Comprehensive Management of the Diabetic Foot: Ulcers, Infections, and Surgical Interventions
Key Takeaway
The management of diabetic foot complications requires a multidisciplinary approach addressing peripheral neuropathy, vascular insufficiency, and altered biomechanics. This guide details the pathophysiology, clinical evaluation, and evidence-based treatment of diabetic ulcers and infections. From total contact casting to complex surgical interventions like metatarsal head resections and tendon lengthenings, mastering these protocols is essential for limb salvage and optimizing patient outcomes in orthopedic practice.
Introduction to Diabetic Foot Complications
The management of diabetic foot complications represents one of the most challenging and resource-intensive domains within orthopedic surgery. Care for diabetic foot ulcers and their associated sequelae is estimated to cost the healthcare system over 10 billion dollars annually. Beyond the economic burden, diabetic ulcers exert a profound impact on patient quality of life. Clinical outcome scores for patients with unhealed ulcers are significantly lower than those with healed ulcers, and both cohorts score substantially lower than the general population.
Successful management demands a highly coordinated, multidisciplinary approach. The care team typically includes an orthopaedic surgeon, vascular surgeon, endocrinologist, infectious disease consultant, and a certified pedorthotist. The primary goal is limb salvage, achieved through meticulous risk assessment, offloading, infection control, and timely surgical intervention.
Clinical Pearl: The presence of a diabetic foot ulcer is a sentinel event. It is not merely a localized wound but a marker of systemic disease severity, carrying a 5-year mortality rate comparable to several aggressive malignancies.
Pathophysiology and Biomechanics
The development of a diabetic foot ulcer is rarely the result of a single pathology; rather, it is the culmination of a triad of peripheral neuropathy, biomechanical deformity, and peripheral arterial disease (PAD).
Peripheral Neuropathy
Neuropathy in the diabetic patient affects the sensory, motor, and autonomic nervous systems:
* Sensory Neuropathy: The loss of protective sensation (LOPS) means patients are unable to perceive repetitive microtrauma or undue pressure, placing the skin at severe risk of breakdown.
* Motor Neuropathy: Denervation of the intrinsic foot musculature leads to an "intrinsic-minus" foot. This muscular imbalance results in the classic claw toe and hammer toe deformities. The resulting prominent metatarsal heads and dorsal proximal interphalangeal (PIP) joints become highly vulnerable to pressure necrosis.
* Autonomic Neuropathy: Loss of sympathetic tone leads to autosympathectomy, resulting in dry, anhidrotic skin that is prone to fissuring, providing a portal of entry for bacteria. It also causes arteriovenous shunting, which bypasses the capillary beds and deprives the skin of essential nutrients.

Fixed flexion deformities of the interphalangeal joint of the hallux and proximal interphalangeal joint of the second toe. The rigid nature of these deformities exponentially increases focal plantar pressures.
Altered Biomechanics and Achilles Contracture
Equinus contracture is a critical biomechanical fault in the diabetic foot. A tight Achilles tendon limits ankle dorsiflexion, forcing the foot to compensate by increasing pressure across the forefoot during the stance phase of gait.
Furthermore, diabetes induces structural changes within the Achilles tendon itself. Non-enzymatic glycosylation of collagen leads to the disorganization of tendon fibers, advanced glycation end-product (AGE) cross-linking, and intratendinous calcification. These changes, highly prevalent in older diabetic patients, explain the profound stiffness and loss of viscoelasticity in the gastrocsoleus complex, directly contributing to forefoot ulceration.
Peripheral Vascular Disease and Altered Healing
Peripheral arterial disease increases the risk of ulceration ninefold and severely impairs healing once an ulcer occurs. Diabetic PAD typically affects the infrapopliteal vessels (tibial and peroneal arteries) while sparing the pedal vessels, a pattern distinct from atherosclerotic disease in non-diabetics.
Additionally, diabetic patients suffer from altered immune function and delayed bone healing. Defects in leukocyte chemotaxis, adherence, phagocytosis, and intracellular killing leave these patients highly susceptible to infection. Diabetics face an 80% increased risk of cellulitis, a fourfold increased risk of osteomyelitis, and double the risk of sepsis. Bone healing is also compromised; biomechanical studies demonstrate decreased fracture callus strength and reduced collagen synthesis, parameters that can be partially reversed with strict glycemic control.
Clinical Evaluation and Risk Assessment
A comprehensive clinical evaluation is paramount for risk stratification. The American Orthopaedic Foot & Ankle Society (AOFAS) outlines key risk factors, including a history of previous ulcers, prior amputations, bony deformity, and peripheral edema.
Neurologic Evaluation
Protective sensation must be evaluated using the 5.07 (10-gram) Semmes-Weinstein monofilament. Inability to detect this monofilament indicates a loss of protective sensation and a high risk for ulceration.

Evaluating protective sensation with the 5.07 Semmes-Weinstein monofilament. The filament should be applied perpendicular to the skin until it buckles.
Vascular Evaluation
Clinical signs of vascular insufficiency include absent pedal pulses, trophic skin changes (hair loss, shiny skin), and a history of claudication. Non-invasive vascular testing is mandatory. Because medial arterial calcification (Mönckeberg's sclerosis) can falsely elevate the Ankle-Brachial Index (ABI), Toe-Brachial Index (TBI) and toe systolic pressures using photoplethysmography (PPG) are more reliable indicators of pedal perfusion.

Measurement of toe systolic pressure with a manual PPG unit. A toe pressure >40 mm Hg is generally required for predictable wound healing.
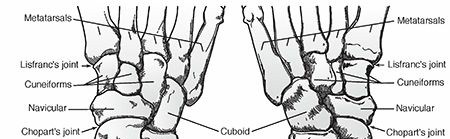
Classification of Diabetic Foot Ulcers
Accurate classification guides treatment and establishes a prognosis. The Wagner Classification is the most widely utilized system in orthopedic practice, grading ulcers based on depth and the presence of gangrene.
The Wagner Classification System
- Grade 0: Pre-ulcerative lesion, healed ulcer, or presence of bony deformity (skin at risk).
- Grade 1: Superficial ulcer without subcutaneous tissue involvement.
- Grade 2: Deep ulcer penetrating to tendon, bone, or joint capsule.
- Grade 3: Deep ulcer with abscess, osteomyelitis, or joint sepsis.
- Grade 4: Localized gangrene (e.g., forefoot or heel).
- Grade 5: Extensive gangrene involving the entire foot.

Superficial (Wagner Grade 1) ulcer. The dermis is breached, but deep structures are not exposed.

Deep (Wagner Grade 2) ulcer with exposed tendon and joint capsule. Immediate offloading and infection surveillance are required.

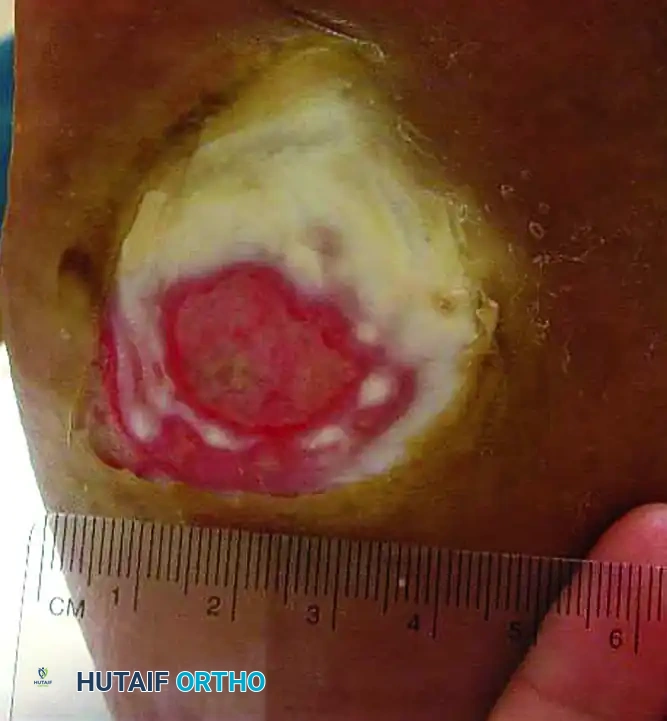
Wagner Grade 3 ulcer with underlying osteomyelitis. Note the deep tissue destruction and purulent exudate.
Surgical Warning: The University of Texas San Antonio classification system is an excellent adjunct to the Wagner system, as it incorporates ischemia and infection into a matrix grid. Higher grades in the UT system correlate more closely with prolonged healing times and the ultimate risk of amputation.
Nonoperative Management
The cornerstone of nonoperative management for plantar diabetic foot ulcers is aggressive mechanical offloading.
Total Contact Casting (TCC)
Total contact casting remains the gold standard for offloading plantar ulcers. TCC reduces plantar pressures by increasing the weight-bearing surface area and transferring loads from the foot to the lower leg (shank). It also locks the ankle in neutral, eliminating the propulsive push-off phase of gait where forefoot pressures peak.

A plantar ulcer successfully healed after 2 months of strict total contact casting.
Application of a total contact cast. Meticulous padding of bony prominences is essential to prevent iatrogenic ulceration.
For patients who cannot maintain strict non-weight-bearing status, modifications can be made. The addition of a metal stirrup extending beyond the foot-plate transmits ground reaction forces directly to the cast walls, bypassing the plantar surface entirely.
Total contact cast modified with a metal stirrup to further offload the plantar surface in ambulatory patients.
Removable Cast Walkers
Removable diabetic boots (Controlled Ankle Motion or CAM walkers) have demonstrated efficacy comparable to TCC in biomechanical offloading studies. However, clinical healing rates are often lower due to poor patient compliance. Wrapping the boot with cohesive bandages or fiberglass (rendering it "irremovable") significantly improves healing rates, underscoring that forced compliance is the primary advantage of TCC.

Removable diabetic boot. While effective for offloading, clinical success is heavily dependent on patient adherence.
Advanced Wound Therapies
- Negative Pressure Wound Therapy (NPWT): Vacuum-assisted closure promotes granulation tissue formation, reduces edema, and manages exudate. It is highly effective following surgical debridement or partial amputation, demonstrating higher healing rates and lower amputation rates compared to standard moist wound care.
- Hyperbaric Oxygen Therapy (HBOT): HBOT increases tissue oxygen tension, promoting angiogenesis and enhancing leukocyte bactericidal activity. Studies show an overall healing rate of 76% (vs. 48% in controls) and a reduced amputation rate (19% vs. 45%) when utilized for chronic, hypoxic wounds. The effect is dose-dependent, requiring >10 sessions for optimal efficacy.
- Extracorporeal Shockwave Therapy (ESWT): Emerging evidence suggests ESWT can stimulate neovascularization and cellular proliferation, proving beneficial for recalcitrant chronic ulcers.
Operative Management and Surgical Techniques
Surgical intervention is dictated by the presence of infection, the depth of the ulcer, and the underlying biomechanical deformity. According to the International Working Group on the Diabetic Foot, urgent surgical indications include necrotizing fasciitis, gas gangrene, and deep space abscesses.
Infection Management and Debridement
Empiric broad-spectrum intravenous antibiotics should be initiated immediately for infected ulcers, followed by targeted therapy based on deep intraoperative tissue cultures (superficial swabs are notoriously unreliable).
For severe infections, emergent incision and drainage (I&D) with aggressive debridement of all necrotic soft tissue and bone is mandatory. The phrase "time is tissue" is highly applicable; delayed debridement increases the risk of major limb amputation.
Management of Osteomyelitis
Chronic osteomyelitis that fails conservative management requires surgical resection. The goal is to excise all infected and non-viable bone while preserving as much functional biomechanical anatomy as possible.

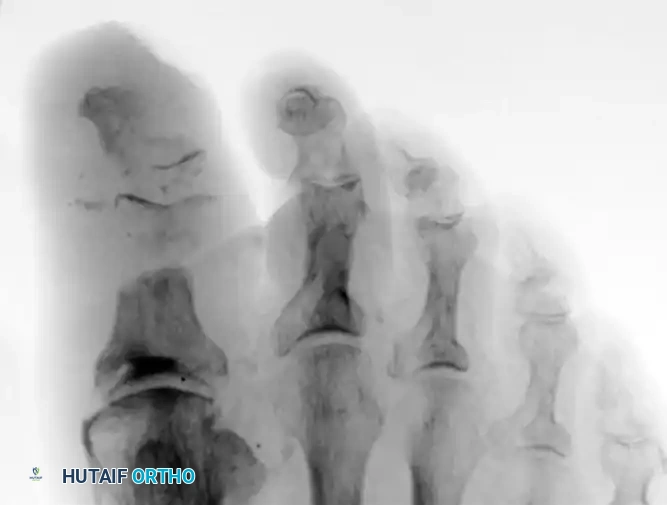
Radiograph demonstrating severe osteomyelitis and bone destruction of the metatarsophalangeal joints, necessitating surgical resection.
- Toe Amputations: For osteomyelitis isolated to the phalanges, partial or complete toe amputation is performed. Preserving the base of the proximal phalanx, when oncologically safe, helps maintain the collateral ligament complex and prevents adjacent toes from drifting into the void.
- Metatarsal Head Resection: Ulcers beneath the metatarsal heads frequently lead to localized osteomyelitis. Isolated metatarsal head resection can be curative. If multiple heads are involved, a pan-metatarsal head resection or a transmetatarsal amputation (TMA) provides a more durable, balanced stump.
- Ray Resection: If infection extends into the metatarsal shaft, a ray resection is indicated. For first ray resections, preserving the base of the first metatarsal is ideal to maintain the insertion of the peroneus longus, though this is often impossible in severe infections.
- Partial Calcanectomy: Heel ulcers complicated by calcaneal osteomyelitis are notoriously difficult to treat. A partial calcanectomy—excising the posterior and plantar aspects of the calcaneus—can eradicate the infection while salvaging the limb, avoiding a below-knee amputation (BKA).
Prophylactic and Reconstructive Surgery
To prevent ulcer recurrence, the underlying biomechanical forces must be neutralized.
* Tendon Lengthenings: Because equinus drives forefoot pressure, Achilles tendon lengthening (TAL) or gastrocsoleus recession (Strayer or Baumann procedures) is highly effective in healing recalcitrant forefoot ulcers and preventing recurrence.
* Targeted Releases: For specific focal pressures, targeted tendon releases are utilized. An intramuscular lengthening of the posterior tibial tendon can offload a fifth metatarsal head ulcer, while a Z-lengthening of the peroneus longus can reduce pressure under the first metatarsal head.
* Arthroplasty and Tenotomy: Flexible claw toe deformities causing apical toe ulcers can be treated with simple percutaneous flexor tenotomies. Rigid deformities may require PIP joint resection arthroplasty to relax the soft tissue envelope and allow the ulcer to heal.
Postoperative Protocols and Rehabilitation
Postoperative care is as critical as the surgical intervention itself. Following debridement or amputation, the foot is typically placed in a bulky, non-compressive Jones dressing or a negative pressure wound therapy device.
Strict non-weight-bearing is enforced until the surgical incisions are fully healed and sutures are removed (typically 3-4 weeks, as diabetic healing is delayed). Once the soft tissue envelope is stable, the patient is transitioned to a total contact cast or a Charcot Restraint Orthotic Walker (CROW) boot.
Long-term success relies on lifelong pedorthic management. Patients must be fitted with custom-molded, multi-density orthotics and extra-depth shoes with rigid rocker-bottom soles. The rocker-bottom sole simulates ankle dorsiflexion and metatarsophalangeal extension, effectively bypassing the foot's intrinsic joints and drastically reducing plantar peak pressures during the terminal stance phase of gait. Routine surveillance by a multidisciplinary team is mandatory to monitor the contralateral limb, which remains at an exceptionally high risk for future ulceration.
You Might Also Like