haglund deformity, colloquially referred to as a "pump bump," represents a complex triad of pathologies involving an abnormal osseous prominence of the posterosuperior calcaneal tuberosity, retrocalcaneal bursitis, and superficial pretendinous Achilles bursitis. Understanding the intricate anatomy of the Achilles tendon insertion is paramount for the orthopedic surgeon evaluating and treating this condition.
The Achilles tendon lacks a true synovial sheath; instead, it is enveloped by a paratenon that supplies its vascularity, particularly in the watershed area 2 to 6 cm proximal to its insertion. At the insertion site, two distinct bursae dictate the clinical pathology:
1. The Retrocalcaneal Bursa: A constant, anatomically native bursa situated between the anterior aspect of the distal Achilles tendon and the posterosuperior calcaneal tuberosity. It serves to reduce friction during ankle dorsiflexion.
2. The Superficial Pretendinous Bursa: An adventitious bursa that develops between the posterior aspect of the Achilles tendon and the overlying skin. According to anatomical studies by Jones, this bursa is present in approximately 50% of patients and forms primarily as a physiological response to chronic external friction.
The etiology of Haglund syndrome is predominantly mechanical. Chronic irritation from a rigid shoe heel counter (hence "pump bump") compresses the superficial bursa, the Achilles tendon, and the retrocalcaneal bursa against the prominent posterosuperior calcaneus. This repetitive microtrauma leads to chronic inflammation, bursal hypertrophy, and eventually, insertional Achilles tendinopathy with intratendinous calcification.
Demographically, this deformity occurs most frequently in young women in their 20s and 30s, correlating strongly with the use of restrictive, rigid-heeled footwear.
Clinical Pearl: Differentiating pure Haglund deformity with retrocalcaneal bursitis from advanced insertional Achilles tendinopathy is critical for prognostication. Watson, Anderson, and Davis reported a significantly higher patient satisfaction rate and a shorter time to maximal clinical improvement in patients treated for isolated retrocalcaneal bursitis and Haglund deformity compared to those requiring extensive debridement for insertional Achilles tendinitis.
PREOPERATIVE EVALUATION AND INDICATIONS
Clinical Assessment
Patients typically present with posterior heel pain that is exacerbated by walking, running, or wearing closed-heel shoes. Physical examination reveals a palpable, often erythematous, osseous prominence at the posterolateral aspect of the heel. Tenderness is usually localized anterior to the Achilles tendon (elicited by the two-finger squeeze test of the retrocalcaneal bursa) rather than within the tendon substance itself, though concomitant tendinopathy may blur these lines.
Radiographic Templating
Standard weight-bearing radiographs (lateral, AP, and axial calcaneal views) are mandatory. On the lateral radiograph, the surgeon should evaluate:
* Fowler-Philip Angle: An angle greater than 75 degrees suggests a pathological posterosuperior prominence.
* Parallel Pitch Lines (Chauveaux-Liet): A more reliable indicator where the osseous prominence extends superior to the upper parallel pitch line.
* Intratendinous Calcification: Indicates chronic degenerative tendinopathy, which will dictate the extent of surgical debridement.
Magnetic Resonance Imaging (MRI) is highly recommended if the surgeon suspects significant intrasubstance Achilles degeneration, as this will determine the need for tendon detachment, debridement, and potential flexor hallucis longus (FHL) augmentation.
Surgical Indications
Surgery is infrequently required as the first line of treatment. Modification of shoe wear (open-heeled shoes), heel lifts to plantarflex the ankle and decompress the retrocalcaneal space, nonsteroidal anti-inflammatory drugs (NSAIDs), and targeted physical therapy usually relieve symptoms.
Surgical intervention is strictly indicated only after the exhaustion of conservative measures (typically 3 to 6 months of compliant non-operative management).
SURGICAL TECHNIQUE: CALCANEAL EXOSTECTOMY AND BURSECTOMY
The following technique is the gold standard for addressing Haglund deformity when conservative measures fail.
Positioning and Anesthesia
- Anesthesia: The procedure can be performed under general anesthesia or regional anesthesia (popliteal block) combined with intravenous sedation.
- Positioning: Place the patient in the prone position. Ensure all bony prominences are well-padded.
- Tourniquet: Apply a thigh or calf tourniquet to provide a bloodless surgical field, inflating it after exsanguination of the limb.
Surgical Approach
- Make a longitudinal lateral incision approximately 1 cm lateral to the lateral border of the Achilles tendon.
- The incision should extend distally from 3 to 4 cm proximal to the superior tuberosity of the calcaneus, down to 2 to 3 cm distal to the superior tuberosity.
- Surgical Warning: Strict adherence to a lateral approach (rather than medial) avoids the medial neurovascular bundle. However, meticulous superficial dissection is required to identify and protect the sural nerve, which crosses the lateral border of the Achilles tendon in the proximal aspect of the incision.
Exposure and Resection
- Plantar flex the ankle joint to reduce tension on the Achilles tendon. By sharp and blunt dissection, identify the lateral border of the Achilles tendon.
- Incise the paratenon longitudinally and retract it.
- Place a right-angle retractor between the anterior aspect of the Achilles tendon and the posterior/superior borders of the calcaneal tuberosity.
- With the foot held in plantar flexion, this maneuver usually affords sufficient exposure to resect the superior border of the calcaneal tuberosity without raising the Achilles tendon off its calcaneal footprint.
- Note on Tendon Reflection: The Achilles tendon has an extensive, broad insertion into the posterior and plantar aspects of the calcaneal tuberosity. If exposure is inadequate, raising a 1- to 2-cm-long portion of the tendon may be necessary to resect the bone adequately.
The Osteotomy
- Remove the superior aspect of the tuberosity (the Haglund lesion) using a microsagittal saw or a sharp broad osteotome.
- Technical Pearl: Placement of several transverse drill holes along the proposed osteotomy site creates a perforation line. This makes the resection easier and prevents the osteotomy from propagating distally into the body of the calcaneus, which could create a dangerous stress riser.
- Ensure the resection is generous. A common cause of surgical failure is under-resection of the posterosuperior prominence. The final cut should slope anteriorly and distally, leaving no sharp medial or lateral ridges that could abrade the tendon.
- Perform a thorough retrocalcaneal bursectomy, removing all inflamed synovial tissue.
Addressing Intratendinous Calcification
- If an area of ossification remains within the tendon substance, split the Achilles tendon in a coronal plane distally.
- Elevate the anterior third or half of the tendon to free up enough tissue to meticulously excise the calcified, degenerative tendon.
- Following debridement, repair the split tendon with heavy non-absorbable sutures (e.g., #2 FiberWire) using a Krackow or similar locking stitch technique. Use suture anchors to reattach any reflected portion of the tendon to the calcaneal footprint.
ADVANCED RECONSTRUCTION: FHL TENDON TRANSFER
In cases of severe, chronic Haglund syndrome with concomitant insertional Achilles tendinopathy, the surgeon may be forced to debride more than 50% of the Achilles tendon insertion to achieve healthy tissue margins. In such scenarios, the remaining Achilles tendon is biomechanically insufficient, and augmentation is required to prevent catastrophic postoperative rupture and to restore plantar flexion power.
The Flexor Hallucis Longus (FHL) tendon is the ideal transfer candidate due to its proximity, in-phase firing pattern, and robust cross-sectional area. The modified Mann technique is highly recommended for this augmentation.
FHL Harvest and Routing
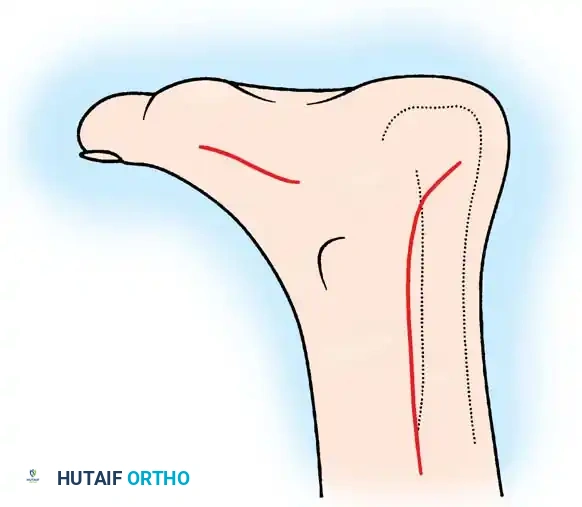
Incisions for exposure and harvest of the flexor hallucis longus tendon. A medial midfoot incision is utilized to harvest the tendon at the Master Knot of Henry, while the posterior incision is used for the calcaneal transfer.
- Medial Incision: Make a longitudinal incision along the medial arch of the foot to expose the plantar fascia and the underlying musculature.
- Identification: Dissect deeply to identify the Master Knot of Henry, where the FHL crosses dorsal to the Flexor Digitorum Longus (FDL).
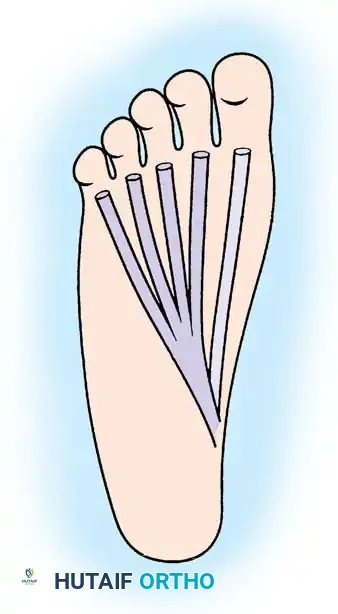
Plantar view demonstrating the anatomical relationship between the flexor digitorum longus (FDL) and the adjacent flexor hallucis longus (FHL) tendon prior to harvest.
- Harvest and Tenodesis: Transect the FHL tendon as distally as possible. To prevent loss of active interphalangeal joint flexion of the hallux, perform a tenodesis by anastomosing the distal stump of the FHL to the adjacent FDL tendon.
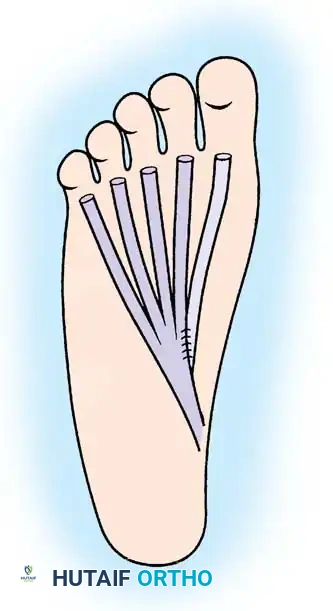
Anastomosis of the distal stump of the FHL tendon to the FDL tendon, ensuring preservation of distal toe flexion.
- Tendon Routing: Withdraw the proximal stump of the FHL tendon into the posterior ankle incision.
- Calcaneal Fixation: Drill a transverse hole through the calcaneus, anterior to the Achilles footprint. Pass the FHL tendon through this drill hole from medial to lateral.
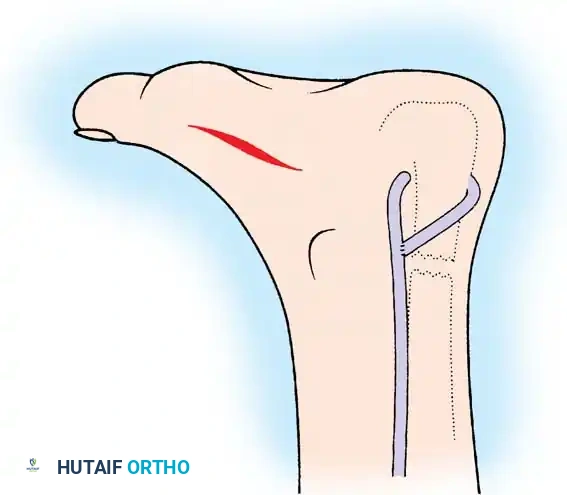
The FHL tendon is pulled through the transverse drill hole in the calcaneus and tensioned appropriately to augment plantar flexion.
- Tensioning: With the ankle held in approximately 15 to 20 degrees of plantar flexion, tension the FHL tendon and suture it back onto itself or secure it with an interference screw within the calcaneal tunnel.
Closure
- Copiously lavage the wound with sterile saline to remove all bone debris, which can cause heterotopic ossification if left behind.
- Close the paratenon meticulously over the Achilles tendon to prevent skin adhesions.
- Close the subcutaneous tissue and skin in layers using a non-strangulating technique (e.g., Allgöwer-Donati sutures) to respect the tenuous posterior heel vascularity.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management is as critical as the surgical execution, particularly given the high risk of wound breakdown and tendon rupture in the posterior heel.
Phase I: Immobilization (Weeks 0-3)
- Immediately postoperatively, apply a well-padded, short leg, non-weight-bearing (NWB) cast with the ankle immobilized in approximately 20 degrees of plantar flexion. This position minimizes tension on the Achilles tendon and the posterior skin incision.
- Strict elevation is mandated to control edema and protect the incision.
- At 3 Weeks: The cast is bi-valved, and sutures are removed. Note: Sutures may be removed earlier (at 2 weeks) if the incision is fully healed, but the non-weight-bearing cast must remain on for a full 3 weeks.
Phase II: Transitional Weight-Bearing (Weeks 3-6)
- At the 3-week mark, transition the patient into a removable controlled ankle motion (CAM) weight-bearing cast boot.
- The boot should initially be fitted with heel wedges to maintain slight plantar flexion.
- Active plantar flexion and gentle active dorsiflexion exercises are initiated out of the boot. Passive dorsiflexion stretching is strictly prohibited at this stage to protect the tendon insertion.
- Weight-bearing is advanced as tolerated in the CAM boot.
Phase III: Strengthening and Return to Function (Weeks 6-12+)
- Wean the patient from the CAM boot into a supportive athletic shoe with a slight heel lift.
- Initiate formal physical therapy focusing on eccentric strengthening, proprioception, and gait normalization.
- Return to high-impact sports or running is typically delayed until 4 to 6 months postoperatively, contingent upon the recovery of symmetrical calf strength and the absence of pain.
Preoperative Counseling Imperative: It is absolutely critical during preoperative counseling to manage the expectations of the patient. Explain clearly to a young woman presenting with a "pump bump" that it may take 3 to 6 months before she can even attempt to wear a stylish, closed-heel shoe. Furthermore, the surgeon must explicitly state that there is no guarantee she will ever be able to wear rigid-heeled footwear comfortably again. Setting these expectations prevents postoperative dissatisfaction despite a technically flawless surgery.
You Might Also Like

