Comprehensive Surgical Management of the Diabetic Foot
Key Takeaway
The diabetic foot presents a complex triad of neuropathy, ischemia, and infection. Successful management requires a multidisciplinary approach, precise vascular assessment, and strategic surgical intervention. This guide details the pathophysiology, Wagner and Brodsky classification systems, and step-by-step operative protocols for diabetic ulcers and neuropathic deformities. Emphasizing biomechanical off-loading and meticulous debridement, it provides orthopedic surgeons with evidence-based strategies to optimize limb salvage and prevent major amputations.
Introduction to the Diabetic Foot
In the management of the diabetic foot, the orthopedic surgeon is confronted with a triad of devastating pathologies: ischemia, infection, and neuropathy. While ischemia and infection represent acute, life-threatening emergencies, neuropathy remains the most insidious and difficult condition to treat. The medical and surgical literature concerning the clinical and pathological manifestations of the diabetic foot is vast, encompassing endocrinology, vascular surgery, infectious disease, and orthopedics.
To navigate this complex clinical entity, a strictly evidence-based, multidisciplinary approach is mandatory. A comprehensive team—comprising an endocrinologist, infectious disease specialist, vascular surgeon, orthopedic surgeon, specialized nursing staff, orthotist, and podiatrist—is indispensable. The "diabetic foot in trouble" requires aggressive, coordinated care to prevent major limb amputation and reduce mortality.

Fig. 82-1 A, Feet show most severe complications of diabetes—dry, scaly skin; swelling; and venous shunting from autosympathectomy. B, Deformity from neuropathic arthropathy in midfoot with collapse of arch on left foot with prominent bony protrusions medially and plantarward; further deformity from amputation of left fourth toe because of infection. C, Fifth toe is dislocated at metatarsophalangeal joint. Great toe is clawed secondary to intrinsic muscle paralysis.
Pathophysiology: The Role of Neuropathy
Neuropathy, angiopathy, retinopathy, and nephropathy—alone or in combination—dictate the prognosis of the diabetic foot. Neuropathy manifests in three distinct forms, each contributing to the cycle of ulceration and deformity:
- Sensory Neuropathy: The loss of protective sensation (LOPS) begins distally. Vibratory and proprioceptive senses are lost early, leaving the patient unaware of the foot's position in space. Total anesthesia from the midtibia distally results in a limb that the patient dissociates from their body, leading to unrecognized repetitive microtrauma.
- Motor Neuropathy: Denervation of the intrinsic foot musculature (lumbricals and interossei) leads to an "intrinsic-minus" foot. The long flexors and extensors overpower the intrinsic muscles, resulting in fixed claw toe deformities. This biomechanical shift draws the protective plantar fat pad distally, exposing the metatarsal heads to extreme shear and vertical forces.
- Autonomic Neuropathy: Autosympathectomy results in the complete absence of sweating (anhidrosis), leading to dry, scaly, and inelastic skin that is prone to fissuring. Furthermore, loss of sympathetic tone causes arteriovenous shunting, leading to a swollen, hyperemic limb with bounding pulses, which paradoxically suffers from capillary-level ischemia.
Clinical Pearl: The combination of sensory loss (inability to feel pain), motor neuropathy (deformity causing high-pressure areas), and autonomic neuropathy (dry, easily broken skin) creates the perfect storm for diabetic ulceration.
Diagnostic Aids and Vascular Assessment
Before any surgical intervention or aggressive off-loading is initiated, a rigorous vascular assessment is paramount. The ischemic index, derived from Doppler flow pressures, serves as an essential baseline to predict both ulcer healing and the viability of limited foot amputations.
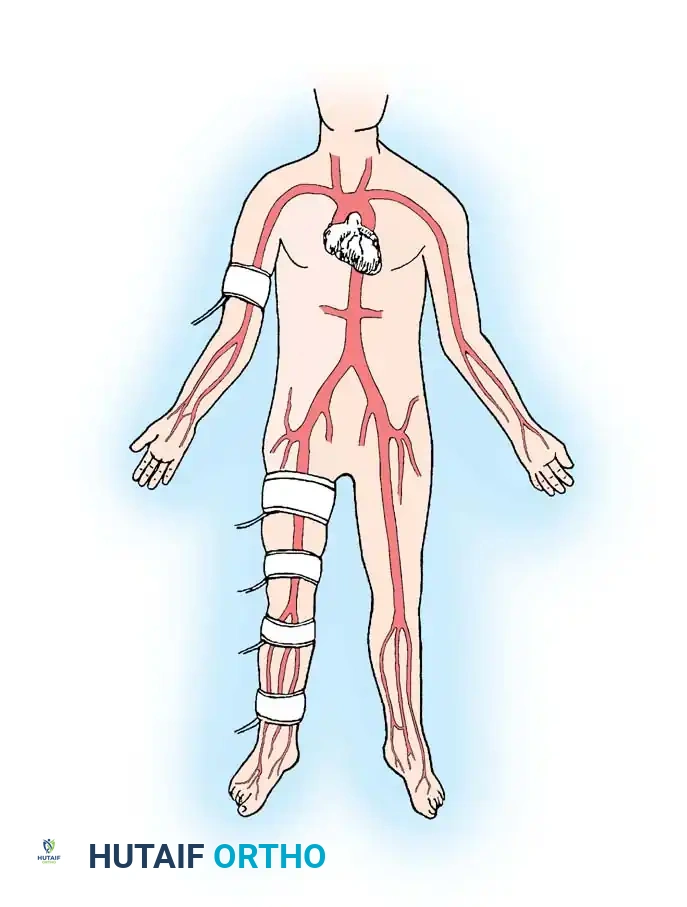
Fig. 82-6 Normal condition on right side of body with ankle systolic pressure equal to brachial systolic pressure. Ankle pressure divided by arm pressure determines ankle/arm index, in this case 1. On left side, ankle/arm index is 0.6, indicating only 60% of expected normal flow at rest. In addition, any gradient greater than 30 mm Hg between two successive cuffs indicates high-grade stenosis or occlusion.
While pulse volume recordings and transcutaneous oxygen pressures (TcPO2) are valuable, they do not replace a meticulous physical examination. It is critical to recognize that 5% to 10% of diabetic patients exhibit medial arterial calcification (Mönckeberg's sclerosis), which renders the arteries incompressible and results in falsely elevated Ankle-Brachial Index (ABI) values (e.g., ABI > 1.3).

Fig. 82-7 Measurement of posterior tibial ankle pressure and great toe pressure is shown using Doppler ultrasound device and photoplethysmography.
Predictors of Healing:
* Ischemic Index (ABI): A ratio of 0.6 or greater is generally required for healing, though values must be interpreted cautiously in the presence of calcification.
* Absolute Ankle Pressure: $\ge$ 70 mm Hg.
* Absolute Toe Pressure: $\ge$ 40 mm Hg (Toe pressures are less affected by arterial calcification and are highly reliable).
* Transcutaneous Oxygen (TcPO2): $\ge$ 30 mm Hg indicates adequate tissue perfusion for wound healing.
Surgical Warning: Never apply a total contact cast (TCC) or occlusive dressing to a foot lacking palpable pedal pulses without first obtaining comprehensive Doppler pressures and consulting a peripheral vascular surgeon. The risk of inducing gangrene in a vascularly deficient foot far outweighs the benefits of off-loading.
Diabetic Ulceration: Biomechanics and Presentation
Diabetic ulcers predominantly occur in the forefoot, specifically beneath the metatarsal heads or the interphalangeal (IP) joint of the hallux.

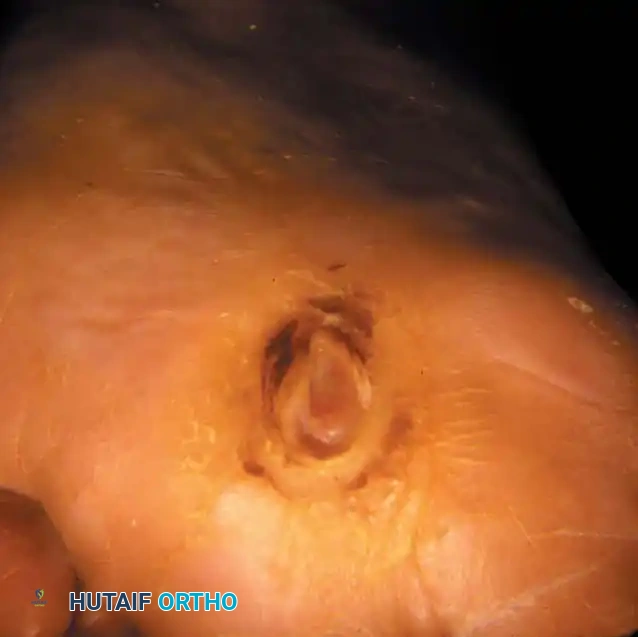
Fig. 82-2 Stage III ulcer beneath second metatarsal head that extends into metatarsal head with presumptive contiguous osteomyelitis.

Fig. 82-3 Diabetic patient with peripheral neuropathy and ulcer at interphalangeal joint of hallux is especially refractory to treatment, even in cast. After ulcer has healed, reulceration is common despite stringent pedorthic care.
The pathogenesis is deeply rooted in biomechanical dysfunction. Fixed clawing of the toes, secondary to intrinsic muscle paralysis, forces the metatarsal heads plantarward. This is particularly devastating beneath the first metatarsal head, where the sesamoid bones lie just beneath the skin, creating massive shear forces during the terminal stance phase of gait.

Fig. 82-4 Patient with diabetes mellitus and neuropathy had severe claw toes, and shear forces across plantar surface of first metatarsal head caused recurrent ulceration.
In approximately 30% of patients with plantar forefoot ulcerations, atherosclerosis of the tibial and peroneal arteries significantly prolongs healing time. Recurrent infections and progressive deformities often necessitate multiple toe amputations or transmetatarsal amputations.

Fig. 82-5 Patient with diabetes had arteriosclerotic and neuropathic involvement of foot. Ischemic index was 0.6. Because of recurrent infections and deformities, patient had multiple toes on left amputated and transmetatarsal amputation on right with primary healing.
Classification of Diabetic Ulcers
Standardized classification systems are vital for establishing a prognosis and formulating a treatment algorithm. The two most widely utilized systems in orthopedic surgery are the Wagner Classification and the Brodsky Classification.
The Wagner Classification System
Wagner developed a comprehensive grading system based on the depth of penetration and the presence of gangrene or infection:
- Grade 0: Skin intact, but bony deformities produce a "foot at risk." Preulcerative lesions may be present.
- Grade 1: Localized, superficial ulcer involving full skin thickness but not underlying tissues.
- Grade 2: Deep ulcer penetrating to tendon, bone, ligament, or joint capsule.
- Grade 3: Deep abscess, osteomyelitis, or pyarthrosis.
- Grade 4: Gangrene of toes or forefoot.
- Grade 5: Gangrene of the entire foot.

Fig. 82-8 Collapsed midfoot in patient with diabetic neuroarthropathy and preulcerative lesion (Wagner Grade 0).

Fig. 82-9 A, Localized superficial ulcer treated in cutoff postoperative shoe. B, Six weeks in shoe (Wagner Grade 1).

Fig. 82-10 A, Fibrinous bed to deep ulcer over metatarsal head. Second metatarsophalangeal joint was dislocated, plantar plate disrupted, and bone and tendon exposed (Wagner Grade 2/3).
The Brodsky Classification System
Brodsky introduced a classification that specifically excludes gangrene, focusing purely on the depth of the neuropathic ulcer:
* Depth 0: Intact skin, representing a preulcerative lesion with erythema, callus formation, and possible intradermal shear hemorrhage over a bony prominence.
* Depth I: Superficial, full-thickness skin ulcer down to, but not through, the subcutaneous tissue.
* Depth II: Ulceration extending to the tendon and joint capsule, but bone/joint is not visible.
* Depth III: Exposed bone or joint, implying contiguous osteomyelitis or pyarthrosis.
Surgical Management and Operative Techniques
Surgical intervention in the diabetic foot is indicated for the eradication of infection, correction of unbraceable deformities, and prophylactic off-loading of recurrent ulcerations.
1. Preoperative Optimization
- Glycemic Control: Optimize HbA1c to < 7.5% if possible, though acute infections require immediate surgery regardless of glycemic status.
- Infection Control: Obtain deep tissue cultures (not superficial swabs) for targeted antibiotic therapy. Broad-spectrum empiric antibiotics should be initiated immediately in the presence of systemic toxicity or deep abscess.
- Vascular Clearance: Ensure adequate perfusion (Toe pressure > 40 mmHg) prior to elective deformity correction.
2. Debridement and Exostectomy
For Grade 2 and Grade 3 ulcers, aggressive surgical debridement is the cornerstone of therapy. The goal is to convert a chronic, contaminated wound into an acute, clean wound.

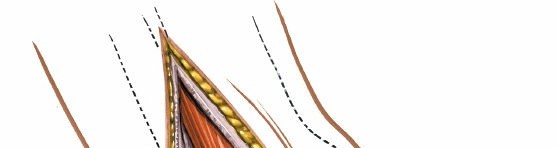
Surgical Diagram: Excision of necrotic tissue and underlying bony prominences.
Surgical Steps:
1. Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg, providing clear access to the plantar aspect of the foot.
2. Incision: Extend the ulcer longitudinally to expose the underlying pathology. Avoid transverse incisions on the plantar weight-bearing surface.
3. Soft Tissue Debridement: Excise all hyperkeratotic margins, fibrotic tissue, and necrotic fascia until healthy, bleeding tissue is encountered.
4. Bone Resection (Exostectomy): If a metatarsal head or sesamoid is the source of the pressure point, it must be resected. Use an oscillating saw or rongeur to perform a partial or complete metatarsal head resection. Bevel the remaining bone dorsally to prevent a new plantar pressure point.
5. Irrigation: Copious pulsatile lavage with normal saline.
6. Closure: Leave the wound open to heal by secondary intention, or apply a negative pressure wound therapy (NPWT) device. Primary closure is contraindicated in the presence of active infection.
Surgical Diagram: Deep debridement extending to the joint capsule and bone.
3. Achilles Tendon Lengthening (ATL)
Equinus contracture is a major contributor to elevated forefoot plantar pressures. An Achilles tendon lengthening is frequently performed adjunctively to off-load forefoot ulcers.
Surgical Steps (Percutaneous Hoke Method):
1. Patient prone or supine with the knee extended.
2. Make three stab incisions: the first medially just proximal to the calcaneal insertion, the second laterally 2-3 cm proximal to the first, and the third medially 2-3 cm proximal to the second.
3. Dorsiflex the foot forcefully to snap the remaining intact fibers, achieving 10-15 degrees of dorsiflexion.
4. Immobilize in a short leg cast for 6 weeks.
4. Amputations
When tissue loss is extensive, osteomyelitis is diffuse, or vascular reconstruction has failed, amputation becomes necessary. The goal is to preserve as much functional length as possible while ensuring primary healing.
- Toe Amputation: Indicated for localized gangrene or osteomyelitis of the phalanx. Use a racquet-shaped incision, preserving the plantar flap if possible.
- Ray Amputation: Indicated for infection involving the MTP joint. Resect the metatarsal shaft at the metaphyseal-diaphyseal junction. Be cautious with first ray amputations, as they significantly alter foot biomechanics and increase the risk of transfer ulcers to the lesser metatarsals.
- Transmetatarsal Amputation (TMA): An excellent definitive procedure for extensive forefoot gangrene. A long plantar flap is utilized to cover the distal metatarsal stumps. The Achilles tendon must often be lengthened simultaneously to prevent equinus and subsequent distal stump ulceration.
Postoperative Protocols and Off-Loading
The success of any surgical intervention in the diabetic foot hinges entirely on postoperative biomechanical management.
Total Contact Casting (TCC)
The Total Contact Cast is the gold standard for off-loading plantar neuropathic ulcers (Wagner Grades 1 and 2). It works by increasing the weight-bearing surface area, thereby reducing peak pressures under the metatarsal heads by up to 30%.
Application Principles:
* Apply a thin layer of stockinette and minimal padding (only over bony prominences) to ensure intimate contact between the cast and the leg.
* Mold the fiberglass carefully around the malleoli and the arch.
* The cast must be changed every 1 to 2 weeks to accommodate reductions in edema and to inspect the wound.
* Contraindications: Active deep infection, severe ischemia (ABI < 0.45), or patient non-compliance.
Pedorthic Management
Once the ulcer has healed, the skin remains fragile and the biomechanical forces that caused the initial ulcer are still present. Lifelong pedorthic care is mandatory.

Surgical Diagram: Postoperative shoe modifications and off-loading orthotics.
Footwear Modifications:
* Extra-Depth Shoes: To accommodate claw toe deformities and custom orthotics.
* Custom Molded Inserts: Fabricated from plastazote or similar materials to distribute pressure evenly.
* Rocker Bottom Soles: To eliminate the propulsive phase of gait, drastically reducing shear forces across the metatarsal heads.
* Rigid Shanks: To prevent bending of the shoe at the MTP joints.
Clinical Pearl: The phrase "healed diabetic ulcer" is a misnomer. The correct terminology is "ulcer in remission." Without stringent, lifelong adherence to custom footwear and daily foot inspections, the recurrence rate of diabetic foot ulcers approaches 50% within the first year.
Conclusion
The management of the diabetic foot requires a profound understanding of its underlying pathophysiology, meticulous clinical and vascular evaluation, and precise surgical execution. By adhering to established classification systems, aggressively debriding non-viable tissue, correcting biomechanical deformities, and enforcing strict postoperative
📚 Medical References
- diabetic foot care during the 1980s: prognostic determinants for major amputation, J Diabetes Compl 12:96, 1998.
- Finsen V, Persen L, Lovlien M, et al: Transcutaneous electrical nerve stimulation after major amputation, J Bone Joint Surg 70B:109, 1988.
- Fisher A, Meller Y: Continuous postoperative regional analgesia by nerve sheath block for
You Might Also Like