Congenital Vertical Talus: Comprehensive Surgical Management and Techniques
Key Takeaway
Congenital vertical talus (CVT) is a rigid pediatric foot deformity characterized by a fixed dorsal dislocation of the navicular on the talar head. This comprehensive guide details the clinical presentation, radiographic diagnosis, and age-specific surgical interventions, including single-stage open reduction, the Kumar technique, and Grice-Green extraarticular subtalar fusion. Early recognition and meticulous surgical realignment are critical to restoring foot biomechanics and preventing long-term disability.
CONGENITAL VERTICAL TALUS: PATHOLOGY AND BIOMECHANICS
Congenital vertical talus (CVT), frequently referred to as "rocker-bottom flatfoot" or congenital rigid flatfoot, is a severe, rigid pediatric foot deformity characterized by a fixed dorsal dislocation of the navicular on the head of the talus. It is imperative that the orthopedic surgeon distinguishes this rigid, pathologic entity from the flexible pes planus commonly observed in normal infant development.
While CVT may present as an isolated, idiopathic congenital anomaly, it is frequently teratologic, associated with numerous neuromuscular and genetic disorders. Common syndromic associations include arthrogryposis multiplex congenita, myelomeningocele, spinal muscular atrophy, and neurofibromatosis.
Pathoanatomy and Adaptive Changes
The primary pathoanatomic lesion in CVT is the rigid dorsal dislocation of the talonavicular joint. The biomechanical cascade resulting from this dislocation is profound:
* The Talus: The talus is forced into a severe equinus (plantarflexed) and medialized position, rendering it almost vertical. Its longitudinal axis aligns nearly parallel to the tibia.
* The Calcaneus: The calcaneus is also held in equinus, though to a lesser degree than the talus, and is displaced posteriorly.
* The Midfoot and Forefoot: The forefoot is rigidly dorsiflexed and abducted at the midtarsal joints. The navicular rests on the dorsal aspect of the talar neck and head.
As the child develops and begins weight-bearing, severe adaptive osseous and soft-tissue changes occur. The talus assumes an "hourglass" shape due to abnormal compressive forces, and only the posterior third of its superior articular dome articulates with the tibial plafond. The anterior plantar surface of the calcaneus becomes rounded.
Clinical Pearl: In long-standing CVT, the posterior tibial and peroneus longus and brevis tendons subluxate anterior to the malleoli. In this perverted anatomic position, they act as paradoxical dorsiflexors rather than plantarflexors, further exacerbating the rigid rocker-bottom deformity.
CLINICAL AND RADIOGRAPHIC EVALUATION
Clinical Presentation
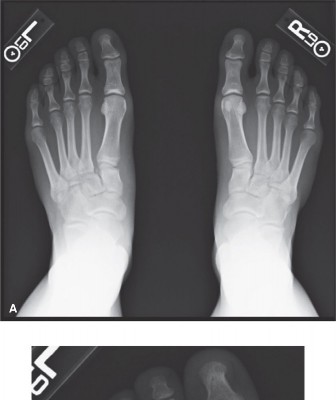
CVT is typically detectable immediately at birth. The pathognomonic clinical presentation includes a convex plantar surface (rocker-bottom sole) and a rigid, rounded prominence on the medial and plantar aspect of the midfoot, which represents the uncovered, vertically oriented head of the talus.

Deep skin creases are characteristically present on the dorsolateral aspect of the foot, anterior and inferior to the lateral malleolus, indicating severe dorsal soft-tissue contracture. When the child attempts to bear weight, the forefoot is driven into severe abduction, and the heel remains suspended off the floor due to the rigid hindfoot equinus. Callosities rapidly develop beneath the anterior calcaneus and the prominent medial talar head.

Radiographic Diagnosis
Differentiating CVT from severe but flexible pes planus or oblique talus requires rigorous radiographic evaluation. Standard weight-bearing (or simulated weight-bearing in infants) anteroposterior (AP) and lateral radiographs are required. However, the definitive diagnostic view is the plantar flexion lateral stress radiograph.
- Normal Foot / Flexible Pes Planus: On a plantar flexion lateral view, the long axis of the first metatarsal aligns with or passes plantarward to the long axis of the talus, indicating that the talonavicular joint is reducible.
- Congenital Vertical Talus: On the plantar flexion lateral view, the long axis of the first metatarsal remains rigidly dorsal to the long axis of the talus. This confirms the irreducible dorsal dislocation of the midfoot and forefoot on the hindfoot.
Surgical Warning: Failure to obtain a forced plantar flexion lateral radiograph can lead to misdiagnosis of an oblique talus as a true vertical talus, potentially resulting in unnecessary or overly aggressive surgical intervention.
TREATMENT ALGORITHM
Congenital vertical talus is notoriously difficult to correct and carries a high risk of recurrence. While conservative management alone is rarely curative, it plays a vital preparatory role.
Conservative Management
Initial treatment consists of gentle serial manipulation and cast immobilization (similar to the Ponseti method, but with reverse mechanics). The goal is to stretch the contracted dorsal skin, fibrous tissues, and extensor tendons. While this rarely achieves anatomic reduction of the talonavicular joint, it significantly reduces the extent of soft-tissue release required during subsequent open surgery and minimizes the risk of postoperative wound necrosis.
Age-Specific Surgical Indications
The definitive treatment for CVT is surgical, with the specific procedure dictated by the patient's age and the rigidity of the deformity:
* 1 to 4 Years: Open reduction and realignment of the talonavicular and subtalar joints (e.g., Kumar technique). In severe teratologic cases in children over 3 years old, navicular excision may occasionally be required to decompress the lateral column.
* 4 to 8 Years: Open reduction combined with an extraarticular subtalar arthrodesis (Grice-Green procedure) to maintain hindfoot correction.
* >12 Years: Triple arthrodesis is the procedure of choice for permanent correction of the rigid, symptomatic deformity in adolescents.
SURGICAL TECHNIQUES
Single-Stage Correction (Kodros and Dias)
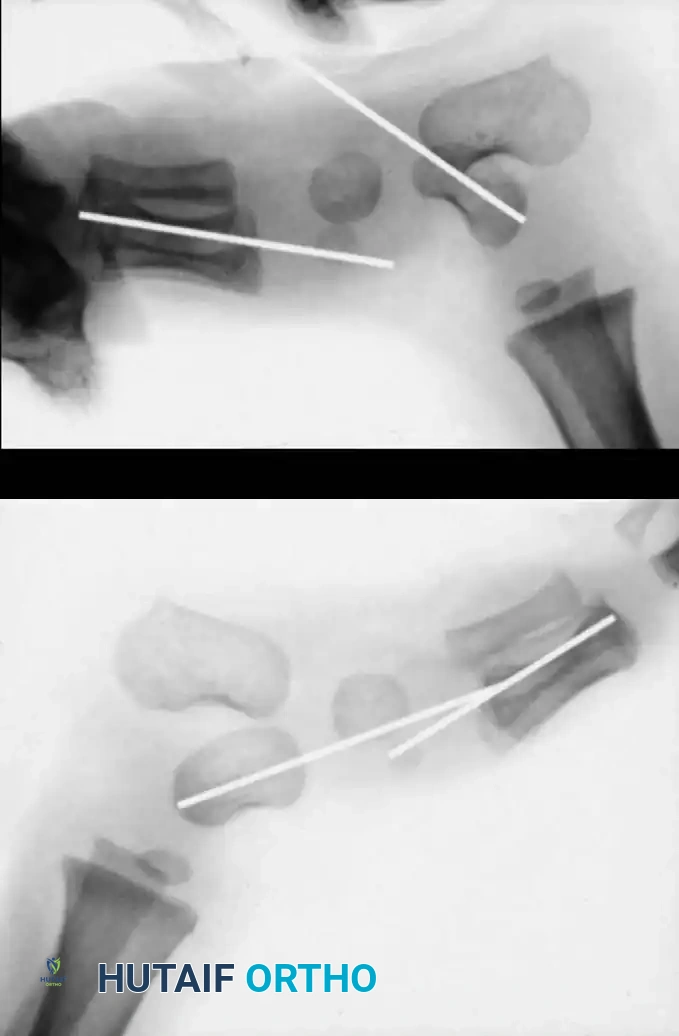
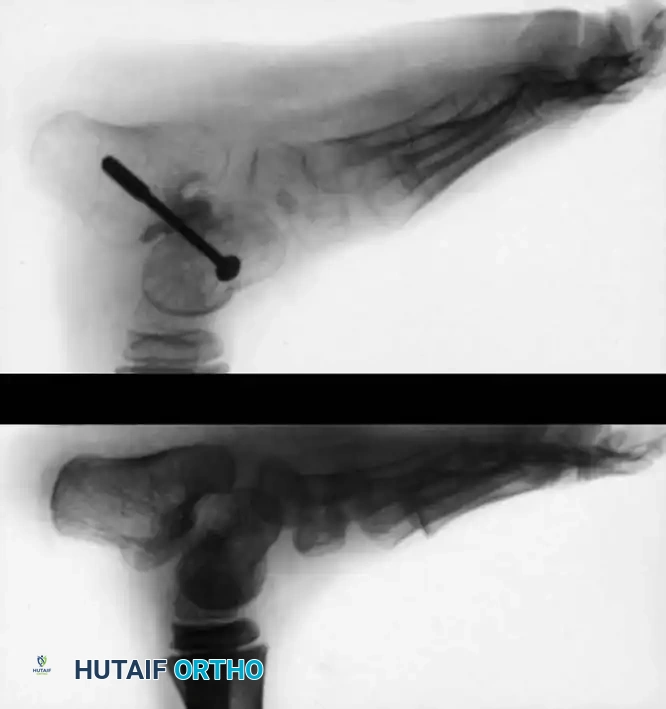
For infants and young children, a single-stage minimally invasive or limited-open approach has gained traction. Kodros and Dias described a highly effective technique utilizing a threaded Kirschner wire (K-wire) as a "joystick" to manipulate the vertical talus into an anatomic position.
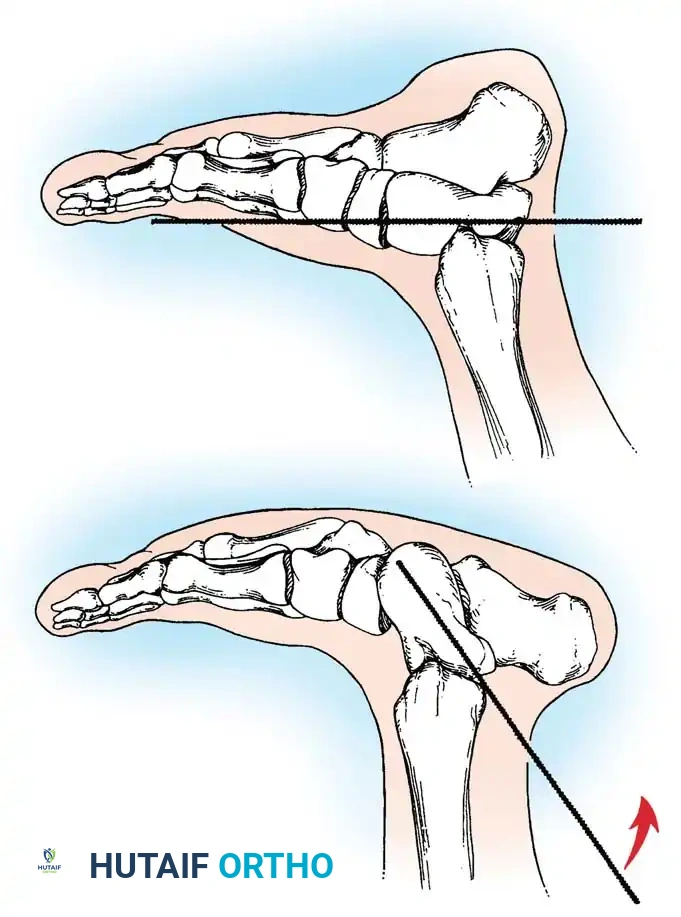
Technique Overview:
1. A threaded K-wire is introduced axially into the vertical talus from a posterior approach.
2. The wire is utilized as a joystick to lever the talus out of equinus and medial deviation, elevating the talar head.
3. Simultaneously, the forefoot is plantarflexed and inverted to reduce the navicular onto the talar head.
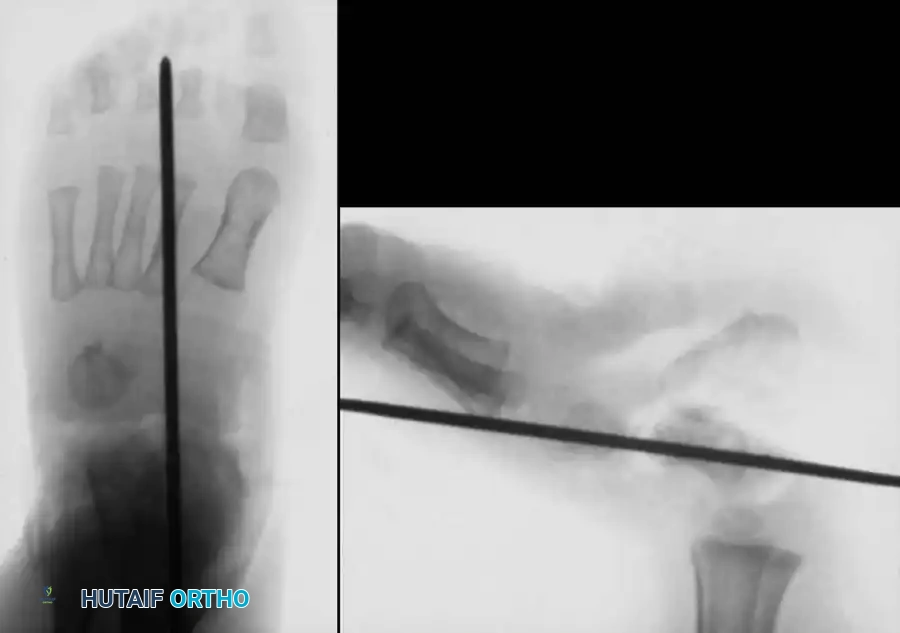
4. Once anatomic reduction is confirmed fluoroscopically, the K-wire is advanced across the talonavicular joint to secure the reduction. Additional wires may be placed across the subtalar joint.
Outcomes: Mazzocca et al. demonstrated that a single-stage dorsal approach yields significantly shorter operative times, superior clinical scores, and fewer complications compared to traditional extensive posterior or combined approaches.
Open Reduction and Realignment (Kumar, Cowell, and Ramsey)
For mild to moderate deformities in young children (1-4 years), the comprehensive soft-tissue release and realignment technique described by Kumar, Cowell, and Ramsey is the gold standard.
Incision and Exposure:
* The procedure can be performed via three separate incisions (lateral sinus tarsi, medial talar head, and posteromedial Achilles) or through a single transverse circumferential (Cincinnati) approach. The Cincinnati approach is highly preferred as it provides unparalleled, simultaneous access to the medial, posterior, and lateral peritalar structures.
Step-by-Step Surgical Execution:
1. Lateral Release: Expose the extensor digitorum brevis and reflect it distally to visualize the anterior subtalar joint. Identify the calcaneocuboid joint and perform a thorough release of all contracted structures, including the calcaneocuboid ligament and the bifurcate ligament.
2. Medial Release: Expose the prominent head of the talus and the medial aspect of the navicular. Isolate the anterior tibial tendon; if severely contracted, perform a Z-plasty lengthening.
3. Talonavicular Mobilization: Release all tight structures on the medial and dorsal aspects of the talonavicular joint. Circumferentially free the anterior talus from its ligamentous attachments to the navicular and calcaneus. This requires transection of the dorsal talonavicular ligament, the plantar calcaneonavicular (spring) ligament, and the anterior fibers of the superficial deltoid ligament.
4. Subtalar Release: If the talus remains rigidly fixed, partially divide the talocalcaneal interosseous ligament until the talus can be easily manipulated with a blunt elevator.
5. Extensor Tendon Management: If the peroneal tendons, extensor hallucis longus (EHL), and extensor digitorum longus (EDL) remain bowstrung and contracted, perform Z-plasty lengthenings.
6. Posterior Release: Perform a Z-plasty lengthening of the Achilles tendon. Perform a comprehensive posterior capsulotomy of both the ankle and subtalar joints to correct the hindfoot equinus.
7. Reduction and Fixation: Manipulate the talus and calcaneus into their corrected anatomic positions. Plantarflex and invert the forefoot to reduce the navicular onto the talar head. Pass a smooth, stout Steinmann pin or K-wire retrograde through the navicular and into the center of the talar neck to rigidly maintain the reduction.
Closure and Postoperative Protocol:
* Attempt to imbricate and reconstruct the redundant plantar talonavicular (spring) ligament to support the talar head.
* Close the wound meticulously in layers to avoid skin necrosis.
* Apply a well-padded long leg cast with the knee flexed 90 degrees, the ankle in neutral dorsiflexion, and the foot in slight inversion.
* Aftertreatment: The initial cast and Steinmann pin are removed at 8 weeks under anesthesia. A new long leg cast is applied for 1 month, followed by a short leg walking cast for an additional month. A rigid ankle-foot orthosis (AFO) is mandated for 3 to 6 months thereafter to prevent recurrence.
Open Reduction and Extraarticular Subtalar Fusion (Grice-Green)
For older children (4 to 8 years) presenting with severe, neglected, or recurrent CVT, soft-tissue realignment alone is insufficient due to adaptive bony changes. Coleman et al. popularized combining the open reduction technique with a Grice-Green extraarticular subtalar arthrodesis to provide a permanent osseous block to talar plantarflexion.
Surgical Technique:
1. Exposure: Make a short curvilinear incision over the lateral aspect of the foot, directly overlying the sinus tarsi.
2. Preparation of the Sinus Tarsi: Incise the cruciate ligament in the direction of its fibers. Evacuate the fat pad and ligamentous debris from the sinus tarsi. Reflect the extensor digitorum brevis distally.
3. Hindfoot Reduction: Place the foot in equinus and invert it to mechanically lever the calcaneus directly beneath the talus, correcting the valgus and equinus deformity. In severe cases, a posterior subtalar capsulotomy or limited lateral calcaneal ostectomy may be required to achieve reduction.
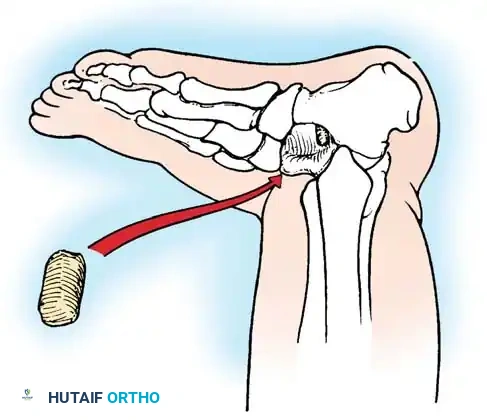
4. Graft Bed Preparation: Insert a broad periosteal elevator into the sinus tarsi to block the subtalar joint in its corrected position and determine the required graft dimensions. Prepare the recipient beds by decorticating a thin layer of cortical bone from the inferior surface of the talar neck and the superior surface of the anterior calcaneus.

- Graft Harvest and Insertion: Harvest a cortical bone block (typically 3.5 to 4.5 cm long and 1.5 cm wide). The anteromedial proximal tibial metaphysis is the traditional donor site, though a segment of the distal fibula or a tricortical iliac crest graft provides excellent structural support. Shape the graft with a rongeur to allow it to be countersunk into the cancellous beds, preventing lateral extrusion.
- Fixation: With the foot held in slight overcorrection, impact the graft into the sinus tarsi. Evert the foot slightly to lock the graft under compression.
Surgical Pearl (Dennyson and Fulford Modification): To prevent graft dislodgement and increase fusion rates, utilize rigid internal fixation. Pass a cancellous screw anteriorly from the dorsal talar neck, through the graft, and into the body of the calcaneus.
- Equinus Correction: Once the subtalar joint is stabilized by the graft, assess ankle dorsiflexion. Perform a percutaneous or open Achilles tendon lengthening to correct residual ankle equinus.
- Immobilization: Apply a long leg cast with the knee flexed, the ankle in maximal safe dorsiflexion, and the hindfoot in neutral.
COMPLICATIONS AND ASSOCIATED PATHOLOGIES
Recurrence and Overcorrection
The most common complication of CVT surgery is undercorrection or recurrence of the deformity, particularly in syndromic patients (e.g., arthrogryposis). Conversely, overzealous release of the plantar structures and over-lengthening of the Achilles tendon can result in a calcaneocavus deformity or a dorsal bunion.

Associated Tibial Deformities
Surgeons must evaluate the entire lower extremity in patients with CVT. Posterior angular deformities of the tibia are occasionally noted but generally remodel and improve with skeletal growth. Limb-length discrepancies are common and require annual radiographic surveillance; appropriately timed epiphysiodesis or distraction osteogenesis may be necessary.
Pitfall: Anterior angular deformities of the tibia associated with CVT are highly concerning. They carry a strong association with congenital pseudarthrosis of the tibia (CPT). If radiographs reveal any narrowing or sclerosis of the medullary canal (the "high-risk tibia"), prophylactic bracing is mandatory until skeletal maturity is achieved to prevent catastrophic fracture and nonunion.
Postoperative Outcomes
Long-term outcomes depend heavily on the etiology of the CVT. Idiopathic cases treated early with meticulous single-stage or Kumar open reductions generally yield functional, plantigrade, and pain-free feet.

However, teratologic cases, particularly those associated with neural tube defects, have a significantly higher rate of revision surgery. In a long-term follow-up by Kodros and Dias, nearly 25% of feet required subsequent operations at an average of 7 years post-surgery, the majority of which were in patients with underlying myelomeningocele. Continuous multidisciplinary follow-up is essential for these complex pediatric patients.
📚 Medical References
- Becker-Andersen H, Reimann I: Congenital vertical talus: reevaluation of early manipulative treatment, Acta Orthop Scand 45:130, 1974.
- Coleman SS, Martin AF, Jarrett J: Congenital vertical talus: pathogenesis and treatment, J Bone Joint Surg 48A:1442, 1966.
- Coleman SS, Stelling FH III, Jarrett J: Congenital vertical talus: pathomechanics and treatment, Clin Orthop Relat Res 70:62, 1970.
- Dennyson WG, Fulford GE:
You Might Also Like